Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Polysubstance dependence wikipedia , lookup
Drug interaction wikipedia , lookup
Drug discovery wikipedia , lookup
Pharmacokinetics wikipedia , lookup
National Institute for Health and Care Excellence wikipedia , lookup
Pharmacognosy wikipedia , lookup
Pharmaceutical industry wikipedia , lookup
Adherence (medicine) wikipedia , lookup
Prescription costs wikipedia , lookup
Neuropsychopharmacology wikipedia , lookup
Clinical trial wikipedia , lookup
Ciprofloxacin wikipedia , lookup
Pharmacogenomics wikipedia , lookup
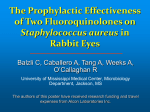
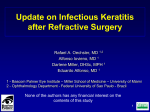
Ongoing trials with new drugs/regimens: the fluoroquinolone case J. Grosset, E. Nuermberger & R.Chaisson Center for TB Research, Johns Hopkins University 1. What are fluoroquinolones ? 2. What is the experimental antituberculosis activity of fluoroquinolones ? 3. What information is available on the antituberculosis activity of fluoroquinolones in humans ? 4. What are the ethical issues in clinical trials with fluoroquinolones? 1. Fluoroquinolones Fluoroquinolones are synthetic antimicrobial agents derived from nalidixic acid and characterized by a fluorine atom at position 6 : - Ciprofloxacin (C) - Ofloxacin (O) - Levofloxacin (L) - Sparfloxacin (S) - Moxifloxacin (M) - Gatifloxacin (G) 2 µg/ml 2.1. MICs (μg/ml) of main quinolones against M. tuberculosis 2.2. Comparative pharmacokinetics and pharmacodynamics of fluoroquinolones after single oral dose in humans* Drug Pharmacokinetics Pharmacodynamics Dose (mg/kg) Cmax (µg/ml) AUC24 (mg.h/L) MIC90 (µg/ml) CMax/MIC90 AUC24/MIC90 Ciprofloxacin 250 (4.1) 500 (8.3) 1.5 ± 0.43 1.9 ± 2.9 5.75 ± 1.25 10-19 1.0 1-2 2-3 5-6 10-20 Ofloxacin 400 (6.6) 600 (10) 4 11 48 58 2.0 2 5 24 29 Levofloxacin 500 (8.3) 6.21 ±1.34 44.8 1.0 5.7 40-50 Sparfloxacin 200 (3.3) 400(6.6) 0.70 1.18 18.7 33 0.5 2 2-4 40 66 Moxifloxacin 100 (1.4) 400 (6.6) 0.43 ±1.23 4.34 ± 1.61 6.18 ± 1.18 39.3 ± 5.35 0.5 1 9 12-15 80 Gatifloxacin 400 (6.6) 3.42 ± 0.74 30 ± 3.8 0.5 7 60 * from Hooper et Wolfson, 1985; Siefert et al., 1999; Hooper, 2000; Lubasch et al., 2000; Wright et al., 2000; Schentag et al., 2001. 2.3. Antituberculosis activity of fluoroquinolones in mice Change in log10 spleen CFU Bactericidal activity of fluoroquinolones alone against M. tuberculosis in mice 1.5 1 0.5 0 -0.5 -1 -1.5 -2 -2.5 -3 -3.5 Control INH 25 INH 25 O 150 Levo 150 Spar 50 Spar 50 Moxi 100 0 1 2 3 4 Weeks of treatment Ji et al, AAC (1995); 39:1341 Ji et al, AAC (1998); 42:2066 2.4. Conclusions from experimental data 1. Among all fluoroquinolones, MXF has the most favorable PK/PD parameters 2. Used alone in the mouse model, MXF has the most potent bactericidal activity among all fluoroquinolones 3. The bactericidal activity of MXF is close to that of INH 3a.Activity of fluoroquinolones in humans • In 1985, Tsukamura et al., treated 19 patients with ofloxacin alone for 6 to 9 months: 5 became culture negative. No side-effect. • Many anecdotal reports confirmed these findings. • In 1993, ATS and CDC noted that fluoroquinolones might be active for MDR-TB treatment. • In 2003, ATS/CDC guidelines recommended fluoroquinolones for MDR-TB treatment but not as first-line agents. Why? 3b.Why fluoroquinolones were not recommended as first-line agents? • All EBA study with fluoroquinolones other than MXF failed to demonstrate powerful activity • The addition of a fluoroquinolone to the standard regimen failed to demonstrate benefit in terms of time to culture conversion and relapse rate. • However, in a trial (TRC Chennai 2002),the addition of ofloxacin to the standard regimen and the shortening of treatment duration to 4 and 5 months was gave positive results. But this trial raised ethical issues. 4. Ethical Rules for Clinical Trials • Autonomy - consent of the patient • Beneficence – the patients should benefit, or at least not suffer, from being in the trial • Equipoise – when randomizing, the investigators must be equally comfortable with the alternative treatment arms • Justice – the benefits and burdens of research should be shared fairly to the extent possible In practice 1. Basic fact: the present 6-month standard regimen CAN cure 100% of newly diagnosed patients with drug susceptible organisms and regular intake of drugs 2. Consequently, 1st. Patients should not be deprived of a 100% active treatment 2nd. Patients should not be exposed to undue risks of toxicity 3rd. The trial should be scientifically founded (prerequisite experimental & clinical evidence) 4th. The trial should be scientifically designed and performed 4.1. No risk of depriving patients from an active treatment Any deviation in the drug content and the duration of the standard treatment is unacceptable without solid scientific experimental/clinical evidence . For example, there is no evidence* that (i) the duration of treatment might be reduced, and (ii) the time to smear and culture conversion is shortened with the use of any new drug * Possibility is not evidence 4.2. No exposition to undue risk of toxicity • Except in a 6-month study conducted in Italy with no side effect (Valerio et al., 2003), MXF has not been given for several weeks or months • Therefore, preliminary studies in which MXF is substituted for ethambutol are now in progress (CDC, Johns Hopkins) with two primary end-points: culture conversion within two months and safety/tolerability. 4.3. The trial should be scientifically founded • On experimental data • On clinical data Both should provide rationale for undertaking of the trial Moxifloxacin (MXF) in combination with first-line agents Aim of the experiment: determine the effect of 1. The addition of MXF to the standard regimen, 2RHZ/4RH. 2. The substitution of MXF for each of the individual components of the standard regimen. L 1 u n g C F U c o u n t s 0 9 8 7 U n 2 2 t r e a t R H Z + R H Z M e d 4MRH + 2 RM Z+ 4 RM 2 Z M H+ 4 M H 6 4 R + H 4 R H M 5 2 R H 4 3 Log CFU in entire lung 2 1 0 0 1 D u r 2 a t i o n 3 o f t r e a 4 t m e n 5 t ( m o s 6 . ) Results of log10 CFU counts from lung homogenates. Early Bactericidal Activity (EBA) of Drugs in Pulmonary Tuberculosis (Fall in log10 CFU counts during the first 2 days) Authors INH RIF MXF Hafner et al.,1997 Gosling et al., 2003 Pletz et al., 2003 0.57 - - 0.77 0.28 0.53 0.40 - 0.54 Consequences of scientific foundation • CDC is working with the Russian Research Institute for Phthisio-pulmonology to implement a phase II to evaluate MXF in place of isoniazid in the initial phase of treatment (Time to culture conversion, Safety/tolerability) • Investigators at Johns Hopkins are also developing a similar approach 4.4. The trial should be scientifically designed and performed The protocol should follow the rules of controlled clinical trial : - Control group - Adequate number of patients to obtain significant results - Adequate organization of drug intake, and clinical and laboratory monitoring - Definition of primary and secondary end- point Conclusions • At long last (R. O’Brien, 2003), improving treatment of tuberculosis is more than a distant dream. • For such a dream not to be a nightmare for some patients, all investigators should comply with ethical rules. Alligato gozaimasu FIN END