Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
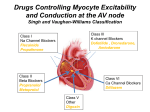
- Antiarrhythmic Agents - AV node Normal heartbeat and atrial arrhythmia Normal rhythm Atrial arrhythmia AV septum 0 1 2 3 4 Determination of pacemaker rate - 1- more negative maximum diastolic potential, from -80 to -100mV: Vagal AC-chol. discharge. 2- reduction of the slope of diastolic depolarization: b-Blockers. increase slope:NEP, low K+, fiber stretch, acidosis and injury: increase slope More positive threshold potential, from -65 to -45mV. Not common, prolongation of the action potential duration. - Abnormalities of Cardiac Impulses atrial fibrillation Ventricular fibrillation (VF) Ventricular tachycardia (VT) Wolff-Parkinson-White syndrome Supraventricular tachycardias (SVT) Effects of Class IA, IB, and IC antiarrhythmics on the ventricular action potential Class I antiarrhythmics (Na +channel blockers) act on ventricular myocytes to decrease re-entry. All subclasses of the class I antiarrhythmics block the Na +channel to some degree: class IA agents exhibit moderate Na +channel block, class IB agents rapidly bind to (block) and dissociate from (unblock) Na + channels, and class IC agents produce marked Na +channel block. Class IA, IB, and IC agents also differ in the degree to which they affect the duration of the ventricular action potential Summary of Antiarrhythmic classes Contraction of ventricles ECG (EKG): wave segments IC Repolarization of ventricles Contraction of atria Class I: Na+ channel blockers Class II: B-Blockers Class III: K+ channel blockers Class IV: Ca+ channel blockers IA III II IV - Cardiac arrythmias Occurs in 25% treated with digitalis 50% of anesthetized patient 80% of patients with acute myocardial infraction Need treatment because: Too rapid or too slow or asynchronous reduce cardiac output…. - Cardiac Electrophysiology Transmembrane potential -- determined primarily by three ionic gradients: Na+, K+, Ca 2+ water-soluble, -- not free to diffuse through the membrane in response to concentration or electrical gradients: depended upon membrane channels (proteins) Movement through channels depend on controlling "molecular gates" Gate-status controlled by: Ionic conditions Metabolic conditions Transmembrane voltage - Determination of pacemaker rate - 1- more negative maximum diastolic potential, from -80 to -100mV: Vagal AC-chol. discharge. 2- reduction of the slope of diastolic depolarization: b-Blockers. increase slope:NEP, low K+, fiber stretch, acidosis and injury: increase slope More positive threshold potential, from -65 to -45mV. Not common, prolongation of the action potential duration. - Factors that may precipitate or exacerbate arrhythmias Ischemia Hypoxia Acidosis Alkalosis Abnormal electrolytes Excessive catecholamine levels Autonomic nervous system effects (e.g., excess vagal tone) Drug effects: e.g., antiarrhythmic drugs may cause arrhythmias) Cardiac fiber stretching (as may occur with ventricular dilatation in congestive heart failure) Presence of scarred/diseased tissue which have altered electrical conduction properties - Factors that can increase automaticity: hypokalemia cardiac fiber stretch beta-adrenergic receptor activation injury currents acidosis Antiarrhthmic Drug Classes - Antiarrhthmic Drug Classes Class I: Sodium Channel Blockers: Class II: Beta-Adrenergic Antagonists: Propranolol Esmolol Class III: K+ Channel Blockers: Disopyramide Procainamide Quinidine Mexiletine Amiodorone Dofetilide Ibutilide Class IV: Ca+ channel blockers Diltiazem Verapamil - - Antiarrhthmic Drug Classes Class I: Sodium Channel Blockers Class IA: (effective in treating Sinoatrial lessventricular arrhythmias) Quinidine Procainamide Disopyramide. Class IB: (effective in treating ventricular arrhythmias) Lidocaine Mexiletine Tocainidine Phenytoin. - Quinidine: Metabolism Hepatic: hydroxylation to inactive metabolites; followed by renal excretion 20% excreted unchanged in urine Impaired hepatic/renal function: accumulation of quinidine and metabolites Sensitive to enzyme induction by other agents- decreased quinidine blood levels with phenytoin, phenobarbital, rifampin - Amiodarone (Cordarone) (Class I and III Channel Blocker) - Amiodarone Mechanism of Action Blocks sodium and potassium channels and prolongs action potential duration. Prolongs effective refractory period in: SA node AV node ventricle atrium His-Purkinje system accessory bypass tracts (Wolff-ParkinsonWhite syndrome) - Amiodarone Vascular Effects Noncompetitive a and b adrenergic receptor blocker Systemic vasodilation Antianginal properties, secondary to coronary vasodilation - Amiodarone Approved for use only in treatment of serious ventricular arrhythmias (USA) also used for refractory supraventricular arrhythmias Numerous adverse effects. - Amiodarone Metabolism & Excretion Long elimination halftime: 29 days Minimal renal excretion Extensive protein binding Amiodarone concentrated in the myocardium (10-50 times plasma concentration) - Amiodarone: Side Effects Pulmonary: Most serious adverse effect seen in long-term therapy is a rapidly progressive pulmonary fibrosis which may be fatal Frequency: 5%-15% treated patients Mortality rate: 5% to 10% Cause: unknown (possibly related to amiodarone-mediated generation of free oxygen radicals in the lung) Two types of amiodarone-pulmonary toxicity clinical presentations: More common: Slow, insidious, progressive dyspnea, cough, weight loss, pulmonary infiltration (chest x-ray) Acute onset: dyspnea, cough, arterial hypoxemia. Class II: Beta-Adrenergic Antagonists Class II Antiarrhythmic drugs Propranolol (Inderal) Metoprolol (Lopressor) (beta-1 "specific") Pindolol (Visken) (partial agonist) Esmolol (Brevibloc)(very short acting) - - Class III: Potassium Channel Blockers - Bretylium (Bretylol) - Class IV: Calcium Channel Blockers Verapamil Diltiazem & Bepridil - Antiarrhthmic Drug Classes Class I: Sodium Channel Blockers Class II: Beta-Adrenergic Antagonists Class III: prolongation of AP Class IV: Ca+ channel blockers - Antiarrhthmic Drug Classes Class I: Sodium Channel Blockers: Class II: Beta-Adrenergic Antagonists: Propranolol Esmolol Class III: K+ Channel Blockers: Disopyramide Procainamide Quinidine Mexiletine Amiodorone Dofetilide Ibutilide Class IV: Ca+ channel blockers Diltiazem Verapamil THE END