Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
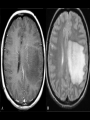
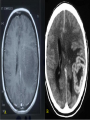
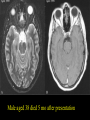
Demyelinating diseases FM Brett., MD., FRCPath Classification of demyelinating disorders of the CNS 1. Primary demyelinating diseases – MS, ADEM, AHL 2. Secondary demyelinating diseases CPM, PML, SADC, 3. Leukodystrophies and metabolic disorders e.g sudanophilic leucodystrophy, metachromatic leucodystrophy, adrenoleucodystrophy, Krabbes leucodystrophy, Canavans disease 4. Toxic demyelination - Hexachlorophane, cyanide, carbon monoxide, chronic solvent vapour abuse. MS • Chronic, progressive immune-mediated CNS disease • Characterized by demyelination and axonal loss neurologic impairment and disability • Axonal damage and brain atrophy occur early and may be irreversible ~ 85 % RRMS i.e sporadic attacks followed by complete, partial or no improvement ~ Within 10 years half of these pts develop secondary-progressive disease (essentially unrelenting clinical progression with possible superimposed acute attacks and minor remissions) ~ Remainder primary-relapsing disease – characterised either by progression from onset with acute relapses OR Primary progressive disease progression without relapse or remission Epediomology of MS • ~350,000 affected in US – ~8,500–10,000 new cases yearly • Most cases strike between ages 15 and 45 – Women outnumber men 2:1 • 85% present with RRMS – Within 10 years, 50% of these patients develop secondary-progressive MS associated with significant disability Presenting features of MS Limb weakness 50% Optic neuritis 20% Diplopia 10% Parasthesia 10% Bladder Parasthesia 10% Vertigo and nystagmus 5% Diagnosis of MS Dissemination of lesions in time Dissemination of lesions in space Paraclinical tests VER, MRI Clinical history Less commonly acute mass lesion difficult to distinguish clinically and pathologically from a neoplasm MS Characteristics 1. Immune-mediated CNS disease 2. Characterized by demyelination Axonal Transection in acute acute Multiple Axonal Transection in MultipleSclerosis Sclerosis and axonal loss neurologic lesions lesions impairment and disability 3. Dissemination of lesions in space SMI-32 (non-phosphorylatedneurofilament) neurofilament) -demyelinated swellings SMI-32 (non-phosphorylated -demyelinatedaxons axonsand and swellings MBP intact axons MBP intact axons Bruce Trapp et al., NEJM 338,278 278(1998) (1998) Bruce Trapp et al., NEJM 338, Normal white matter Active demyelination Inactive plaque Biopsy F23 Ambulant 14 yrs later F21 wheelchair bound F 36 Died 56 dys after admission Normal white matter Active demyelination Inactive plaque Pathological features of acute demyelination Hypercellularity – macrophages +++++ Areas of complete myelin loss Relative axonal preservation Perivascular lymphocytic cuffing Annesley-Williams et al., JNEN 2000;59:477-89 Inflammation and axonal Inflammation andtransection Axonal Disease Stage Early Main Component Main Clinical Outcome Inflammation and demyelination Relapses (incipient global tissue loss, altered NAA content) Late Atrophy, axonal loss, and increasing tissue destruction (less Gd-defined inflammation, demyelination ongoing) Disability AXONAL TRANSECTION IN ininacute Axonal Transection Transection acuteMultiple MultipleSclerosis Sclerosis lesions ACUTE MS MS Lesions A 64 m B 45 m Reprinted with permission from Trapp BD et al. N Engl J Med. 1998;338:278-285. Copyright 1998 Massachusetts Medical S All rights reserved. swellings (non-phosphorylated neurofilament) SMI-32 (non-phosphorylated SMI-32 neurofilament)-demyelinated -demyelinatedaxons axonsand and swellings axons intact axons MBP intact MBP Clinical forms of MS • • • • • • • • Charcot triad Generalised form Onset with ocular symptoms Sensory form Cerebral form Spinal form Brainstem forms Acute multiple sclerosis BBB Blood –brain barrier breakdown as initiating event in demyelination Endothelial reaction EC ECEC EC Cytokines, chemokines, excitotoxins Macrophage activation accumulation Gliosis BBB Break down Sinus arachnoid villi Spinal nerves Lymphatics Lymphatics Lymph node Lymph node Dominant parameter governing leukocyte traffic into the CNS 1. Activation of the migrating cell type: T cells B cells 2. Alteration/activation of the CNS endothelial cell Neutrophils Phagocytic macrophages Memory and naïve T cells 3. Physiological (no known alteration/activation required) Perivascular cells Microglia (during fetal life) Meningeal macrophages Choroid plexus macrophages Mast cells Parenchymal reaction as the initiating event in demyelination Recruitment of elements for defensive inflammatory reaction EC EC EC BBB breakdown stimulus BB T T B Cytokines, chemokines, excitotoxins NAWM and ‘new’ imaging techniques Study Werring er al., Brain 2000 Rocca et al., Neurol 2000 Filippi et al., Ann Neurol 1998 Goodkin et al, Neurol 1998 Technique MR diffusion imaging Mean diffusivit y MTR MTR Time interval 6-8mo between changes and lesion appearance 6 weeks 3 mo Several months Location of lesion Away from areas of enhancem ent Contralat eral NAWM NAWM NAWM Pathological NAWM T1, T2 NAWM Diff imaging MTR Evangelou et al., Ann Neurol 2000 Allen et al., J Neurol Sci 2001 Allen & McKeown., J Neurol Sci 1979 Adams CWM., B Med Bull 1979 De Groot., Brain 2001 van Waesberghe et al., Ann Neurol 1999 van Walderveen et al., Neurology 1998 Werring et al., Brain 2000 Rocca et al., Neurol 2000 Filippi et al ., Ann Neurol 1998 Goodkin et al., Neurol 1998 A B A B Female aged 36 years 24 weeks gestation A B A B Male aged 38 died 5 mo after presentation A B A B ADEM vs MS Clinical CSF Radiology Pathology ADEM monophasic Cells ++ OB+ Abn Symmetric Cerebrum Cerebellum Basal ganglia Inflam +++ Demyel + MS Multiple lesions Inflam + Demyel ++++ monosympt Cells + omatic OB + EDSS: Progression to Disability Walking Ability 10.0 = Death due to MS 9.0–9.5 = Completely dependent 8.0–8.5 = Confined to bed/chair; self-care with help 7.0–7.5 = Confined to wheelchair 6.0–6.5 = Walking assistance is needed 5.0–5.5 = Increasing limitation in ability to walk 4.0–4.5 = Disability is moderate Confined to a wheelchair or bed Walks with aid (<5 yards) Walks with assistance (22–220 yards or more) Walks unaided (110–220 yards or more) Walks unaided (330–550 yards or more) 3.0–3.5 = Disability is mild to moderate 2.0–2.5 = Disability is minimal Fully ambulatory 1.0–1.5 = No disability 0 = Normal neurologic exam Kurtzke JF. Neurology. 1983;33:1444-1452. Diagnosis of MS Dissemination of lesions in time Dissemination of lesions in space Paraclinical tests VER, MRI Clinical history Less commonly acute mass lesion difficult to distinguish clinically and pathologically from a neoplasm Central Pontine Myelinolysis ~ Middle aged or elderly patients who are malnourished or chronically debilitated ~ Associated with fluid-electrolyte imbalance particularly where hyponatremia has been treated rapidly with hypo-osmolar saline ~ Mechanism of demyelination is unknown but may relate to impaired vascular perfusion during the episode of rapid electrolyte shift ~ Myelin loss usually occurs in the central pons Progressive Multifocal leucoencephalopathy ~ Lytic infection of oligodendrocytes by JC virus ~ Usually debilitated or immunosupressed patients ~ well recognised complication of Aids PML