Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
.
The Digestive System
Deglutition (Swallowing)
Deglutition (Swallowing)
Involves the coordinated activity of the tongue,
soft palate, pharynx, esophagus and 22 separate
muscle groups
Buccal phase – bolus is forced into the oropharynx
Pharyngeal-esophageal phase – controlled by the
medulla and lower pons
All routes except the one into the digestive tract are
sealed off
Peristalsis moves food through the pharynx to the
esophagus
THEORY OF CONSTANT PROPORTION
1. Oral phase; the bolus is formed and
transported under voluntary control to the
pharynx;
2. Pharyngeal phase; following receipt of the
bolus, the pharynx is activated to propel the
food to the oesophagus;
3. Oesophageal phase; passage of bolus down
the oesophagus to the stomach by oesophageal
contraction
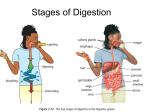
Physiology of Deglutition (Swallowing)
Moving bolus from
mouth to stomach
Three phases
Facilitated by saliva,
mucous secretions
Involves mouth,
pharynx, esophagus
1. Buccal phase
Voluntary
Occurs in the mouth
Moves bolus to oropharynx
Food is formed into a bolus
The bolus is forced into the pharynx by the tongue
Voluntary elevation and retraction of tongue
against the hard palate propels the bolus to the
pharynx
Physiology of Deglutition
2.Pharyngeal phase
Involuntary
It is very rapid (1 second) occur
reflexly {Swallowing reflex}
Receptors in oropharynx
(tonsillar pillars)
Afferent : glossopharyngeal
nerves
Center: medulla oblongata
(Swallowing Center) and pons
Efferent :motor fibers of cranial
nerves V,IX,X,XII.
Response: series of reflexes to
prevent entry of food into air
passages:
Response: series of reflexes to prevent entry of food
into air passages:
1. Block mouth with tongue
2. Block nasopharynx with soft palate
3. Raise larynx to seal epiglottis, blocking airways
4. Relax upper esophageal sphincter
Bolus is moved through pharynx into esophagus
.
1-Elevation of soft palate closure of nasal cavity
2-Approximation of palatopharyngeal folds
sagittal slit through which small food particles pass
and prevent passage of large particles
3- Closure of glottis (opening of larynx) by
approximation of vocal cords& elevation of larynx and
folding of epiglottis.
4-Inhibition of breathing (Swallowing apnea).
5-Relaxation of pharyngeo-esophageal sphincter and
contraction of superior pharyngeal muscle –rapid
pharyngeal peristalsis –forces the food into relaxed
upper oesophagus.
Deglutition (Swallowing)
Pharyngeal-esophageal phase
Involuntary transport of the bolus
All passageways except to the stomach are blocked
Tongue blocks off the mouth
Soft palate (uvula) blocks the nasopharynx
Epiglottis blocks the larynx
Peristalsis moves the bolus toward the stomach
The cardioesophageal sphincter is opened when
food presses against it
Deglutition (Swallowing)
Figure 14.14
Deglutition (Swallowing)
Figure 22.13a-c
.
Physiology of Deglutition
3. Esophageal stage
Upper esophageal sphincter
(UES) closes:
pharyngeo-esophageal
junction is normally closed by
striated muscle tone to prevent
entry of inspired air into
stomach.
During swallowing the
sphincter relaxes reflexely and
then reclosed after swallowing.
Gastroesophageal
sphincter opens
Esophagus controls involuntary
peristaltic movement
Epiglottis reopens
Bolus moves from esophagus
to stomach
Esophagus
Peristalsis
Involuntary, rhythmic
contraction of
muscularis
Controlled by
medullary centers
A movement activity:
inner circular layer of
smooth muscle
contracts behind bolus
to push it forward;
outer longitudinal
muscle contracts to pull
esophagus wall up
Upper esophageal
Esophagus
sphincter
Peristalsis
Lower esophageal
(cardiac/gastroesophageal)
sphincter
Sharp transition from
nonkertinized stratified
squamous epithelium to
simple columnar epithilium
Esophageal epithelium
resistant to abrasion but
not to acid and proteolytic
enzyme attack – acid
reflux disease
Esophageal phase
Peristaltic contractions in body of esophagus
combined with simultaneous relaxation of the
lower esophageal sphincter propel the bolus
into the stomach.
CAUSES OF DYSPHAGIA
Divided into two categories:
Oropharyngeal dysphagia (OPD) Abnormalities
affecting the neuromuscular mechanisms controlling
movements of the tongue, pharynx, and UES
Esophageal dysphagia (ED)
Abnormal affecting the esophagus itself
.
.
.
.
.
.
.
Deglutition (Swallowing)
Figure 22.13d, e
.
.
Oral Preparatory Phase
tongue positions material on the teeth
rotary lateral movement of the mandible and tongue
during mastication
tongue moves the material back onto the teeth as the
mandible opens
after cycle is repeated numerous times, a bolus is
formed
during active chewing, the soft palate is not pulled
down and forward and premature spillage is common
and entirely normal