Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Cancer immunotherapy wikipedia , lookup
Molecular mimicry wikipedia , lookup
Hygiene hypothesis wikipedia , lookup
Psychoneuroimmunology wikipedia , lookup
Atherosclerosis wikipedia , lookup
Adoptive cell transfer wikipedia , lookup
Innate immune system wikipedia , lookup
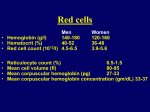
Anemic syndrome Anca Bacârea, Alexandru Schiopu Hematopoiesis Hematopoiesis is the process by which mature blood cells are generated and functional, assuming the existence of cells of origin who have a long series of transformations and hematopoetic microenvironment (composed of stromal cells and stimulating factors). Bone marrow (BM) is the central component generating blood cells: red cells, granulocytes, monocytes, lymphocytes, platelets and hematopoietic functions are proliferation, differentiation and cell release into circulation. BM consists of: reticulovascular stroma (with supporting role, nutrition and movement of hematopoietic cells); medullar parenchyma - composed of active cells forming islands of hematopoiesis, usually arranged around a trophic cell - "nurse cell." Nurse cells are involved in erythropoiesis (iron stores) in myelopoesis and megacaryopoesis (liberate stimulating factors e.g.. IL-3). Hematopoiesis Pluripotent stem cells (PSCs) are the cells of origin of all blood cells. Anemic syndrome Definition Anemic syndrome is defined as a poly-etiologic syndrome characterized by decrease in circulating hemoglobin (Hb) below the normal values. Anemic syndrome Adults (>15 years) Hb (g/dl) Hb (mmol/l) Women 12.0 7.4 Men 13.0 8.1 Children Hb (g/dl) Hb (mmol/l) Children < 5 years 11.0 7,1 Children < 15 years 12.0 7.4 Signs and symptoms Presence of a history of bleeding (not in all cases) Dyspnea (initial effort) Pallor Dizziness Low grade fever Compensatory hemodynamic syndrome Tachycardia Murmurs Palpitations Low blood pressure Signs and symptoms Ventilatory changes Polipnea Changes in the peripheral nervous system's activity caused by neuronal hypoxia: Paresthesia Neurovegetative dystonia Changes of reflexes Positive Babinski sign Ataxia Sphincter incontinence Changes of the senses Signs and symptoms Changes in the central nervous system activity - driven by neuronal hypoxia: Fatigue Asthenia Irritability Decreased ability to concentrate Insomnia Depression, suicide - Vitamin deficiency anemia. B12 Paranoia - Vitamin deficiency anemia. B12 Hallucinations - Vitamin deficiency anemia. B12 Psychosis - Vitamin deficiency anemia. B12 Panic Attacks - Vitamin deficiency anemia. B12 Changes in personality - Vitamin deficiency anemia. B12 Decreased muscle strength - Vitamin deficiency anemia. B12 Impotence - Vitamin deficiency anemia. B12 Signs and symptoms Trophic disorders of the mucous membranes Glossitis Esophagitis Gastritis Dyspepsia Trophic disorders of the skin and appendages Brittle hair Digital hypocratism (hippocratic fingers) Pigmentation of the skin Leg ulcers Bone pain Classification A. Anemia caused by decreased production of red blood cells B. Anemia caused by lost of red blood cells C. Anemia caused by combined mechanisms A. Anemia caused by decreased production of red blood cells 1. Involvement of hematogenous bone marrow (BM): a. Destructive processes: Physical factors: ionizing radiation Chemical factors: drugs (cytostatics, anti-inflammatory phenylbutazone, chloramphenicol, phenytoin), industrial benzene, insecticides; Biological factors: some viruses (Epstein - Barr virus, hepatitis C, parvovirus infection, human immunodeficiency virus); Immune diseases: timom, graft versus host reaction, eosinophilic fasciitis; Unknown etiology A. Anemia caused by decreased production of red blood cells 1. Involvement of hematogenous bone marrow (BM): b. Bone marrow infiltrative processes: Tumours of the bone marrow (BM): leukemia, lymphoma, multiple myeloma (MM) Metastases in BM Sarcoidosis Bone marrow fibrosis Storage diseases (glicogenoze, lipidosis - Gaucher disease) Bone marrow necrosis Bone marrow infections: sepsis, miliary tuberculosis, fungal infections A. Anemia caused by decreased production of red blood cells 1. Involvement of hematogenous bone marrow (BM): c. Low production of erythropoietin: Anemia of chronic disease (chronic inflammation, chronic infections, cancers) - inflammatory cytokines (IL1, IL 6, TNF-α) suppresses the synthesis of erythropoietin and erythropoietin increases resistance to the action; Kidney disease - chronic renal insufficiency - insufficient production of erythropoietin due to renal lesions; Liver disease - by parenchymal liver failure (cirrhosis, hepatice, toxic hepatitis, chronic aggressive hepatitis, etc.) - It reduces the synthesis of erythropoietin and hemoglobin precursors; Poliglandular hypofunction - production of erythrocytes is influenced by thyroid hormones, testosterone, glucocorticoids. A. Anemia caused by decreased production of red blood cells 2. Deficiency of forming factors: a. Protein deficiency: Low protein intake Malnutrition - starvation, low protein in food; Maldigestion - exocrine pancreatic insufficiency, bile salt deficiency, gastrectomy; Malabsorption - intestinal resection, bacterial diarrheal diseases, viral (excluding the time of contact of food with intestinal mucosa), intestinal parasites; The reduced synthesis of proteins - parenchymal liver insufficiency; The additional consumption of protein - "trap" of protein in endstage of cancer; Increased protein loss - diarrheal diseases, burns, nephrotic syndrome; A. Anemia caused by decreased production of red blood cells 2. Deficiency of forming factors: b. Lack of synthesis of purine and pyrimidine derivatives (nucleic acids, macroergic phosphates) Lack of vitamin B12 Lack of folic acid (B9) Other vitamin deficiencies - deficiency of fat soluble vitamins (A, D, K, E, F), lack of water-soluble vitamins - B thiamine (B1), riboflavin (B2), niacin (B3), pirodoxina (B6), pantothenic acid (B5), biotin (B7); c. Caused by iron deficiency anemia (iron deficiency anemia) Loss of blood Low intake Increased needs Iron metabolism disorders B. Anemia caused by lost of red blood cell mass 1. Bleeding or iatrogenic emissions of blood 2. Increased destruction of erythrocytes - hemolytic syndrome (prehepatic jaundice) a. Extracorpusculare causes: Physical factors Mechanical Mechanical cardiac causes hemolytic anemia (acquired or congenital) - aortic stenosis, coarctation of the aorta, mitral insufficiency, aortic aneurysm, heart valves; Thermal – heat Ultrasound Radiation - ultraviolet (photodermatosis), high-energy ionizing radiation; B. Anemia caused by lost of red blood cell mass 2. Increased destruction of erythrocytes - hemolytic syndrome (prehepatic jaundice) a. Extracorpusculare causes: Chemical factors Exogenous - arsenic, copper, lead, etc.. Endogenous - hemolytic anemia in nitrogen retention (renal failure); Biological factors Parasites - Malaria (Plasmodium falciparum), babesiosis (Babesia genus) Bacteria - bacterial toxins (Clostridium, E. Coli, Streptococci) Viruses (Epstein Bar, herpes encephalitis virus); Toxic - venoms (snake, scorpion, spider) B. Anemia caused by lost of red blood cell mass 2. Increased destruction of erythrocytes - hemolytic syndrome (prehepatic jaundice) a. Extracorpusculare causes: Autoimmune hemolytic anemia Hypersplenism Removal of damaged erythrocytes Response to bacterial, viral, parasitic Autoimmune diseases Metabolic diseases Tumors Hemolytic anemia with combined mechanisms - vascular coagulation (DIC) DIC is a clinical syndrome (infections, cancers, venoms, autoimmune diseases, trauma, burns, etc. obsterticale cases.) characterized by intravascular coagulation, with the formation of thrombosis and necrosis, accompanied by secondary fibrinolysis and consumption of coagulation factors, with bleeding. B. Anemia caused by lost of red blood cell mass 2. Increased destruction of erythrocytes - hemolytic syndrome (prehepatic jaundice) b. Corpuscular causes: Metabolic - enzyme deficiency: At the level of glycolysis - glucose 6-phosphate dehydrogenase (G6PDH) deficiency, pyruvate kinase deficiency, etc. In the cycle of glutathione - glutathione synthetase deficiency, glutathione reductase deficiency; Lack of heme synthesis (porphyrias) Lack of globin synthesis (globinopathies) Lack of hemoglobin synthesis (hemoglobinopathies) Complications of anemic syndrome Decreased Hb reduces oxygen to tissues with consequent hypoxia. The effct of hypoxia depends on cells needs (neurons and muscle cells have greater needs) and on cell proliferation rate. Complications of anemic syndrome Biochemical changes: Krebs cycle activity is reduced due to low oxygen. Following, the synthesis of macroergic phosphates (plastic and energetic role) is reduced. Reduced Warburg respiratory chain activity with reduced heat production. Increased glycolitic activity with accumulation of non-volatile organic acids (lactic acid, pyruvic acid) flattens the hemoglobin dissociation curve (oxygen is released more easily to the tissue). Reduced liver metabolism. Complications of anemic syndrome Hemodynamic changes: Preferential redistribution of blood flow to vital organs (catecholamines causes vasoconstriction in the splanhnic and skin territory) - skin blood flow reduction causes - pallor, decreased skin temperature, feeling cold, shivering, trophic skin changes. Onset of symptoms depends on the magnitude and duration of the anemic syndrome. Hemodynamic compensatory hyperkinesia evidenced by: tachycardia, increased blood flow, increased blood speed, murmurs, increased circulatory flow. Hyperkinetic compensation increases oxygen consumption which, in time, will lead to cardiac decompensation (dyspnea, swelling, transudates, etc.) If there is a preexiting coronary obstruction, anemia and compensatory tachycardia, may lead to angina or increased frequency of its manifestation, instable angina or even myocardial infarction. Complications of anemic syndrome Respiratory changes Compensatory polipnea Renal changes Hypoxia stimulates production of erythropoietin Through hypoxia - induced transcription factor 1 * (HIF -1). Hypoxia stimulates renal renin → activates the renin angiotensin - aldosterone system → retention of sodium (electrolyte imbalance). Complications of anemic syndrome Alteration of tissue perfusion: Vasomotor activity and angiogenesis are modiffied. Promotion of angiogenesis is through vascular - endothelial growth factor - (VEGF). Changes in skin and mucous membranes (tissues with increased cell turn-over): Glossitis, esophagitis, gastritis, bronchitis, vulvovaginitis Leg ulcers Pigmentation Changes to appendages Brittle hair, digital hipocratism Complications of anemic syndrome Increased production of red blood cells Stimulation of erythropoietin encoding gene via hypoxia-induced transcription factor (HIF-1), results in increased synthesis of erythropoietin. * HIF-1 functions as a regulator of adaptive responses induced by hypoxia. Under conditions of hypoxia it activates transcription of over 40 genes, including those responsible for synthesis erythropoietin, glucose transporters, glycolitic enzymes, vascular - endothelial growth factor (VEGF) and other proteins that facilitate metabolic adaptation to hypoxia. Increasing production of red blood cells is mediated by erythropoietin. Rates of synthesis of erythropoietin is in inverse relationship with Hb concentration. Erythropoietin concentration can increase 1000 times in severe anemia. It enhances erythropoiesis, with expandation of erythropoietic tissue, possibly with sternal pain or diffuse bone pain. Complications of anemic syndrome Immune system abnormalities: Hipoxia lowers the defense capacity of the immune system, especially related to protection of mucosas; Anemic patient is prone to infections; Endocrine changes: Pituitary hypofunction Thyroid hypofunction Gonadal hypofunction Changes in menstrual cycle Amenorrhoea Impotence Particular form of anemia - Iron deficiency anemia Iron deficiency is the most common cause of anemia. 20% of women (50% of pregnant women) and 3% of men do not have enough iron in the body. Disruption of iron metabolism causes anemia and disturb cytochromes activity (cell respiration). Iron is obtained through dietary intake (muscle, liver) and iron absorption requires the presence of HCl and transferrin. Iron deficiency anemia - causes Loss of blood: Bleeding Menstrual loss Frequent blood emission Polycythemia vera (PV) – therapy Blood donors Neoplasms Inadequate intake: Vegetarian diet Global malabsorption / selective for iron Aclorhydria Resected stomach Celiac disease Parasitosis Iron metabolism disorders Lack of transferrin Congenital Hepatic Nephrotic syndrome Defective / deficient transferrin receptors Increased needs: pregnancy, lactation, gemelarity, prematurity, sports performance Iron deficiency anemia - causes Laboratory data Low Hb Normal or low number of reticulocytes Low sideremia Increased total iron binding capacity Elevated transferrin Low ferritin Absent iron reserves in the bone marrow (Perls staining) Blood smear CBC Microcytosis Hypochromia Pokylocitosis Low Hb, MCV ↓, MCH ↓, MCHC ↓ WBC count normal or slightly decreased Frequently thrombocytosis Bone marrow Red series hyperplasia with iron deficiency erythroblasts Blood smear Blood smear Anemia of chronic disease It is a normochromic, normocytic or hypochromic, microcytic anemia, which develops through multiple mechanisms. Newest name, inflammation associated anemia, is more representative because it reflects pathophysiological mechanisms. It secondary appears in: Chronic inflammation (infections, tuberculosis, endocarditis, abscesses); Collagen diseases (SLE, RA, SS); Malignancy (carcinoma, multiple myeloma, lymphoma) Elderly anemia. Pathogenesis This type of anemia is characterized by the inability of the body to increase red cell production, to compensate for red cell destructions more or less increased. Sustained stimulation of monocytic-macrophage system because of chronic inflammation, autoimmune diseases or tumors, decrease life of erythrocytes by increasing phagocytosis. During inflammation, iron releasing from macrophages and liver deposits is significantly inhibited. Interleukin 6 (IL-6) produced during inflammation induces the synthesis of hepcidine (iron regulating hormone), which in turn inhibits iron release from macrophages and hepatocytes, with consequent decreasing sideremia. Hepcidine binds the feroportin molecules from the membrane, molecules responsible for iron export, leading to their internalization and intracellular degradation. In this way iron stuck in macrophages and can not be used for Hb synthesis. It is known that iron is incorporated into protoporphyrin IX and zinc may substitute iron for its synthesis. Pathogenesis Another mechanism mediated through inflammation mediators (IL-1, interferon alpha) is low compensation capacity through erythropoietin by decreasing its synthesis. Finally there is a decreased iron in serum and erythrocyte precursors, with increased reserves of iron. The lifespan of red blood cells decreases without adequate compensation. Inflammatory cytokines promote the production of white blood cells. Other anemia with low erythropoietin Kidney disease - chronic renal insufficiency - insufficient production of erythropoietin due to renal lesions; Liver disease - by parenchymal liver failure (cirrhosis, toxic hepatitis, chronic aggressive hepatitis, etc.) - It reduces the synthesis of erythropoietin and hemoglobin precursors; Poliglandular hypofunction - production of erythrocytes is influenced by thyroid hormones, testosterone, glucocorticoids. Laboratory data Low Hb; Low number of reticulocytes; Low sideremia; Low total iron binding capacity; Increased ferritin; Perls staining of bone marrow shows reduced number of syderoblast and a high amount of hemosiderine in the macrophages. Megaloblastic anemia Anemia is normochromic, macrocytic defined by increasing MCV over 100 fl. Macrocytosis is typical in: Megaloblastic anemia Alcoholism Liver disease Megaloblastic anemia is characterized by nucleo-cytoplasmic asincronism due to deficiency in DNA synthesis with normal RNA and protein synthesis (immature nuclei and mature cytoplasm). The most common cause is vitamin B12 deficiency and / or folic acid deficiency. A common cause of B12 deficiency is Biermer anemia. It is believed that the mechanism is immune, mediated by antibodies to intrinsic factor (IF) or / and anti gastric parietal cells. Thus vitamin B12 absorption disorder is secondary to lack of IF. Megaloblastic anemia Folic acid: It is found in fresh vegetable products, liver; The daily necessary amount is about 100 mg, normal diet providing much more than this amount; The total reserve is up to 5 mg, enough for 3-4 months; Normal serum level is - 5 to 20 ng / ml; It is absorbed in the proximal jejunum; Vitamin B12: Food sources are animal products; B12 absorption occurs in the terminal ileum; The daily necessary is 1μg; B12 liver reserves are sufficient for 3-5 years; Serum B12 level is 200-600 pg / ml; Absorption is only in the presence of intrinsic factor (IF), glycoprotein produced by gastric parietal cells. Causes of B12 deficiency Deficient intake (malnutrition, vegetarian); Malabsorption: Inadequate production of IF (pernicious anemia), gastrectomy, congenital deficiency; A disease of the terminal ileum: celiakie, Crohn's disease, intestinal resection, intestinal neoplasms, selective malabsorption of B12; An intestinal consumption of B12: parasites, bacteria Drugs that interfere with B12 absorption: neomycin Deficiency in transportation and use of B12 : congenital deficiency of transcobalamin II (TC), excess of I and III TC, enzyme deficiency. Causes of folic acid deficiency Deficient intake : alcoholism, low-vegetable diet, infancy, prematurity Increased needs: Pregnancy Childhood Malignancies Intense hematopoiesis Chronic skin exfoliation (psoriasis) Malabsorption Drugs - barbiturates Signs and symptoms Depression Paranoia Hallucinations Psychosis Panic Attacks Changes in personality Suicide Decreased muscle strength Impotence Laboratory data Low Hb Low / normal number of reticulocytes CBC MCV > 100 fl Leucopenia Moderate thrombocytopenia Blood smear Macrocytosis (macrocytic anemia) , macro-ovalocytes, megalocytes Hypersegmented neutrophils (from 5 lobes) Bone marrow Hyperplasia, predominantly in red blood cells with asincronism in maturation of the hematopoetic precursors Laboratory data Biochemistry: Low serum cobalamin <100 pg / ml Increased level of intrinsic factor antibodies and anti-parietal cells Increased lactate dehydrogenase Increased or normal serum iron Schilling test positive - no excretion of radiolabelled B12 Atrophy of gastric mucosa at endoscopy Laboratory data Principles of treatment Treatment and management of underlying disease Blood transfusion Recombinant erythropoietin administration Vitamin B12/folate administration Iron preparations Dietary therapy Food acidification Stopping alcohol intake Vitamin supplementation Glucocorticoids Immunosuppressive drugs Splenectomy Marrow transplantation Phototherapy in newborn