Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Pharmaceutical marketing wikipedia , lookup
Specialty drugs in the United States wikipedia , lookup
Electronic prescribing wikipedia , lookup
Compounding wikipedia , lookup
Orphan drug wikipedia , lookup
Polysubstance dependence wikipedia , lookup
Drug design wikipedia , lookup
Drug discovery wikipedia , lookup
Neuropsychopharmacology wikipedia , lookup
Neuropharmacology wikipedia , lookup
Pharmaceutical industry wikipedia , lookup
Pharmacognosy wikipedia , lookup
Prescription costs wikipedia , lookup
Psychopharmacology wikipedia , lookup
Pharmacokinetics wikipedia , lookup
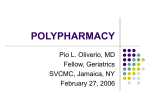
Geriatric Polypharmacy, The Good The Bad And The Ugly John Kashani DO Staff Toxicologist, New Jersey Poison Center Attending, St. Joseph’s Regional Medical Center Objectives • Discuss the epidemiology of the aging population • Discuss polypharmacy and adverse drug reactions • Outline pharmacokinetics as it relates to the aging population Objectives • Outline potentially inappropriate medications for the elderly population • Discuss clinically significant drug interactions • Provide a rational approach to elderly medication prescribing • Illustrate polypharmacy cases Introduction • Over 30 new medications are introduced each year • Recognizing drug interactions is a daily challenge and is becoming increasingly more difficult • Multiple drug regimes carry the risk of adverse interactions Introduction • Precipitant drugs modify the object drugs absorption, distribution, metabolism, excretion or clinical effect • Additionally, newly introduced medications, and medications with new indications may have multiple pharmacologic effects Introduction • The population is steadily aging: – Greater than 65 years old • 12% of the United States Population • 43% of Emergency Department • 48% of critical care admissions Introduction • 2003 Poison Center exposures – Increases fatality ratio – Greatest among those 80 years or older • May be grossly underestimated Introduction • The elderly are prescribed more drugs • 32% of prescriptions – Cardiovascular disease – Arthritis – Gastrointestinal disorders – Bladder dysfunction Introduction • Average use for persons 65 years or older: – 2 to 6 prescription drugs and 1 to 3.4 over-the-counter medicines • Average American senior spends $670/year for pharmaceuticals Polypharmacy • Polypharmacy means "many drugs“ • The use of more medication than is clinically indicated or warranted • 5 or more drugs Adverse Drug Reaction • The most consistent risk factor for adverse drug reactions (ADRs) is the number of drugs being taken – Risk rises exponentially as the number of drugs increases Adverse Drug Reaction ADRs occur as a result of 1. Drug-drug interactions 2. Drug-disease interactions 3. Drug-food interactions 4. Drug side effects 5. Drug toxicity Polypharmacy • Polypharmacy leads to: – More adverse drug reactions • Patient outcomes – Poor quality of life – High rate of symptomatology – (Unnecessary) drug exposure/expense Consequences: Quality of Life • In ambulatory elderly: 35% experience ADRs and 29% require medical intervention • In nursing facilities: 2/3 of residents experience ADRs • Up to 30% of elderly hospital admissions involve ADRs *Beers MH. Arch Internal Med. 2003 “If medication related problems were ranked as a disease, it would be the fifth leading cause of death in the US!” *Beers MH. Arch Internal Med. 2003 Pharmacokinetics and Aging – Absorption – Distribution – Metabolism – Excretion Pharmacokinetics and Aging • Absorption: – Age-related gastrointestinal tract and skin changes seem to be of minor clinical significance for medication usage Pharmacokinetics and Aging • Distribution: – Important Age-Related Changes: • Decrease in Lean Body Mass and total body water • Increased percentage Body Fat Pharmacokinetics and Aging • Increase in volume of distribution for lipophilic drugs – Protein Binding changes are of modest significance for most drugs, especially at steady-state • Volume of distribution (Vd) – Apparent volume the drug is dissolved in – Measured in Liters or Liters/Kg • not a real volume Pharmacokinetics and Aging • Metabolism: – Though liver function tests are unchanged with age, there is some overall decline in metabolic capacity – Decreased liver mass and hepatic blood flow Pharmacokinetics and Aging • Hepatic conjugation – Inactive metabolites • Hepatic oxidation – Active metabolites Pharmacokinetics and Aging • Renal Excretion: – Age-related decreased renal blood flow and GFR is well-established – Decreased lean body mass leads to decreased creatinine production Pharmacokinetics and Aging Cr clearance=(140-age)(IBW)/creatinine(72) (multiply by 0.85 for women) Example: “70kg” 75 year old man Cr Clearance= (140-75)(70)/1.0(72)=63 Pharmacodynamics and Aging • Generally, lower drug doses are required to achieve the same effect with advancing age – Receptor numbers, affinity, or postreceptor cellular effects may change – Changes in homeostatic mechanisms can increase or decrease drug sensitivity Avoiding Polypharmamcy – Avoid automatic refills – Look for other sources of medications ie. OTC – Caution with multiple providers – Don’t use medications to treat side effects of other meds – What can you discontinue or substitute for safer medication? Vitamin and Herbal Use in Older Adults • Highly prevalent among older adults • Generally not reported to the physician • Some serious drug interactions are possible: – Warfarin: gingko biloba, vitamin E – SSRI’s: St. Johns Wort (Potentially)Inappropriate Medications for Older Adults * • • • • • Propoxephene Diphenhydramine Amitryptiline Alprazolam Diazepam * Beers, MH et al. Arch Intern Med 151:1825,1991. Polypharmacy in the Making… • Drug reactions in the elderly often produce effects that simulate the conventional image of growing old: unsteadiness dizziness confusion nervousness fatigue insomnia drowsiness falls depression incontinence malaise Polypharmacy in the Making… • Avoid treating adverse reactions/side effects of drug with more drugs! – Dizziness from anti-hypertensive treated with meclizine – Edema from a calcium-channel blocker treated with furosemide and KCL Polypharmacy in the Making… • Drugs most frequently associated with adverse reactions in the elderly: – psychotropic drugs – anti-hypertensive agents – diuretics – digoxin Polypharmacy in the Making… – NSAIDS – corticosteroids – warfarin – theophylline Warfarin • Drugs that inhibit warfarin's metabolism include ciprofloxacin (Cipro), clarithromycin (Biaxin), erythromycin, metronidazole (Flagyl) and trimethoprim-sulfamethoxazole (Bactrim, Septra) • Acetaminophen Warfarin • Aspirin • Nonsteroidal Anti-inflammatory Drugs Fluoroquinolones • Divalent cations (calcium and magnesium) and trivalent cations (aluminum and ferrous sulfate) Antiepileptic Drugs • Carbamazepine (Tegretol), phenobarbital and phenytoin (Dilantin) – CYP450 interactions 2D6/3A4 • Fluoxetine (Prozac) Paroxetine (Paxil) Sertraline (Zoloft) • Cimetidine (Tagamet) Clarithromycin (Biaxin) Erythromycin Fluvoxamine (Luvox) Grapefruit juice Itraconazole (Sporanox) Ketoconazole (Nizoral) Lovastatin (Mevacor) Nefazodone (Serzone)Cisapride (Propulsid) Lithium • Diuretics • Ace Inhibitors • NSAIDS Sildenafil • Nitrates 3-Hydroxy-3-Methylglutaryl Coenzyme A Reductase Inhibitors • Concomitant use of statins and erythromycin, itraconazole, niacin or gemfibrozil (Lopid) can cause toxicity that manifests as elevated serum transaminase levels, myopathy, rhabdomyolysis and acute renal failure Serotonergic Agents • • • • • • Inhibit 5-HT uptake Enhances 5-HT release Inhibits 5-HT breakdown Metabolized to 5-HT 5-HT1A agonist Enhances 5-HT receptor response to stimulation Case 1 80 year old widow who now lives with her daughter comes to Emergency Department complaining of being a nervous wreck and not being able to “turn off her mind for the past 2 yrs”. She brings with her a bag of all her meds Case 1 PMHx: CHF, irritable bowel syndrome, depression, HTN, recurrent UTIs, stress incontinence, anemia, occipital headaches, osteoarthritis, generalized weakness Case 1 Meds: sucralfate, Cimetidine, enteric ASA, Atenolol, Digoxin, Alprazolam, Naproxen, Oxybutynin, Dicyclomine TID, Lasix, Tylenol #2, Verapramil Medication Red Flags: • High risk drugs: alprazolam, oxybutynin, tylenol #2, dicyclomine, NSAIDS • Digoxin P-Glycoproteins, Digoxin and polypharmacy Small Intestine Biliary Excretion * * Lumen Enterocyte Bile Hepatocyte Plasma Renal Tubular Secretion * Urine Tubular Cell Plasma Plasma P-Glycoproteins • Inhibitors – Amiodarone – Clarithromycin – Cyclosporine – Diltiazem – Erythromycin – Ketocanazole – Quinidine – Verapramil – tacrolimus • Inducers – Rifampin – St. John’s Wort – Dexamethasone – Indinavir – Ritonavir – Retonoic acid – Morphine – Phenothiazine – clotrimazole Medication Red Flags: • naproxen and aspirin carry the potential drug related adverse events of gastritis/GIB and sucralfate and cimetidine are being used to treat these side effects Case 2 Mrs. Jones is a 72 yr living in an assisted living facility where she has been recently complaining of increasing confusion, lightheadedness in the am and difficulty sleeping at night Case 2 PMHx: CHF, NIDDM, OA, glaucoma, depression, and stress incontinence Meds: Digoxin, Furosemide, Timolol gtts, Metformin, Ibuprofen, Paroxetine, Oxybutynin,Propoxyphene/apapprn, and Diphenhydramine Medication Red Flags: • Diphenhydramine: sedative, anticholinergic properties • Oxybutynin: anticholinergic Propoxyphene - narcotic • Digoxin Case 3 Mr. Wilson is a 81 yr who had an URI and subsequently was admitted for acute confusion and disorientation. He then began wandering and having hallucinations while spiking a fever. Case 3 PMHx: CAD with MI, COPD, DJD, Hypothyroidism, Depression/anxiety, chronic anemia and diarrhea, aortic valve replacement, gout, neuropathy, bilateral total knee replacements Case 3 • Meds: aggrenox, neurontin, theophylline, synthroid, allopurinol, prozac, combivent, colchicine, Imodium prn, metamucil, calcium, iron, multivitamin, codeine Case 3 • Medical workup: significant for negative head CT, EKG with no acute changes, UA, CBC, LP, Chem10, CXR shows possible RLL infiltrate Medication Red Flags: • Theophylline: low therapeutic index • Iron deficiency anemia is more rare in men, so check levels and maybe discontinue supplement • Chronic diarrhea: iatrogenic? From colchicine? Also Imodium is anticholinergic Prescribing Pearls • Use single daily dose regimens • Limit the use of PRN medications • Consider all new medicines as a therapeutic trial Prescribing Pearls • Discontinue a drug if it is ineffective or intolerable adverse effects occur • Provide legible written instructions • Instruct caregivers as needed Patient Education • Use one pharmacist/pharmacy • Use your PCP as intended…avoid seeing multiple physicians • Do not use medications from others • Report symptoms • All medicines, even over-the-counter, have adverse effects • Report all products used Ways to Decrease Drug Costs • Generics ok • Change dosing regimen • Older drugs, e.g. beta blockers, diuretics, acetaminophen • Double duty drugs, e.g. beta and alpha blockers, ACE-inhibitors • Avoid non-regulated products Geriatric Rx Principles • • • • First consider non-drug therapies Match drugs to specific diagnoses Reduce meds when ever possible Avoid using a drug to treat side effects of another Geriatric Rx Principles • Review meds regularly (at least q3 months) • Avoid drugs with similar actions/same class • Clearly communicate with pt and caregivers • Consider cost of meds! Avoiding Polypharmamcy • Avoid automatic refills • Look for other sources of medications ie. OTC • Caution with multiple providers • Don’t use medications to treat side effects of other meds • What can you discontinue or substitute for safer medication? Summary • Polypharmacy and ADRs have profound medical and economic consequences • Elderly have unique pharmacokinetics predisposing them to drug toxicity • High risk medications include cardiovascular, analgesic, psychotropics, and meds with a low therapeutic index Summary • Drug toxicity may be masquerading as an illness • Be a patient advocate! It may be you one day… References 1. 2. 3. 4. 5. 6. 7. 8. Swanson’s Family Practice Review. Fourth Ed. A. Tallia, D. Cardone, D. Howarth, K Ibsen; Mosby 2001. Geriatrics: 20 common problems. A. Adelman, M. Daly; McGraw Hill 2001. Primary Care Geriatrics: A Case- Based Approach. Third Ed. R. Ham, P. Sloane; Mosby 1997. Essentials of Clinical Geriatrics. Fourth Ed. RL Kane, JG Ouslander, IB Abrass; McGraw Hill 1999. Polypharmacy. Didactic at SFM by Dr. Pat Borman Holland EG, Degruy FV. Drug- Induced Disorders. American Family Physician Vol 56, Nov 1, 1997. Beers MH. Updating the Beers Crieria for 003Potentially Inappropriate Medication Use in Older Adults. Arch Internal Med. 2003: 2716-2724. Personal Medical Record developed by Dr. Eric Coleman, UCHSC, HCPR : http://caretransitions.org/document/phr.pdf