Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Environmental impact of pharmaceuticals and personal care products wikipedia , lookup
Discovery and development of direct thrombin inhibitors wikipedia , lookup
Discovery and development of ACE inhibitors wikipedia , lookup
Metalloprotease inhibitor wikipedia , lookup
Discovery and development of neuraminidase inhibitors wikipedia , lookup
Prescription costs wikipedia , lookup
Neuropharmacology wikipedia , lookup
Pharmaceutical industry wikipedia , lookup
Psychopharmacology wikipedia , lookup
Pharmacogenomics wikipedia , lookup
Neuropsychopharmacology wikipedia , lookup
Theralizumab wikipedia , lookup
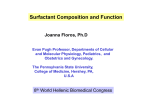
Respiratory Drugs Part 2 V. Leukotriene inhibitors A. Leukotrienes • Leukotrienes (LT) are a family of eicosanoid, formed when arachidonic acid (released by phospholipids in cell membranes) is reacted upon by the lipooxygenase (LOX) enzymes. • LT’s are synthesized by a number of different cells (i.e. mast cells, macrophages) in the airways. • Three LT’s in particular, LTC4, LTD4, and LTE4 are responsible for many of the effects which occur during an attack, especially bronchoconstriction. • There are 2 categories of LT inhibitors: receptor antagonists and LT synthesis inhibitors. • Both categories are effective in blocking antigen induced (grass, cat dander, ragweed, and mixed antigens), • as well as exercise-induced airway responses. • Neither category is as effective as inhaled corticosteroids in regard to alleviating symptoms, airway inflammation and bronchial reactivity. • However, they are equal to inhaled corticosteroids in reducing the frequency of asthma exacerbation. • An advantage the LT inhibitors have over the inhalation corticosteroids is that they are administered orally. • This is useful in patients who have poor compliance with the correct use of a MDI (children, the elderly). B. Receptor antagonists 1. montelukast (Singulair) • This works by blocking the binding of LT’s. • It’s safety and effectiveness has been demonstrated in children as young as 6 months of age. It is generally administered in the evening (PO 10 mg, children PO 4 mg). • Adverse effects in adults include headache, fatigue, cough and rash. • The same adverse effects, as well as otitis, sinusitis, nausea and diarrhea are seen in children. 2. zafirlukast (Accolate) • This is similar to Singulair in that it is a receptor antagonist of leukotriene. • Specifically, it is a selective and competitive receptor antagonist of leukotriene D4 and E4 (LTD4 and LTE4), components of slow-reacting substance of anaphlaxis(SRSA). • It is administered either 1 hour before or 2 hours after meals (adults PO 20 mg, bid; children PO 10 mg bid). • Headache is the most frequently reported adverse effect. • Other adverse effects are similar to those reported for montelukast. C. Leukotriene synthesis inhibitor 1. zileuton (Zyflo) • This drug has a different mechanism of action, it inhibits formation of leukotrienes by inhibiting the enzyme 5-lipoxygenase (5-LO). • The dosage is 400-800 mg, 2-4 times a day. It is approved for the prevention and chronic treatment of asthma in patients aged 12 years and older. • In a clinical study, patients receiving Zyflo were able to reduce their use of inhaled beta-adrenergic drugs. • Headache is the most frequently reported adverse effect. There are also a few reports of liver toxicity (elevated liver enzymes) with this drug. VI. Decongestants A. Decongestant actions • Decongestants act as vasoconstrictors to reduce blood flow to mucous membranes in the nose, sinuses and pharynx. • They produce vasoconstriction by stimulating alpha receptors in the smooth muscle around blood vessels B. Oral decongestants • The most common oral decongestants are: • 1. pseudoephedrine (Chlor-Trimeton, Dimetapp, Drixoral, Sudafed, Suphedrin, Triaminic, many generics). • Also found in many combination products (Actifed Cold and Sinus) which contain antihistamine/pain reliever (aspirin, acetaminophen, or ibuprofen). • The dosage is 60 mg every 4-6 hours, or 120 mg extended release every 12 hours, or 240 mg extended release, once a day. • As pseudoephedrine has been used in the illicit manufacture of methamphetamine, Federal regulations require that all OTC medications that contain pseudoephedrine be kept behind the counter in the pharmacy. • In addition, people buying these products must provide a photo ID and sign a logbook. 2. phenylephrine • Some drug companies are concerned that the Federal regulations regarding pseudoephedrine may keep people from buying their products, so they have reformulated their products by removing the pseudoephedrine and substituting phenylephrine for it. • Pseudoephedrine and phenylephrine • Note the long list of medications that contain phenylephrine: • Sudafed PE, PediaCare Children’s decongestant, Actifed Cold and Allergy, Benadryl Allergy & Cold, Benadryl Allergy & Sinus, Children’s Sudafed Cough & Cold, Children’s Tylenol Plus Cold, Children’s Tylenol Plus Cold & Allergy, Excedrin Sinus Headache, Sudafed PE Nightime Nasal decongestant, Sudafed PE Sinus & Allergy, Sudafed PE Cold & Cough, Sudafed PE Multisymptom, Theraflu Cold & Cough, Theraflu Cold & Sore Throat, Theraflu Daytime Severe Cold, • Theraflu Daytime Flu & Sore Throat, Theraflu Nighttime Severe Cold, Triaminic Cold & Allergy, Triaminic Daytime Cold & Cough, Triaminic Nighttime Cold & Cough, Tylenol Allergy MultiSymptom, Tylenol Cold Head Congestion, Tylenol Cold MultiSymptom, Tylenol Cold MultiSymptom Daytime, Tylenol Cold MultiSymptom Nighttime, Tylenol Sinus Congestion & Pain Daytime, Tylenol Sinus Congestion & Pain Nighttime, Tylenol Sinus Congestion Severe, Vicks Day Quil Sinus, Vicks Day Quil Cold/Flu, Vicks Formula 44D Cough & Head Congestion Relief. • Congressman Henry Waxman, among others, have expressed concerns that these newly formulated drugs are not working well enough for their intended purpose. • In a peer-reviewed letter to the editor published in late 2006 in the Journal of Allergy and Clinical Immunology, two University of Florida researchers concluded that there is "virtually no evidence to show that phenylephrine oral nasal decongestants at the FDAsanctioned dose of 10mg are effective”. • To address the issue, Waxman has twice called upon the US Food and Drug Administration (FDA) to launch an investigation into the use of phenylephrine in these drugs, based on a study by Schering-Plough. • According to Schering-Plough, phenylephrine was "not significantly different from placebo in decreasing nasal congestion" while pseudoephedrine was "significantly more effective," in a clinical trial involving 38 people. • Both phenylephrine and pseudoephedrine oral have a prolonged duration of action compared to topical decongestants, but they also have more adverse effects. • These include excitability, nervousness, and insomnia. C. Topical decongestants • 1. Oxymetazoline (Afrin, Dristan 12 hours nasal, NeoSynephrine 12 hour, various generics). The recommended dosage for this 0.05% solution is 2-3 sprays per nostril, two times a day. • 2. Phenylephrine containing nasal sprays (Neo Synephrine) • This is available in 0.25, 0.5 and 1.0% solutions. The recommended dosage is 23 sprays per nostril, two times a day. This nasal spray form of phenylephrine is more effective than the pill form • 3. xylometazoline (Otrivin) • This is available in 0.05 and 0.1% solutions. The recommended dosage is 23 sprays per nostril, every 8-10 hours. • These topical decongestants are recommended for the acute treatment of congestion related to the common cold. • They should not be used for longer than 3 days, as they tend to cause rebound congestion. VII. Expectorants A. Expectorant actions • Expectorants reduce the viscosity or thickness of sputum so that patients can more easily cough it up • The use of expectorants, especially in the treatment of a common cold, is controversial. • Traditional colds involve the upper respiratory tract, whereas expectorants are designed to facilitate mucus removal from the lower respiratory tract. • In addition, many clinicians have questioned their effectiveness in actually facilitating the clearance of mucous. B. Expectorant agents • 1. Guaifenesin (Mucinex, Robitussin, numerous generics) • Guaifenesin is the only FDA approved OTC expectorant, 100 – 400 mg every 4 hours. • It is an ingredient also in many combination products which come in several forms, including capsules, tablets, and liquids. • It may be combined with antihistamines, antitussives, or decongestants. VIII. Antitussives • Antitussives are agents which suppress a cough. Their main purpose is to control nonproductive dry coughs. • They are not indicated in the treatment of productive cough as they may allow accumulation of secretions which lead to airway obstruction. A. nonopioid • 1. dextromethorphan (Benylin, Delsym, Robitussin, Vicks, various generics) • Dextromethorphan is a non-opioid antitussive without analgesic or addictive properties. • This is often found in combination products along with antihistamine/decongestant/expectorant. The recommended dosage is 10-20 mg every 4 hours or 30 mg every 6-8 hours. B. opioid • Opioids are the most effective drugs available for cough suppression. This is achieved at doses below those used to produce an analgesic effect. • The specific mechanism of antitussive action of opioids is not known, however, it appears that the receptors involved in their antitussive effects are different from those associated with their analgesic effects. • 1. codeine • 10-20 mg every 4-6 hours as needed, but not to exceed 120 mg in 24 hours 2. hydrocodone • There are a number of FDA approved hydrocodone-containing antitussives marketed in the U.S. • In terms of cough suppression, hydrocodone is about 3 times more potent than codeine. It can lead to both physical and psychological dependence. • hydrocodone and chlorpheniramine (Tussionex suspension): • This formulation contains an antihistamine (chlorpheniramine) along with the antitussive hydrocodone. • The dosage is 5 mL of the suspension every 8-12 hours. Side effects include dry mouth, dizziness, drowsiness, euphoria, nausea, vomiting and constipation. • hydrocodone and homatropine (Hycodan, Tussigon): This formulation contains an anticholinergic, homatropine, which is effective in drying up secretions. • It is available both in a suspension and tablet form: 1 tablet/tsp every 4-6 hours. Side effects include dizziness, nausea, vomiting and constipation IX. Mucolytic agents • These agents interfere with the chemical structure of mucous making it less viscous • 1. acetylcysteine or N-acetylcysteine (Mucomyst) • Acetylcysteine is used to help break up the thick, viscous, mucous that is often present in people suffering from respiratory ailments. • It accomplishes this by breaking the disulfide bonds in mucoproteins thereby lowering their viscosity. • It is indicated as an adjuvant treatment for the following: • • • • • • • amyloidosis, bronchiectasis, bronchitis, cystic fibrosis, emphysema, pneumonia tuberculosis • The usual dosage is 2-20 ml of a 10% solution via a nebulizer, but high dose oral N-acetylcysteine has recently been used to treat inflammation in cystic fibrosis patients • 2. dornase alpha (Pulmozyme) • Dornase alfa is a solution of recombinant human deoxyribonuclease (rhDNase). • This is a treatment used by cystic fibrosis patients to clear the mucus that accumulates in the airways and leads to infection (Pseudomonas aeruginosa). • Their sputum contains a higher concentration of DNA. • This is believed to be derived from the nuclei of degenerating WBC’s, and results in an increase in viscosity of their sputum. • It was approved by the FDA in 1993. • It is administered as a 2.5 mg single ampule inhaled once a day via a nebulizer. • It must be kept refrigerated. • Side effects of its use include cough, laryngitis and hoarseness. X. Surfactants A. Lung surfactant • In premature infants, a deficiency of lung surfactant often leads to respiratory distress syndrome (RDS) of the newborn, believed to account for approximately 1520% of all neonatal deaths in Western countries. • This syndrome is characterized by a 2 to 15 times greater surface tension than normal, due to a deficiency of lung surfactant. • Lung cells which produce surfactant (arrows) • Lung surfactant is found in the liquid layer that lines the alveoli of the lungs. • The primary role of lung surfactant is to decrease the surface tension of the liquids lining the alveoli. • There are several important physiological effects of a decrease in surface tension brought about by the presence of a surfactant in the alveoli: • prevention of alveolar collapse; • a decrease in surface tension increases compliance (stretching), which means that less work is needed to expand the alveoli; • and a decrease in surface tension prevents water from leaking into the alveoli from the lung capillaries. • RDS of the newborn is most common in infants whose gestational age is less than 34 weeks. • There is a test which can be performed before birth, which helps predict the maturity of the fetal lung. • In this test, a sample of amniotic fluid is tested to determine its L/S (Lecithin/Sphingomyelin) ratio • (Surfactant is composed of about 85-90% lipid, and most of this is dipalmitoylphosphatidylcholine, or lecithin). • sphingomyelin • A ratio of 2 or greater is desired, and is normally found at the gestational age of about 4 weeks up to term. • If the ratio is between 1.5 and 1.9, there is slightly less than a 50% chance of developing RDS. • The risk increases greatly to about 75% when the L/S ration is less than 1.5 B. Treatments 1. Antenatal treatment • Antenatal treatment with corticosteroids for women in preterm labor. • These corticosteroids induce a significant and rapid acceleration of lung maturation. • They are currently recommended in a setting of preterm labor at 24-34 weeks gestation unless delivery is imminent. • The treatment with corticosteroids continues for 48 hours while attempting to halt labor. • Generally, either two 12 mg doses of betamethasone IM, 24 hours apart • or • four 6mg doses of dexamethasone IM, 12 hours apart 2. Exogenous surfactant a. beractant (Survanta, derived from bovine lung extract) • 4 ml/Kg of birth weight in four divided doses through a catheter placed into the endotracheal tube, with the infant manually ventilated for a minimum of 30 seconds, or until stable between each dose. • Repeated after 6 hours if there is continuing respiratory distress • This is specifically recommended by the manufacturer for prophylactic therapy in infants weighing less than 1,250 g, within 15 minutes of birth. • In addition, it is indicated within 8 hours of birth for infants with evidence of RDS. b. poractant alfa (Curosurf, derived from porcine lung extract), • 2.5 ml/Kg of birth weight in two divided doses through a catheter placed into the endotracheal tube, with the infant manually ventilated with 100% oxygen for 1 minute. • A 1.25 ml/Kg of birth weight subsequent dose, is repeated twice at 12 hour intervals if needed. Maximum dose of 5 ml/Kg of birth weight. c. calfactant (Infasurf, derived from bovine lung extract) • 3 ml/Kg of birth weight to an intubated infant in two divided doses if administered by side-port delivery or 4 doses if by catheter delivery, with the infant mechanically ventilated for up to 2 minutes between doses d. recombinant human surfactant protein D (rhSP-D) • In a study published in February 2010 in the American Journal of Respiratory and Critical Care Medicine, premature lambs were treated with either Survanta or Survanta containing rhSP-D. • In lambs given Survanta alone, manual ventilation resulted in pulmonary inflammation. • In the group given Survanta with rhSP-D, there was an inhibition of lung inflammation. This agent has potential for use in premature human infants. C. Adverse effects of surfactant therapy • Adverse effects of surfactant therapy include: acute obstruction of the airway resulting in hypoxemia and bradycardia with a large volume in a single dose, rather than small repetitive additions; • apnea; • and pulmonary hemorrhage (generally in infants weighing less than 700 g at birth) XI. Phosphodiesterase inhibitors A. Phosphodiesterase • There are 11 families of phosphodiesterase, numbered PDE1PDE11. Of particular interest are phosphodiesterase-3 (PDE3), and phosphodiesterase-4 (PDE4) found in airway smooth muscle and epithelial cells. • PDE4 hydrolyzes cAMP, and there is compelling scientific rationale (i.e they are anti-inflammatory in animal models as well as in in vitro studies) for developing PDE3 and 4 inhibitors for use in the treatment of COPD. B. Clinical trials • A 6 month Phase II trial tested the efficacy of one of these PDE4 inhibitors, cilomilast (Ariflo). • cilomilast (Ariflo) • It was administered orally, and reached the most distal portions of the lungs via the systemic circulation. • Not all inhaled bronchodilators are capable of penetrating this deeply, which is significant in that inflammation is often continually present in these small airways. • There was a significant improvement in airflow, compared to placebo (40 ml difference in FEV1), as well as a (more subjective) quality of life improvement, as measured by a questionnaire. • Currently, a Phase III clinical trial has been completed (May 2009) but the results have not yet been published. • Similar findings occurred with a different PDE4 inhibitor. • In July 2009, an application was filed with the FDA for approval of once daily oral roflumilast (Daxas). • A study from 4 clinical trials with roflumilast was expected to be published sometime in 2009 or 2010. • Patients involved in studies conducted with both cilomilast and roflumilast experienced a time delay between exacerbations of their COPD when receiving a PDE4 inhibitor. • The scientists conducting the studies believe that the systemic distribution of the PDE4 inhibitors to the distal airways may be the key to the effectiveness of these drugs. • Although resting lung volumes were not tested in their trials, they believe that improvement in this parameter would be seen if measured in future trials. • Ibudilast (development codes AV-411, MN-166) does not have FDA approval in the U.S., but is available in Japan, where it is used as an anti-inflammatory agent in the treatment of asthma. • Studies indicate that it has a better safety profile and is more potent than theophylline. • Some of the adverse effects associated with PDE inhibitors are GI related (i.e. dyspepsia, nausea). • This has limited their development as potential candidates in the treatment of COPD. • Ibudilast has acceptable GI tolerability. XII. Protease inhibitors A. Alpha-1 antitrypsin • Neutrophil elastase is a protease enzyme which degrades elastic fibers in connective tissue. • Alpha-1 antitrypsin (AAT), also known as Alpha-1-Proteinase is a protein made by the liver and released into the circulation. • Alpha-1 antitrypsin is a protease inhibitor which degrades neutrophil elastase and therefore plays a protective role in the places where unchecked neutrophil elastase activity can have serious consequences, particularly the lungs and liver. • If the breakdown of tissue occurs in the alveolar wall, it can lead to emphysema. • Alpha-1 antitrypsin deficiency (AATD) is an inherited condition that causes low alpha-1 antitrypsin (AAT) levels in the blood. • This predisposes those with the most severely deficient phenotype (PI*ZZ), to emphysema and liver disease (neonatal jaundice, cirrhosis, hepatoma). • people with normal alleles for AAT are designated PI*MM • heterozygotes are designated PI*MZ • Of the approximately 300 million Americans, about 100,000 have the severe AATD (PI*ZZ), and approximately 8 million are heterozygotes. • This condition is found most often in Caucasians of European ancestry, the Z allele is not common in Americans of Asian and African descent. • Symptoms of AATD include jaundice in a newborn or infant that lasts for an extended period of time (more than a week or two); • and wheezing, a chronic cough or bronchitis, and shortness of breath after exertion in a person under 40 years of age (especially when the patient is not a smoker, and has not been exposed to known lung irritants). B. AATD drug therapy • There are, currently, 4 agents approved by the FDA for the treatment of AATD. • These products are derived from human plasma and are extremely expensive (up to $100,000 per year, per patient). • These agents are indicated only for patients with the PI*ZZ phenotype, and not for individuals with cigarette-smoking related emphysema with PI*MM or PI*MZ phenotypes, or those with liver disease due to AATD, unless they also have lung disease. • The 4 agents are Prolastin, Zemaira, Aralast and Glassia. • Glassia is the newest alpha-1 antitrypsin inhibitor, receiving FDA approval in July 2010. Baxter International in October 2010 received the exclusive distribution rights for Glassia in the U.S., Canada, Australia, and New Zealand from Kamada Ltd. (Israel) for $20 million. • All 4 of these agents are administered IV, once a week (recommended dosage of 60 mg/Kg of body weight). • Clinical trials are currently underway in Europe for an inhaled version of an alpha1 antitrypsin inhibitor. Approval for this is expected in 2012 in Europe, with the U.S. to follow shortly after. • There is a randomized, placebo-controlled, double-blind, study conducted by CLS Bering to assess whether the progression of emphysema can be halted by continuous, long term therapy with Zemaira. • The study began in January of 2006 and is expected to end in March 2011. The effect of Zemaira on the progression of emphysema will be assessed by the decline of lung density, measured by computerized tomography (CT). XIII. Tumor necrosis factor inhibitors A. Tumor necrosis factor • During the inflammatory response triggered normally by infection, but also by cigarette smoking, macrophages are activated, and release cytokines. • Cytokines are proteins which mediate communication among the cells of the immune system, as well as between the cells of the immune system and other body systems. • There are 3 major categories of cytokines: interleukins, tumor necrosis factor (TNF) and interferons. • The cytokine of interest here is TNF which induces programmed cell death, primarily in tumor cells, but also in any cell with a receptor. • The sputum of COPD patients has increased levels of TNF-α. • It is believed that an increase in circulating TNF-α leads to the skeletal muscle apoptosis that is associated with the severe wasting in some advanced COPD patients. B. TNF blockers • TNF blockers such as infliximab (Remicade) have been effective in other chronic inflammatory diseases (rheumatoid arthritis, inflammatory bowel disease) and, therefore, may be effective in COPD patients. • However, in a 6 month study of 234 smokers, 40 years or older, it was shown that infliximab was not beneficial in patients with moderate to severe COPD (based on the Chronic Respiratory Questionnaire, prebronchodilator forced expiratory volume in 1 second [FEV1], and 6 minute walk distance. • This study was published in the May 2007 issue of The American Journal of Respiratory and Critical Care Medicine. • It should be noted that infliximab is a chimeric (mouse/human) recombinant antibody construct which results in a large antigenic trigger. • Newer TNF binding proteins have been engineered, and trials of anti-TNF therapies specifically for patients with COPD are currently underway. • The anti-TNF-α agents currently available, include infliximab (Remicade), etanercept (Enbrel) and adalimumab (Humira). • Remicade was first approved in the United States for the treatment of Crohn’s disease in 1998 and later approved for the treatment of Ulcerative colitis in September 2005. • Enbrel was approved for the treatment of rheumatoid arthritis in 1998. • So far, Humira has been approved by the FDA for the treatment of moderate to severe rheumatoid arthritis in 2002, moderate to severe Crohn's disease in 2007 and moderate to severe psoriasis in 2008. • Before any of these drugs can be approved for the treatment of COPD, clinical trials must be completed and the results, published. • Another approach may be to target the enzyme which is responsible for releasing TNF, TNF-α-converting enzyme (TACE). C. Other potential therapeutic targets for drug development in COPD • A recent study has assessed the ability of 36 different biomarkers to confirm the presence of COPD exacerbation and predict its severity. • • • • • This study found that C-reactive protein (CRP), IL-6, myeloid progenitor inhibitory factor (MPIF)-1, pulmonary and activation–regulated chemokine (PARC), • adiponectin (ACRP-30), and • soluble intercellular adhesion molecule (sICAM)1 • significantly vary between baseline and exacerbation of COPD. • These biomarkers are potential therapeutic targets