Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Psychedelic therapy wikipedia , lookup
Neuropsychopharmacology wikipedia , lookup
Prescription costs wikipedia , lookup
Adherence (medicine) wikipedia , lookup
Neuropharmacology wikipedia , lookup
NK1 receptor antagonist wikipedia , lookup
History of general anesthesia wikipedia , lookup
Psychopharmacology wikipedia , lookup
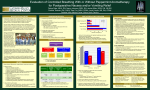
Post Operative Nausea & Vomiting Nicole Weiss MD September 22, 2010 Objectives Importance PONV Risk Factors Review of anti-emetics and strategies aimed at reducing PONV Risk based treatment Rescue Therapy Tulane University Pharmacy The Patient 41 y/o female with a h/o of PONV scheduled for an outpatient laparoscopic cholecystectomy Motion sickness Non-smoker PONV: Importance? 1. High Level of patient concern (second to pain) -willingness to pay $56-$100 2. Major cause of unanticipated hospital admissions 3. Rare complications: pulmonary aspiration, incisional disruption Physiology Vomiting Center – Located in the Medulla Tickling the back of the Throat Gastric Distension Vestibular Stimulation (Etoh) Cerebral Cortex Chemoreceptor trigger zone – Outside of the BBB communicates with the vomiting center – Blood Borne Drugs or Hormones Neurotransmitters involved: – Dopamine, 5-HT, Substance P, Ach Apfel. Miller's Anesthesia. Strategies for Minimizing PONV 1. Identify high risk patients -25-30% incidence of PONV -0.18% intractable PONV 2. Avoid emetogenic stimuli 3. Multimodal antiemetic therapy Risk Factors Patient, Procedure, Anesthesia History of previous PONV History of motion sickness History of migraines Female gender post puberty Childhood after infancy and young adulthood Nonsmoker The type of surgery: laparoscopic, middle ear, ophthalmologic, craniotomy Increasing duration of surgery Dehydration Pain Use of volatile anesthetics, opioids, nitrous oxide or neostigmine “Up to 70% incidence of PONV in “high risk” patients (Kim) Apfel’s Simplified Risk (Adults) 1,2,3 or 4 risk factors-->10, 20,60,80% Female 2. H/o of PONV or motion sickness 3. Non smoking 4. Postoperative IV opiods 1. Apfel, et al. NEJM. 2004. Drugs associated with PONV Nitrous oxide Volatile agents Etomidate Neostigmine (high doses) Excessive opiods Comparison of Agents Apfel, et al. 2002. Protective Anesthesia Hydration Regional Anesthesia TIVA – Utilizing propofol as effective as ondansetron – Dose response relationship for propofol Oxygen Acupuncture Antiemetics 1. 2. 3. 4. 5. 6. Antagonists of 5-HT3 Antagonists of D2 Antagonists of H1 Antagonists of M Receptors Antagonists of Neurokinin-1 Corticosteroids Dopaminergic Agents Haloperidol – Similar efficacy to ondansetron – Not approved for IV use secondary to cardiac arrhythmias Droperidol – Effective – Short half life-3 hours – Increased sedation – FDA black label Clinically Relevant? Study comparing ondansetron and droperidol QT prolongation Charbit B, et al. Anesthesiology. 2005. Dopamine Antagonists Metoclopramide – Prokinetic effects – Studies show 10mg dose no more effective than a placebo – Higher doses (50mg) may be effective – Dyskinetic and extrapyramidal side effects Other Drugs NOT Included in this Talk Metoclopramide Ranitidine Sodium citrate Omeprazole GERD and aspiration precautions are different from PONV 5HT-3 Antagonists Ondansetron, granisetron & dolasetron Work at the chemoreceptor trigger zone & at vagal afferents in the GI tract Anti-vomiting better than anti-nausea All three equal in efficacy, few side effects Four hour half-life, but genetic of polymorphisms of p450 can lead to ultra short metabolism Palonosetron (Aloxi) – RCT demonstrated efficacy – Approved for PONV in 2008 – Duration of up to 72 hours Anticholinergics Scopolamine patch showed to be equally effective to ondansetron Side effects include: – Dry mouth – Visual disturbances – Dizziness – Agitation Corticosteroids Dexamethasone Meta-analysis shows 8-10mg effective No reports of dexamethasone-related side effects in small doses Slow onset of action, better efficacy if given in the beginning of a case Antihistamines Dimenhydrinate (Dramamine) & Diphenhydramine Anticholinergic Properties Side effects: – – – – – – Sedation Dry Mouth Blurred vision Urinary Retention Prolonged recovery from anesthesia Vascular necrosis (promethazine) Neurokinin-1 Antagonists (Substance P Receptors) Work on the final common pathway from the emetic center Aprepitant (Emend) – Recent studies indicate more effective than ondansetron in preventing emesis, similar efficacy in preventing nausea – Patent expiration 2011-2015 Casopitant & Rolapitant Combinations versus single drugs Multiple RCT compare a combination of antiemetics versus a single agent Improved outcomes with combinations of anti-emetics (except for studies with metoclopramide) IMPACT International Multicenter Protocol to Assess Antiemetic Combinations, 2004 Large multicenter RCT 5,199 high risk patients Six Variables: 2x2x2x2x2x2 (64 groups) 1. Ondansetron 2. Dexamethasone 3. Droperidol 4. Air (versus NO) 5. Propofol (versus inhaled agents), 6. Remifentanil (versus fentanyl) Primary Outcome- PONV in 1st 24 hours Relative risk of combined antiemetics equal to multiplying the relative risk of each single agent together Apfel, C, et al. IMPACT. Anaesthetist. 2005. Algorithms for the prevention of PONV Risk adapted algorithms can reduce PONV in select patient populations None have proved to be universally applicable Guidelines for Antiemetic Therapy Patient Factors Surgical Factors •Female •H/o of PONV or motion sickness •Non-smoker •Use of opiods •Laparoscopy •Laparotomy •Craniotomy •Strabismus • ENT 1-2 Factors 1. 2. 3. 4. 5HT-3 Antag. Decadron Scopolamine Droperidol 2-4 Factors 1. Droperidol +5HT-3 Antag 2. Decadron+5HT-3 Antag. 3. Droperidol+Decadron >4 Factors Combination of antiemetics + TIVA with propofol Evidence Based Anesthesia Rescue Therapy Lack of data Mechanical Factors: – Secretions, gastric distension, opiates Choose a different drug class in the first six hours 5HT-3 Antagonists – Non-sedating – Better anti-vomiting than anti nausea – Not dose responsive – Not indicated if failed ondansetron prophylaxis Droperiol Dexamethasone Tulane Pharmacy Costs Wholesale Price Markup 5x wholesale price Submitted to Insurance Company Government Reimbursement for Operative Antiemetic Drugs Facility Surgery Fee DRUG WHOLE SALE INSTITUTION COST Ondansetron $0.78 $3.90 Ondansetron$4.08 $0.78 Droperidol per dose $20.40 Droperidol $4.08 Dimenhydrinate $0.04 Dimenhydrinate$0.04 $1.00 Scopolamine $11.90 $47.26 Dexamethasone $3.12 $15.60 Promethazine $0.54 $2.70 Prochlorperazine $3.60 $18.00 Courtesy of Bob Self, Tulane Pharmacy Director What does this mean? High risk patients ALWAYS warrant aggressive prophylaxis Ondansetron – 50 patients a day, 260 days a year…costs Tulane: $57,000 per year – Puts patients at risk for side effects Only 0.18% patients experience severe PONV requiring hospitalization…almost all can be identified by risk factors References Costanzo, Linda. Physiology. 4th Ed. Lippincott Williams & Wilkins: Philadelphia, 2007. Gan TJ. Risk factors for postoperative nausea and vomiting. Anesth Analog 2006;102:1884-98. Gan, T.J. Effective Management of PONV and Pain in Ambulatory Settings. Glidden, Randall. NMS Clinical Manuals. Lippincott Williams & Wilkins: Philadelphia, 2003. Habib, Ashraf. What Is the Best Strategy to Prevent Postoperative Nausea and Vomiting? Evidence-Based Practice of Anesthesiology. 2nd edition. Sunders Elsevier. 269-275. Kranke P. Algorithms for the prevention of postoperative nausea and vomiting: an efficacy and efficiency simulation. European Journal of Anaesthesiology 2007, 24,10:856-867. Kim, Eun Jin. Combination of Antiemetics for the Prevention of Postoperative Nausea and Vomiting in High Risk Patients. J Korean Med Sci 2007; 22:878-82. Apfel, CC. A Factorial Trial Six Interventions for the prevention of postoperative nausea and vomiting. Anaesthesist. 54 (3). Mar 2005. 201-9. Apfel CC., Kranke P, Katz MH, et al: Volatile Anesthetics may be the main cause of early, but not delayed postoperative vomiting: A randomized controlled trial of factorial design. Br J of Anesthesia. 88: 659-668, 2002. Apfel, CC, Korttila K, Abdallah M, et al.: A factorial Trial of Six interventions for postoperative nausea and vomiting. New England Journal of Medicine. 2004; 350, 2441-2451. Miller, R, et al. Miller’s Anesthesia. 7th ed. Churchill Livingstone: 2009. Kovac A. A randomized, double-blind controlled trial of three different doses of palonosetron versus placebo in preventing postoperative nausea and vomiting over a 72-hour period. Anesthesiology Analogue. 107 (2): 439-44. Charbit B, et al.. AnesthesioDroperidol and ondansetron-induced QT interval prologation: a clinical drug interaction studylogy. Aug 2008; 109 (2): 206-12.