Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
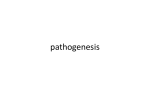
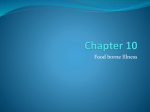
General Management of the Poisoned Patient Medical Student/Intern Lecture Emergency Medicine Who is a poisoned patient? • Sometimes it’s obvious and sometimes not • Poisoning is on the differential for almost every complaint • Having a general approach is useful Case Presentation • 15 year old female is brought in by parents 1 hour after a witnessed ingestion of “pain pills” • She appears drowsy • VS: T 98oF, HR 75, BP 120/70, RR 8, O2 Saturation 88% on room air • Her physical exam is remarkable for drowsiness, hypoventilation, and the following physical finding: Pinpoint pupils Questions • What toxidrome does this patient have? • What laboratory values are useful in the diagnosis of a poisoned patient? • Does she need GI decontamination? • What treatments may be beneficial at this point? History to Obtain • What was the toxin involved? Helpful but not absolutely required May send family/EMS back to scene • What was the time of ingestion? • If unknown, when was patient last seen? Interpretation of levels History • What toxins are around the house? Medications for others in the house including pets Over the counter preparations Cleaning supplies Chemicals in the garage or elsewhere Physical Findings • Some physical findings are of particular importance to toxicology Vital signs including temperature Pupillary size Skin – Dry or moist? Bowel sounds – diminished? Track marks? Pressure sores or compartment syndrome? Physical Findings • Is there a toxidrome present? Adrenergic or Sympathomimetic Cholinergic Anticholinergic Opioid • Many toxins fall into these broad categories • Treatment will be similar across any category Sympathomimetic Toxidrome • Excess of catecholamines • “Fight or Flight” response • Dilated pupils, tachycardia, hypertension, agitation/seizures, diaphoresis • Cocaine, amphetamines, “Ecstasy” or MDMA, Ritalin, caffeine, theophylline are examples of sympathomimetic agents Cholinergic Toxidrome • Excess of Acetylcholine • Sedation, pinpoint pupils, neuromuscular paralysis, bradycardia, SLUDGE syndrome, Salivation, Lacrimation, Urination, Defecation, GI motility, Emesis • Seen in organophosphate and carbamate insecticide poisoning Anticholinergic Toxidrome • Acetylcholine activity is blocked at muscarinic receptors leading to: Mad as a hatter – delirium and hallucinations Dry as a bone – dry skin Red as a beet – flushed skin Blind as a bat – widely dilated pupils Hot as Hades – low grade fever Also significant tachycardia • Seen with many prescription and OTC agents including antihistamines, phenothiazines, TCAs Opioid Toxidrome • Stimulation of opioid receptors • Triad of miosis, CNS depression, and hypoventilation • Agents that cause this include: heroin, morphine, hydrocodone and oxycodone Pinpoint pupils • Not many agents cause this finding COPS mnemonic C – Clonidine, Carbamates O – Opioids, organophosphates P – Phenothiazines S – Sedative/hypnotics Summary Syndrome Pupils Heart Skin rate GI motility Sympathomimetic (cocaine) large small Cholinergic (organophosphate) large Anticholinergic (diphenhydramine) Opioid (heroin) small up wet down down wet up up dry down normal normal down Toxidromes • If present, toxidromes may be helpful both diagnostically and therapeutically • Many toxins do not produce a classic toxidrome What toxidrome does our patient have? • • • • Pin point pupils Respiratory depression CNS depression Opioid toxidrome is present Diagnosis • What laboratory measures might be useful? • Is there an antidote? • Are extracorporeal removal measures effective or indicated? • Can we anticipate any complications that may develop? Use of the Laboratory Laboratory tests • Some “laboratory toxidromes” exist and have important implications for diagnosis and treatment Anion gap metabolic acidosis Sympathomimetic Sodium channel blockade • • • • • • • • Anion gap metabolic acidosis “MUDPILES” Methanol Notice how many of Uremia these are toxins Diabetic ketoacidosis Paraldehyde Iron, INH Lactic acidosis Ethylene glycol, Ethanol ketoacidosis Salicylates Sympathomimetic • Increased catecholamine surge will typically produce Hypokalemia Hyperglycemia Metabolic acidosis, low bicarbonate Potential rhabdomyolysis due to extreme agitation Sodium Channel Blockade • Prolongation of the QRS interval seen in many drug overdoses Tricyclic antidepressants Cocaine Propoxyphene Diphenhydramine • What starts out as QRS prolongation may degenerate into malignant ventricular dysrhythmias Sodium Channel Blockade 1 0 Na rushes in 2 3 4 Phase 0 corresponds to the QRS interval on ECG Sodium Channel Blockade 1 0 Na rushes in 2 3 Sodium channel blockade causes the phase 0 slope to be delayed resulting in prolongation of the QRS complex 4 Sodium channel blockers tend to give a rightward axis on ECG S in Lead I R in Lead aVR S in Lead aVL This is a “fingerprint” pattern for sodium channel blocker (such as TCA) toxicity What about urine drug screens? • • • • Limited value for intentional ingestions Rarely changes pt management Screens for drugs of abuse Tend to be sensitive not specific False (+) common • Reliance on them may mislead you For example, believing an opioid ingestion has been “ruled out” by a negative UDS Urine drug screens • Selective use • Altered mental status of unknown etiology • Pediatric cases of poisoning or suspected abuse • Seizures, MI? Specific drug levels • Acetaminophen level is indicated on ALL overdose patients Ubiquitous toxin with significant toxicity Asymptomatic presentation Easily treatable with time sensitive antidote • Specific drug levels may be indicated for some toxins Iron, theophylline, aspirin, phenytoin, digoxin for example Use of the Laboratory • There is no test for everything • Get a rapid glucose on all AMS pts • “Tox panel” includes Chemistry panel ECG APAP level UPT in females CPK in patients found down or agitated Specific drug levels when the toxin has easily measurable levels such as phenytoin Bedside diagnostic tests • Sometimes response to an antidote can be a diagnostic test Naloxone reverses opioid intoxication Physostigmine reverses anticholinergic intoxication Atropine improves cholinergic intoxication What labs should we get in our patient? • • • • • Chemistry panel ECG Acetaminophen level UPT Would a urine drug screen be helpful? Probably not Is there a bedside test we can perform here? • Naloxone administration • In opioid intoxication will have a dramatic and rapid response • Small dose in opioid addicts as this may precipitate withdrawal • Our patient receives 1.0 mg of naloxone IV and has a dramatic response Decontamination GI Decontamination • • • • • • Ipecac Gastric lavage Activated charcoal Multidose activated charcoal Whole bowel lavage Supportive care Syrup of Ipecac • Induces emesis within 20-30 minutes of administration • Old recommendations: Every household should have a bottle • New recommendations: Probably very few indications for syrup of ipecac • Studies have shown that SOI removes a variable amount of ingested toxin, no improvement in outcomes Syrup of Ipecac • Refractory emesis may preclude administration of other therapies Activated charcoal Oral N-acetylcysteine • For some toxins, onset or presence of vomiting important clinically. Ipecac will mask these findings Iron, theophylline Mushroom intoxication Gastric Lavage • Attractive idea • Pills are not likely to fit through the tube • 40 french tube • Not associated with improved outcomes • Can remove some drug within 1 hr • Complications include esophageal perforation and aspiration pneumonia 40 French tube Gastric Lavage • Consider for: Life threatening ingestion Within one hour post ingestion Toxin without an effective treatment • Generally used less as studies show limited benefit and nontrivial complication rate Activated Charcoal • Large surface area • Adsorbs to toxins and prevents absorption in the GI tract • Complications include bowel obstruction, vomiting with aspiration Activated Charcoal PHAILS to be effective in: • Pesticides • Hydrocarbons • Alcohols • Iron • Lithium • Solvents When to use Activated Charcoal? • • • • • • 1-2 hours post ingestion Ingestion expected to produce toxicity Substance known to adsorb to charcoal Benefits felt to exceed risks 1 gram/kg typical dose + sorbitol Multidose or late charcoal for: Theophylline overdose Evidence of continuing absorption late • Aspirin or SR preparations) Cocaine body packers Whole Bowel Irrigation • Administration of large amounts of GoLightly via NG tube • Flush the toxin out of the system • Run until clear effluent • No proven clinical advantage • Rarely used Whole Bowel Irrigation • May consider in rare cases where lethal doses of toxin are in the GI tract and continuing absorption suspected Cocaine body packers Sustained released cardiac toxins such as calcium channel blockers • Consider toxicology consult before beginning this therapy Does our patient need GI Decontamination? • Ipecac? No • Lavage? Probably not • Activated charcoal? Possibly Watch CNS status to prevent aspiration Medical Management • • • • • ABC’s GI decontamination when indicated Watch for complications Supportive care Antidotal therapy Complications of overdose Aspiration pneumonia • Obtunded patients cannot protect their airway • Toxins cause emesis • Good airway management can be preventive Rhabdomyolysis • Agitation leads to muscle breakdown • CNS depression leads to 8 Hours a muscle crush injury or Later…. compartment syndrome Patients “found down” • Good hydration • Follow CPK’s • Clue: RBC on urine dip but none on microscopic Anoxia • Anoxic brain and organ injury due to CNS depression, hypotension, hypoventilation with hypoxia • End organ damage Renal failure Myocardial infarction Ischemic CVA “The big three” • • • • Aspiration pneumonia Rhabdomyolysis Anoxia Cause most of the morbidity and mortality from overdoses • Particularly seen in “found down” patients A note on seizures… • Toxin induced seizures may require specific therapy Pyridoxine in Isoniazid overdose • Benzodiazepines and barbiturates are the first line agents to treat toxin induced seizures • Phenytoin often not effective Labs return on the patient: • Chemistry panel is normal • UPT is negative • ECG is normal sinus rhythm with normal intervals • Acetaminophen level is 250 mcg/ml Now what? Is specific antidotal therapy indicated? Antidotal therapy Toxin Acetaminophen Arsenic Beta blockers Black widow spider toxin Calcium channel blockers Cyanide Digoxin Ethylene glycol, methanol Iron Isoniazid Lead Methemoglobinemia Opioids Organophosphates Salicylates Thallium Tricyclic antidepressants Valproic acid hepatotoxicity Antidote N-acetylcysteine DMSA Glucagon Specific antivenin Calcium, glucagon, Insulin/glucose Amyl nitrite, sodium thiosulfate, sodium nitrite Digibind (Fab fragments) Ethanol, fomepizole Deferoxamine Pyridoxine EDTA, DMSA, BAL Methylene blue Naloxone Atropine, pralidoxime Sodium bicarbonate Prussian Blue Sodium bicarbonate Carnitine Antidotal therapy • Reverse or counteract the effects of poison • Competitive antagonist Narcan for opioids • Receptor agonist Calcium for calcium channel blocker • Inhibit metabolism Fomepizole for ethylene glycol • Bind/remove toxin Digibind for digoxin • Reactivate enzymes Pralidoxime for organophosphates • However most toxins do not have an antidote Our patient has an elevated acetaminophen level. Should we treat her? Acetaminophen • Toxic via a metabolite formed by p450 metabolism • Minimum dose to cause toxicity 7.5 gm or 150 mg/kg in adult 200 mg/kg in children Acetaminophen metabolism O HN Glucuronide 40-65% 20-45% Sulfate (increased in children) OH Acetaminophen Glutathione Normally Detoxifies NAPQI Mercapturic acid (nontoxic) P450 mixed function oxidase (5-15%) Unchanged in urine O N Glutathione O NAPQI Hepatic adduct formation, cell death Centrilobular necrosis Phases of acetaminophen toxicity • Phase I (0.5-24 hour) – nausea, anorexia, malaise • Phase II (24-72 hour) – “quiescent” phase, LFT’s start to rise, RUQ pain • Phase III (72-96 hour) – Hepatic necrosis, jaundice, encephalopathy Most deaths occur here • Phase IV (4 days–2 weeks) - recovery Hepatotoxicity • NAPQI binds to cell proteins and leads to cell death • Why centrilobular? This area contains the most p450 and the least glutathione • Liver and kidneys contain p450 • Injury is evident once glutathione stores reach 30% of baseline What decision rule can help us decide whether or not to treat a patient with an acute acetaminophen ingestion? Rumack-Matthew Nomogram • Sensitive predictor of hepatotoxicity • Failure rate approaches zero over the past 25 years of use • Useful only with levels obtained between 4 - 24 hours post ingestion • Single acute ingestion N-acetylcysteine (NAC) is antidotal Repletes glutathione Mucomyst® for oral use Acetadote® for IV infusion Dosing • Oral NAC 140 mg/kg loading dose then 70 mg/kg q4 hours for 17 more doses Must dilute at least 1:1 due to taste • IV NAC 150 mg/kg over 1 hr, 50 mg/kg over 4 hr, then 16 mg/kg over 16 hours, continue if needed Call Poison Control, pharmacy, or toxicology for dosing Does our patient need to be loaded with NAC? • • • • Initial level was 1 hour post ingestion Need a 4 hour level to plot on nomogram If it is toxic, start NAC Treatment < 8 hours post ingestion virtually eliminates hepatotoxicity Can wait on the 4 hour level prior to NAC administration in early presenter The 4 hour level is 160 µg/ml… This falls above the treatment line on the Rumack-Matthew nomogram therefore antidotal therapy is indicated 200 150 Log [Serum] µg/ml 6.25 24 4 Time (hours) Case Presentation 6 year old male with an accidental ingestion of Tofranil presents to the PICU comatose, hypotensive, with this rhythm. Questions • What kind of rhythm is this? Wide complex tachycardia • What kind of drug is Tofranil? Imipramine, a tricyclic antidepressant • What is the mechanism for the wide complex tachycardia? Sodium channel blockade • What antidote may be useful? Sodium bicarbonate Treatment With Na+ Bicarbonate One minute after 100 mEq sodium bicarbonate Bicarbonate as an antidote • Used for cardiac toxicity due to sodium channel blocking agents Tricyclic antidepressants Cocaine Class I antiarrhythmics Phenothiazines • Indications: Wide QRS >100-120 ms Dysrhythmias Hypotension Bicarbonate as an antidote • Alkalinization of serum may help with specific toxins Salicylates – facilitates elimination and keeps toxin out of the tissues Tricyclic antidepressants Methanol intoxication What makes a toxin dialyzable? • Small size • Less protein binding • Small volume of distribution More in serum, less in tissues • Charge Dialyzable Toxins • • • • Salicylates Theophylline Lithium Alcohols Pediatric considerations • Beware of the accidental ingestion in children less than 5 years old • Some detective work may be required to determine the toxin involved • Children are more susceptible to some toxic effects such as methemoglobinemia, hypoglycemia, seizures, dysrhythmias Pediatric considerations • “One pill can kill” a child Calcium channel blockers Beta blockers Sulfonylureas MAO inhibitors Cyclic antidepressants Methemoglobin inducers (pyridium, dapsone) Theophylline Pediatric considerations • High morbidity and mortality in pediatric ingestion Hydrocarbons such as lamp oil Insecticides Methyl salicylate • oil of wintergreen, ben-gay Caustic agents • household cleaners The Poison Center as a Resource 1-800-222-1222 962-2323 • Open 24/7 • Provides information to the public and health care providers On drugs, plants, chemicals, venoms, etc. • RNs and Pharmacists • Medical Back-up • Resources Computer database MEDLINE Take Home Points • Toxidromes are helpful if recognized • GI decontamination may be useful • Understand the role of laboratory APAP, Chem-7 and ECG on every overdose • Supportive care and recognize complications • Antidotal therapy in selected cases • Know your resources! Any questions?