Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Remote ischemic conditioning wikipedia , lookup
Electrocardiography wikipedia , lookup
History of invasive and interventional cardiology wikipedia , lookup
Heart failure wikipedia , lookup
Cardiac contractility modulation wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
Myocardial infarction wikipedia , lookup
Cardiac surgery wikipedia , lookup
Coronary artery disease wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
Dextro-Transposition of the great arteries wikipedia , lookup
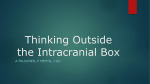
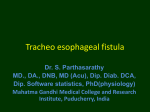
56 © JAPI • february 2013 • VOL. 61 Case Report Subclavian Artery- Internal Jugular Vein Fistula and Heart Failure: Complication of Internal Jugular Vein Catheterization Jai Prakash1, Brojen Takhellambam2, Biplab Ghosh2, Tauhidul Alam Choudhury2, Shivendra Singh3, Om Prakash Sharma4 Abstract Hemodialysis in patients with end-stage renal disease (ESRD) requires vascular access which can be either temporary or permanent. However, these procedures are not without complications. Arterial puncture is the most common immediate complication and pseudoaneurysm formation is the most common late sequel of internal jugular venous catheterization (IJVC). However, arterio-venous fistula (AVF) formation following IJVC is rare. We are reporting a case of AVF formation between subclavian artery (SCA) and internal jugular vein (IJV) following IJVC which later on leads to the development of cardiac failure. I Introduction n patients with end-stage renal disease (ESRD), cannulation of the central venous system with large-bore double lumen catheter is used for hemodialysis until a functioning permanent vascular access is available. Internal jugular venous catheterization (IJVC) is the most preferred route as subclavian approach is frequently associated with stenosis.1 However, serious adverse events such as arterial injury, pneumothorax and nerve injury can occur with these procedures.2-4 Arterial puncture, especially of the carotid artery is the most common complication of IJVC.4 Rarely subclavian artery injuries can also occur.2,3 The most frequent sequelae of accidental puncture of an artery is pseudoaneurysm formation.5 However, subclavian artery (SCA) to internal jugular venous (IJV) fistula after IJVC is extremely rare. We are reporting a rare case of SCA to IJV-fistula formation after IJVC which lead to the development of congestive cardiac failure (CCF). Case Report A 45-years-old non-diabetic lady having chronic kidney disease (CKD) for the last three years progressed to ESRD and became dialysis dependent. The baseline physical examination and investigations revealed anemia, hypertension, stage I left ventricular diastolic dysfunction, mild mitral regurgitation (MR) and good systolic function with left ventricular ejection fraction (LVEF) of 63.82% without any regional wall motion abnormalities. She received renal replacement therapy (RRT) initially in the form of acute peritoneal dialysis and later on maintenance hemodialysis with femoral vein catheterization as the vascular access since November 2009. A radio–cephalic arterio-venous fistula (AVF) was constructed and IJVC was planned to be used till the fistula becomes mature. On 21st January 2010 right IJVC was attempted using the blind landmark-guided technique with 18 G introducer needle which resulted in an accidental arterial puncture. The needle was removed and firm pressure was applied for about 15 minutes till a good hemostasis was achieved. A pressure dressing was Professor, 2Senior Resident, 3Assistant Professor, Department of Nephrology, 4Professor, Department of Radio Diagnosis, Institute of Medical Sciences, Banaras Hindu University, Vanarasi, Uttar Pradesh Received: 28.03.2011; Accepted: 01.04.2011 1 142 applied and patient was sent home. A double-lumen 11.5 Fr Quinton intrajugular catheter was inserted next day successfully by the same technique without any problem. At the end of the process vitals were stable and chest x-ray confirmed the position of the catheter tip at the junction of superior vena cava and right atrium. Patient was put on thrice weekly hemodialysis schedule since then. However because of exit site infection catheter was removed on 26th February 2010. Unfortunately the radio–cephalic fistula did not become functional and a brachio-cephalic fistula was constructed subsequently. Repeated femoral vein was used as access for hemodialysis for the next one and half months as patient did not give consent for other mode of access. After, 45 days of removal of IJVC, patient presented in the hospital emergency with breathlessness and swelling of body. On physical examination she had features of CCF and a continuous murmur was audible in the right supra-clavicular fossa. An emergency echocardiography showed global hypokinesia with LVEF of 33%, stage III diastolic dysfunction, severe mitral regurgitation (MR), moderate pulmonary regurgitation, and moderate tricuspid regurgitation with mild aortic regurgitation without any regional wall movement abnormality. Color Doppler study of neck vessels showed a fistulous communication between right SCA and IJV with a high blood velocity of 481cm /s (Figures 1 and 2). CT angiography of neck vessels confirmed the finding of AVF showing a vascular channel of maximum lumen diameter of 4.6mm and approximate length of 3 cm arising from the right SCA, coursing anteriorly and superiorly and communicating with right IJV about 19.3mm cranial to its termination to brachiocephalic vein (Figure 3). She improved with medical management of CCF and MHD was continued with repeated femoral vein puncture as vascular access as the brachio-cephalic fistula also did not become functional. After 2 months she agreed to switch over to CAPD because no vascular access was available for continuing maintenance hemodialysis. Discussion Anatomical variations of the internal jugular vein which occurs in about 5% of patients, makes it difficult to locate the vein using the blind technique. In the vast majority of cases, IJVC is successful and uncomplicated, but sometimes inadvertent arterial injury can result in the development of hematoma, pseudoaneurysm or AVF.2,3 The most common arterial injury associated with IJVC is carotid artery puncture and its incidence © JAPI • february 2013 • VOL. 61 © JAPI • february 2013 • VOL. 61 57 Fig. 1 : Color Doppler study of right neck vessels showing high velocity blood flow (481cm/s) at the level of fistula strongly suggestive of arterio-venous fistula Fig. 3 : CT angiography showing communication (arrow) between costo-cervical trunk of subclavian artery and internal jugular vein at the level of lower neck on right side correlation between the increase in atrial natriuretic peptide level and the elevation in CO as well as a direct positive correlation between the increase in brain natriuretic peptide level and the subsequent development of diastolic dysfunction.13 Previously it was thought that high-output failure was relevant only with longstanding fistulae but recently it was found that AVFs can reach their maximum flow as early as 6 weeks after creation and, thus, perhaps high-output cardiac failure can occur sooner than initially thought.14 This may explain the deteriorating cardiac status (from stage I diastolic dysfunction to stage III, severe MR and global hypokinesia, LVEF-33.69%) two and half months after the cannulation in our patient. To the best of our knowledge this is probably the first case of heart failure which developed due to fistula formation between SCA and IJV following IJVC in a patient of ESRD. Fig. 2 : Color Doppler study of right neck vessels revealed mosaic appearance at the site of arterio-venous communication between the subclavian artery and internal jugular vein. is as high as 11%, which frequently leads to pseudoaneurysms (0.05–2%) formation.3,5 The actual incidence and frequency of SCA injuries following IJVC are unknown because many cases are probably underreported. Three cases of AV fistula between SCA to IJV had been reported so far.6-8 In our case, we assume that the fistula formation was because of arterial puncture during the needle insertion. The arterial lesion could have been temporarily closed, but reopened days later by increasing hypertension, use of anticoagulant, abnormal calcium and phosphate metabolism which usually occurs in ESRD patients. In summary, one should be aware of development of arteriovenous fistula between SCA and IJV as a complication of IJVC which can lead to CCF later on. AVF bypasses a good proportion of left ventricular (LV) output from systemic circulation to right atrium and thus increases preload of the right ventricle and LV in turn. Subsequently the left ventricle dilates and LVEF declines causing heart failure.9 Savage at el reported that a decrease in the subendocardial perfusion occurred immediately after AVF creation in ESRD patients leading to the development of cardiac failure in some patients.10 Location of the AVF also predicts its outcome, as fistulae located centrally near the heart as in our patient, are more likely to produce heart failure.11 Most dialysis patients can tolerate the increased hemodynamic disturbances imposed by a fistula. However, individuals with pre- existing cardiac disease as in our patient are more susceptible to develop high-output cardiac failure.12 CCF with a low EF can be present despite a concomitant high-output state if the high-output states superimpose on the underlying cardiomyopathy. Because LVEF is a proportion of cardiac output (CO) and preload, increase in preload in excess of increase in CO will yield a low LVEF and CCF will develop as in our case. Iwashima et al observed that most of the increase in CO and left ventricular end-diastolic diameter occurred within the 7 to 10 days of AVF creation for hemodialysis.13 There was a positive © JAPI • february 2013 • VOL. 61 References 1. Michael A, Work J. Venous catheter access for haemodialysis. In: Daugirdas J T, Blake P G. Todds,eds. Handbook of dialysis. Lippincott Williams and Wilkins. Philadelphia 2007; 87-104. 2. Huddy SPJ, Mc Ewan A, Sabbat J, et al. Giant false aneurysm of the subclavian artery: an unusual complication of internal jugular venous cannulation. Anaesthesia 1989;44:588–589. 3. Powell H, Beechey PG. Internal jugular catheterisation: case report of a potentially fatal hazard. Anaesthesia 1990;45:458–459. 4. Peres PW. Positioning central venous catheters. A prospective survey. Anaesth Intensive Care 1990;18:536–539. 5. Trubel W, Staudacher M. The false aneurysm after iatrogenic arterial puncture: incidence, risk factors, and surgical treatment. Int J Angiol 1994;3:207–211. 6. Merino-Angulo J, Cortazar J, Saez-Garmendia F. Subclavian artery to internal jugular vein fistula following percutaneous internal jugular vein catheterization. Cathet Cardiovasc Diagn 1984;10:593– 595. 7.Finlay DJ, Sanchez LA, Sicard GA. Subclavian artery injury, vertebral artery dissection, and arteriovenous fistulae following 143 58 © JAPI • february 2013 • VOL. 61 attempt at central line placement. Ann Vasc Surg 2002;16:774–778. 8. dos Santos MLT, Demartini Jr Z, Matos LAD, et al. Radiculopathy due to iatrogenic fistula between subclavian artery and internal jugular vein. Clinical Neurology and Neurosurgery 2008;110:80–82. 9. Jennifer M, MacRae, Sanjay Pandeya et al. Arteriovenous Fistula– Associated High-Output Cardiac Failure: A Review of Mechanisms. Am J Kidney Dis 2004;43:e17-e21. 10. Savage MT, Ferro CJ, Sassano A, Tomson CR. The impact of arteriovenous fistula formation on central hemodynamic pressures in chronic renal failure patients: A prospective study. Am J Kidney Dis 2002;40:753-759. 11. Givertz MM, Colucci WS, Braunwald E. Clinical aspects of heart 144 failure: high-output failure, pulmonary edema. In: Braunwald E, Zipes DP, Libby P, eds. Heart Disease: A Textbook of Cardiovascular Medicine. 6th ed. WB Saunders, Philadelphia: 2001;534-561. 12. Anderson CB, Codd JR, Graff RA, et al. Cardiac failure and upper extremity arterio-venous dialysis fistulas. Case reports and a review of the literature. Arch Intern Med 1976;136:292-297. 13. Iwashima Y, Horio T, Takami Y et al. Effects of the creation of arteriovenous fistula for hemodialysis on cardiac function and natriuretic peptide levels in CRF. Am J Kidney Dis 2002;40:974-982. 14.Begin V, Ethier J, Dumont M, et al. Prospective evaluation of the intra access flow of recently created native arteriovenous fistulae. Am J Kidney Dis 2002;40:1277-128. © JAPI • february 2013 • VOL. 61