Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
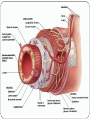
Digestive System Dr. Michael P. Gillespie Digestion & Absorption Digestion is the process of breaking down food into molecules that are small enough to enter the body cells. Absorption is the passage of these smaller molecules through the plasma membrane of cells lining the stomach and intestines into the blood and lymph. Digestive System The organs that perform the functions of digestion and absorption are collectively referred to as the digestive system. Gastroenterology deals with the structure, function, diagnosis and treatment of diseases of the stomach and intestines. Proctology deals with the diagnosis and treatment of disorders of the rectum and anus. Components Of The Digestive System The gastrointestinal (GI) tract or alimentary canal is a continuous tube that extends from the mouth to the anus through the ventral body cavity. Organs of the GI tract include the mouth, most of the pharynx, esophagus, stomach, small intestine, and large intestine. The length of the GI tract in a cadaver is about 9m (30 ft). It is shorter in a living person due to clonus. Components Of The Digestive System Accessory digestive organs include the teeth, tongue, salivary glands, liver, gallbladder, and pancreas. The teeth aid in the physical breakdown of food and the tongue assists in chewing and swallowing. The other accessory digestive organs never come into direct contact with the food. They produce or store secretions that flow into the GI tract and aid in the chemical breakdown of food. Functions Of The Digestive System Ingestion Secretion Mixing and propulsion Digestion Absorption Defecation Ingestion This process involves taking foods and liquids into the mouth (eating). Secretion Cells within the walls of the GI tract secrete about 7 liters of water, acid, buffers, and enzymes into the lumen of the GI tract daily. Mixing & Propulsion Alternating contraction and relaxation of smooth muscle in the walls of the GI tract mix food and secretions and propel them toward the anus. This is referred to as motility. Digestion Mechanical digestion. The teeth cut and grind food. The smooth muscles of the stomach and small intestine churn the food to help it dissolve and mix with enzymes. Digestion Chemical digestion. The large carbohydrate, lipid, protein, and nucleic acid molecules in food are split into smaller molecules by hydrolysis. Digestive enzymes produced by the salivary glands, tongue, stomach, pancreas, and small intestines catalyze these catabolic reactions. Amino acids, cholesterol, glucose, vitamins, minerals, and water can be absorbed without chemical digestion. Absorption Absorption is the entrance of ingested and secreted fluids, ions, and small molecules that are products of digestion into the epithelial cells lining the lumen of the GI tract. The absorbed substances pass into the blood or lymph and circulate to all cells of the body. Defecation Substances that were not absorbed leave the body through the anus in a process called defecation. These substances include wastes, indigestible substances, bacteria, cells sloughed from the GI tract, and digested materials that were not absorbed. The eliminated material is called feces. Layers Of The GI Tract Mucosa Submucosa Muscularis Serosa Mucosa The mucosa (inner lining) is a mucous membrane. It is composed of a layer of epithelium in direct contact with the contents of the GI tract, areolar connective tissue, and a thin layer of smooth muscle (muscularis mucosae). Mucosa Epithelium. Epithelium in the mouth, phaynx, esophagus, and anal canal is nonkeratinized stratified squamous epithelium and serves a protective function. Epithelium in the stomach and intestines is simple columnar epithelium and functions in secretion and absorption. Mucosa Lamina propria. Areolar connective tissue containing many blood and lymphatic vessels, which are routes through which nutrients are absorbed. Mucosa-associated lymphatic tissue is also present to protect against microbes. Muscularis mucosa. A thin layer of smooth muscle fibers which creates folds in the stomach and small intestine to increase surface area. Submucosa The submucosa consists of areolar connective tissue that binds the mucosa to the muscularis. Submucosa It contains blood and lymphatic vessels that receive absorbed food molecules. Submucosa It also contains the submucosal plexus (plexus of Meissner) which is an extensive network of neurons. These neurons are part of the enteric nervous system or “brain of the gut”. They regulate movements of the mucosa and vasoconstriction of the blood vessels. The nerves innervate secretory cells of the mucosal and submucosal glands. Muscularis The muscularis of the mouth, pharynx, and superior and middle parts of the esophagus contains skeletal muscle that produces voluntary swallowing. Skeletal muscle also forms the external anal sphincter, which permits voluntary control of defecation. Muscularis The rest of the GI tract muscularis contains smooth muscle. The myenteric plexus (plexus of Auerbach) is within the layers of smooth muscle. It is also part of the enteric nervous system and controls GI motility (i.E. GI frequency and strength of contraction). Serosa The serosa is the superficial layer of the portions of the GI tract that are suspended in the abdominopelvic cavity. Inferior to the diaphragm it is called the visceral peritoneum. Peritoneum The peritoneum is divided into parietal peritoneum which lines the wall of the abdominopelvic cavity and visceral peritoneum which lines some of the organs in the cavity. The space between the parietal and visceral peritoneum is called the peritoneal cavity. In some diseases, the peritoneal cavity becomes distended by the accumulation of fluid in a condition called ascites. Retroperitoneal Some organs lie on the posterior abdominal wall and are only covered by peritoneum on their anterior surface. These organs are said to be retroperitoneal and include the kidneys and pancreas. Peritoneum Functions The peritoneum contains large folds that weave between the viscera. These folds bind the organs to each other and to the walls of the abdominal cavity. They also contain blood vessels, lymphatic vessels, and nerves that supply the abdominal organs. Peritoneal Folds Greater omentum. Falciform ligament. Lesser omentum. Mesentery. Mesocolon. Greater Omentum The largest peritoneal fold. It drapes over the transverse colon and coils of the small intestine like a “fatty apron”. It contains a considerable amount of fatty tissue. It can greatly expand with weight gain, giving rise to the characteristic “beer belly”. There are many lymph nodes in the greater momentum. Falciform Ligament The falciform ligament attaches the liver to the anterior abdominal wall and diaphragm. The liver is the only digestive organ that is attached to the anterior abdominal wall. Lesser Omentum The lesser omentum suspends the stomach and duodenum from the liver. It contains some lymph nodes. Mesentery The mesentery is fan-shaped and binds the small intestine to the posterior abdominal wall. Blood vessels, lymphatic vessels, and lymph nodes lie between the two layers of mesentery. Mesocolon The mesocolon binds the large intestine to the posterior abdominal wall. It carries blood vessels and lymphatic vessels. The mesentary and mesocolon work together to loosely hold the intestines in place. This allows for great movement to allow them to mix food and propel food along the GI tract. Peritonitis Peritonitis is an acute inflammation of the peritoneum. Contamination of the peritoneum by infectious microbes causes it. Peritonitis This is the result of accidental or surgical wounds in the abdominal wall. Perforation or rupture of abdominal organs also causes this. When inflamed peritoneal surfaces rub together, peritonitis can result. Mouth The mouth is also referred to as the oral or buccal cavity. It is formed by the cheeks, hard and soft palates, and tongue. Mouth The lips (labia) are fleshy folds surrounding the opening of the mouth. The labial frenulum is a midline fold of mucous membrane that attaches the inner surface of each lip to its corresponding gum. The orbicularis oris and buccinator muscles keep food between the upper and lower teeth to assist in chewing. Mouth The vestibule of the oral cavity is the space bounded by the cheeks and lips externally and the teeth and gums internally. The oral cavity proper is the space that extends between the teeth and gums to the fauces (opening between the oral cavity and throat). Mouth The hard palate is the anterior portion of the roof of the mouth and is formed by the maxillae and palatine bones. Mouth The soft palate is the posterior portion of the roof of the mouth. It is an arch-shaped muscular partition that is lined by mucous membrane. The uvula is a conical muscular process hanging from the free border of the soft palate. During swallowing, the uvula and soft palate are drawn superiorly and closing off the nasopharynx to prevent foods from entering the nasal cavity. Salivary Glands A salivary gland is any cell or organ that releases saliva into the oral cavity. Saliva cleanses the mouth and teeth. When food enters the mouth, secretion of saliva increases. Saliva lubricates, dissolves, and begins the chemical breakdown of food. Minor Salivary Glands Labial glands in the lips. Buccal glands in the cheeks. Palatal glands in the palate. Lingual glands in the tongue. Major Salivary Glands These glands lie beyond the oral mucosa and empty their secretions into ducts that lead to the oral cavity. Parotid glands and parotid duct. Submandibular glands and submandibular ducts. Sublingual glands and lesser sublingual ducts. Composition & Functions Of Saliva Saliva is 95/5% water and 0.5% solutes. Lysozyme – a bacteriolytic enzyme. Salivary amylase – a digestive enzyme that acts on starch. Salivation Salivation is the secretion of saliva. It is controlled by the autonomic nervous system. The feel and taste of food are potent stimulators of salivary gland secretions. Salivation Chemicals in food stimulate taste receptors on the tongue and impulses are propagated to the salivary nuclei in the brain stem. Impulses from the facial nerve (CN VII) and the glossopharyngeal nerve (CN IX) stimulate the secretion of saliva. Saliva continues to be secreted heavily for some time after food is swallowing. This washes out the mouth. Mumps Mumps is an inflammation and enlargement of the parotid glands accompanied by moderate fever, malaise (general discomfort), and extreme pain in the throat, especially when swallowing sour foods or acidic juices. Swelling also occurs on one or both sides of the face. In about 30% of males past puberty, the testes may also become inflamed (orchitis). Tongue The tongue is an accessory digestive organ composed of skeletal muscle covered with a mucous membrane. Extrinsic muscles of the tongue move the tongue from side to side and in and out to maneuver food for chewing and push food to the back of the mouth. The intrinsic muscles of the tongue alter the shape and size of the tongue for speech and swallowing. Tongue The lingual frenulum is a fold of mucous membrane in the midline of the undersurface of the tongue. It limits movement of the tongue posteriorly. Ankyloglossia is a condition in which the lingual frenulum is abnormally short impairing eating and speaking (“tonguetied”). Tongue Papillae cover the dorsum and lateral surfaces of the tongue. Fungiform papillae – mushroom like elevations near the tip of the tongue that contain taste buds. Vallate (circumvallate) papillae – contain taste buds and are located in a V shape on the posterior surface. Foliate papillae – located in small trenches on the lateral margins of the tongue. Most of the taste buds degenerate during childhood. Filiform papillae – distributed in parallel rows. They lack taste buds, but contain receptors for touch. Tongue Lingual glands secrete both mucus and a watery serous fluid that contain the enzyme lingual lipase. Teeth Teeth or dentes are accessory digestive organs located in the sockets of the alveolar processes. The processes are covered by gingivae (gums). The sockets are lined by the periodontal ligament or membrane. The teeth are composed primarily of dentin, a calcified connective tissue. Teeth Teeth are harder than bone because of the higher content of calcium salts. The dentin encloses a pulp cavity. The pulp is a connective tissue containing blood vessels, nerves, and lymphatic vessels. Teeth Root canals are narrow extensions of the pulp cavity. A hard substance called enamel covers the dentin of the crown. Enamel is the hardest substance in the body. Branches Of Dentistry Endodontics – deals with prevention, diagnosis, and treatment of diseases that affect the pulp, root, periodontal ligament, and alveolar bone. Orthodontics – deals with prevention and correction of abnormally aligned teeth. Periodontics – deals with treatment of abnormal conditions of the tissues immediately surrounding the teeth. Dentitions Humans have two dentitions (sets of teeth). Deciduous teeth. Permanent teeth. Dentitions Deciduous teeth – also called primary teeth, milk teeth, or baby teeth. Begin to erupt at about 6 months or age and one pair of teeth appears at about each month thereafter until all 20 are present. Permanent teeth – also called secondary teeth. The deciduous teeth are lost between the ages of 6 and 12 years and replaced by permanent teeth. The permanent dentition contains 32 teeth that erupt between age 6 and adulthood. Types Of Teeth Incisors – chisel-shaped to cut into food. Cuspids (canines) – have a pointed surface called a cusp. They are used to tear or shred food. Molars – crush and grind food. Root Canal Therapy All traces of pulp tissue are removed from the pulp cavity and root canals of a badly diseased tooth. A hole is made in the tooth and the root canals are filed out and irrigated to remove bacteria. The canals are treated with medication and sealed tightly. The damaged crown is then repaired. Mechanical & Chemical Digestion In The Mouth Mechanical digestion results from mastication (chewing) in which the food is manipulated by the tongue, ground by the teeth, and mixed with saliva. Mechanical & Chemical Digestion In The Mouth The food becomes a soft, flexible mass called a bolus (lump) that is easily swallowed. Mechanical & Chemical Digestion In The Mouth Chemical digestion is assisted by two enzymes in the mouth. Salivary amylase initiates the breakdown of starch. It reduces the long-chain polysaccharides to disaccharides and trisaccharides. It is deactivated by the stomach acid in about an hour. Lingual lipase is secreted by glands in the tongue and begins to work in the acidic environment of the stomach. It breaks down triglycerides into fatty acids and diglycerides. Summary Of Digestive Activities Of The Mouth Cheeks and lips – keep food between teeth. Food is uniformly chewed during mastication. Salivary glands – secrete saliva which softens, moistens, and dissolves food. Saliva cleanses the mouth and teeth. Salivary amylase splits starch into smaller fragments. Summary Of Digestive Activities Of The Mouth Tongue – maneuvers food for mastication and swallowing. Receptors for gustation (taste) which stimulates salivary glands. Secretes lingual lipase which breaks down triglycerides. Teeth – cut, tear, and pulverize food to create smaller particles for swallowing and increase surface area for enzymatic reactions to occur. Pharynx When food is first swallowed, it passes from the mouth into the pharynx. The pharynx is composed of skeletal muscle tissue lined by a mucous membrane. Pharynx The nasopharynx functions only in respiration; However, the oropharynx and laryngopharynx function in both respiration and digestion. Pharynx Swallowing (deglutition) moves food from the mouth to the stomach. Voluntary stage – the bolus is passed into the oropharynx. Pharyngeal stage – involuntary passage of the bolus through the pharynx into the esophagus. Esophageal stage – involuntary passage of the bolus from the esophagus to the stomach. The bolus stimulates receptors in the oropharynx, which sends signals to the deglutition center in the medulla oblongata and lower pons of the brain stem. Esophagus The esophagus is a collapsible muscular tube that lies superior to the trachea. It lies posterior to the trachea and is about 25 cm (10 in.) Long. Esophagus It pierces the diaphragm at an opening called the esophageal hiatus and ends in the superior portion of the stomach. Sometimes part of the stomach protrudes above the diaphragm through the esophageal hiatus (hiatal hernia). Physiology Of The Esophagus The esophagus secretes mucus and transports food into the stomach. The esophagus does NOT secrete digestive enzymes and does NOT participate in absorption. Physiology Of The Esophagus The upper esophageal sphincter regulates the entrance of food into the esophagus from the laryngopharynx. Physiology Of The Esophagus During the esophageal stage of swallowing, peristalsis occurs. Peristalsis is a progression of coordinated contractions and relaxations and pushed the food bolus onward. The lower esophageal sphincter relaxes during swallowing and allows the bolus to pass through to the stomach. Gastroesophageal Reflux Disease If the lower esophageal sphincter fails to close adequately after food has entered the stomach, the stomach contents can reflux, or back up, into the inferior portion of the esophagus. This is known as gastroesophageal reflux disease (GERD). Gastroesophageal Reflux Disease Hydrochloric acid (HCl) from the stomach contents can irritate the esophageal wall, resulting in a burning sensation called heartburn. Drinking alcohol and smoking can cause the sphincter to relax, worsening the problem. GERD may be associated with cancer of the esophagus. Stomach The stomach is a j-shaped enlargement of the GI tract. It lies inferior to the diaphragm in the epigastric, umbilical, and left hypochondriac regions of the abdomen. Stomach The stomach connects the esophagus to the duodenum. A meal can be eaten much faster than the intestines can digest and absorb it. The stomach is the most distensible part of the GI tract. Functions Of The Stomach Reservoir for holding food before release to SI. Mixes the saliva, food and gastric juice to form chyme. The semisolid bolus of food is converted into a liquid. Secretes gastric juice, which contains HCL, pepsin, intrinsic factor, and gastric lipase. Digestion of starch continues. Functions Of The Stomach HCL kills bacteria and denatures proteins. Pepsin begins digestion of proteins. Intrinsic factor aids absorption of vitamin B12. Gastric lipase aids in digestion of triglycerides. Secretes gastrin into blood. Certain substances are absorbed. Anatomy Of The Stomach Four main regions: Cardia – surrounds the superior opening of the stomach. Fundus – the rounded portion superior and to the left of the cardia. Body – the large central portion of the stomach inferior to the fundus. Pylorus – the region of the stomach that connects to the duodenum. Pylorus Pyloric antrum – connects to the body of the stomach. Pyloric canal – leads to the duodenum. Pyloric sphincter – connects the stomach to the duodenum and regulates passage of food. Anatomy Of The Stomach Rugae – large folds in the mucosa of the stomach when it is empty. Lesser curvature – the concave medial border of the stomach. Greater curvature – the convex lateral border of the stomach. Abnormalities Of The Pyloric Sphincter In Infants Pylorospasm – the muscle fibers of the sphincter fail to relax normally and fails to allow passage of food. The stomach becomes overly full and the infant vomits. Drugs to relax the muscles are used. Pyloric Stenosis – narrowing of the pyloric sphincter. This must be corrected surgically. Projectile vomiting is the hallmark symptom of this condition. Histology Of The Stomach The stomach wall is composed of the same four basic layers of the rest of the GI tract with minor modifications. Histology Of The Stomach The surface of the mucosa contains simple columnar epithelial cells called surface mucous cells. Epithelial cells extend into the lamina propria, where they form columns of secretory cells called gastric glands that line chambers called gastric pits. Gastric Glands The gastric glands contain 3 types of exocrine gland cells that secrete their products into the lumen of the stomach. Mucous neck cells – secrete mucous. Parietal cells – produce intrinsic factor. Chief cells – secrete pepsinogen and gastric lipase. These secretions are called gastric juice (approximately 2000 – 300 ml per day). Mechanical Digestion In The Stomach Mixing waves occur several minutes after food enters the stomach – these are gentle, rippling, peristaltic movements. They occur every 15 to 25 seconds. Few mixing waves occur in the fundus. It serves primarily a storage function. Mechanical Digestion In The Stomach These waves macerate food, mix it with the secretions of the gastric glands, and reduce it to a soupy liquid called chyme. The pylorus remains almost, but not completely closed. Each mixing wave forces some food through the pyloric sphincter. Chemical Digestion In The Stomach Foods may remain in the fundus for up to an hour without becoming mixed with gastric juice. During this time, digestion by salivary amylase continues. Once the food becomes mixed with gastric juice, the salivary amylase is inactivated and the lingual lipase is activated. The parietal cells secrete HCl. Chemical Digestion In The Stomach The chief cells secrete pepsin, which is a proteolytic enzyme. Pepsin is activate in the acidic environment of the stomach. Pepsin is secreted in an inactive form called pepsinogen and therefore does not digest the proteins of the chief cells that secrete it. Chemical Digestion In The Stomach Pepsinogen does not become activate until it comes into contact with active pepsin molecules or HCl. The stomach epithelial cells are protected by mucous secreted from the mucous neck cells. Gastric lipase begins breakdown of triglycerides; However, it does not work well in the acidic environment. Gastric Emptying Gastric emptying is the periodic release of chyme from the stomach into the duodenum. Stimuli such as distention of the stomach and the presence of partially digested proteins, alcohol, and caffeine initiate gastric emptying. Gastric Emptying The enterogastric reflex ensures that the stomach does not release more chyme than the small intestine can handle. Stimuli such as distention of the duodenum and the presence of fatty acids, glucose, and partially digested proteins in the duodenal chyme inhibit gastric emptying. Gastric Emptying Within 2 – 4 hours after eating a meal, the stomach has emptied its contents into the duodenum. Foods rich in carbohydrates spend the least time in the stomach, proteins longer, and fat-laden meals the longest. Vomiting Vomiting or emesis is the forcible expulsion of the contents of the upper GI tract (stomach and sometimes duodenum) through the mouth. Stimuli include the following: Irritation and distention of the stomach. Unpleasant sights. General anesthesia. Dizziness. Certain drugs (morphine, derivatives of digitalis). Vomiting Vomiting involves squeezing the stomach between the diaphragm and abdominal muscles and expelling the contents through open esophageal sphincters. Prolonged vomiting can lead to alkalosis (higher than normal blood pH). Pancreas Stomach chyme passes into the duodenum for chemical digestion. Activities of the pancreas, liver, and gallbladder are necessary for this chemical digestion to occur. Anatomy Of The Pancreas The pancreas is a retroperitoneal gland. It is about 12-15 cm long and 2.5 cm thick. It lies posterior to the greater curvature of the stomach. Anatomy Of The Pancreas The pancreas consists of a head, body and tail. It is connected to the duodenum by 2 ducts. Pancreatic duct (duct of Wirsung) – larger. In most people, the pancreatic duct joins the common bile duct from the liver and gallbladder and enters the duodenum as the hepatopancreatic ampulla (ampulla of Vater). The ampulla opens at the major duodenal papilla. Accessory duct (duct of Santorini) – smaller. Histology Of The Pancreas 99% of the pancreas is made up of small clusters of glandular epithelial cells called acini, which make up the exocrine portion of the gland. The acini secrete the pancreatic juice, which is a mixture of fluid and digestive enzymes. Histology Of The Pancreas The remaining 1% of the pancreas consists of the pancreatic islets (islets of Langerhans), which make up the endocrine portion of the pancreas. The islets secrete the hormones glucagon, insulin, somatostatin, and pancreatic polypeptide. Pancreatic Juice: Composition & Function The pancreatic juice is a clear, colorless liquid consisting mostly of water, some salts, sodium bicarbonate, and several enzymes. Pancreatic Juice: Composition & Function Sodium bicarbonate buffers acidic juice in chyme, stops the action of stomach pepsin, and creates the proper pH for digestive enzymes of the small intestine. Pancreatic Juice: Composition & Function Enzymes include: Pancreatic amylase. Protein digesting enzymes. Trypsin. Chymotrypsin. Carboxypeptidase. Elastase. Pancreatic lipase. Nucleic acid digesting enzymes. Ribonuclease. Deoxyribonuclease. Pancreatitis Pancreatitis is inflammation of the pancreas. It can occur with alcohol abuse or with chronic gallstones. Acute pancreatitis is a more severe condition associated with heavy alcohol intake or biliary tract obstruction. Trypsin begins to digest the pancreatic cells. Recurrent attacks are common. Liver The liver is the heaviest gland of the body, weighing about 1.4 kg. It is the 2nd largest organ in the body after the skin. It is inferior to the diaphragm and occupies most of the right hypochondriac region and part of the epigastric region. Gallbladder The gallbladder is a pear-shaped sac that is located in a depression of the posterior surface of the liver. It is about 7-10 cm long and typically hangs from the anterior inferior margin of the liver. Anatomy Of The Liver The liver is divided into a large right lobe and a smaller left lobe by the falciform ligament. The falciform ligament also suspends the liver. The liver is almost completely covered by visceral peritoneum. Anatomy Of The Gallbladder The parts of the gallbladder are the broad fundus, the body (central portion), and the neck (tapered portion). Functions Of Gallbladder The gallbladder stores and concentrates bile until it is needed in the small intestine. In the concentration process, water and ions are absorbed by the gallbladder mucosa. Histology Of The Liver & Gallbladder The lobes of the liver are made up of many functional units called lobules. The lobules contain hepatocytes arranged in irregular, branching, interconnected plates around a central vein. Histology Of The Liver & Gallbladder The liver has large endothelial lined spaces called sinusoids instead of capillaries. Fixed phagocytes called stellate reticuloendothelial (Kuppfer) cells destroy worn out WBCs, RBCs, bacteria, and any other foreign material in venous blood draining from the GI tract. Histology Of The Liver & Gallbladder Bile is secreted from the hepatocytes and travels through the right and left hepatic ducts. These ducts merge to form the common hepatic duct, which later joins the cystic duct from the gallbladder. Bile is stored in the gallbladder for later release. Jaundice Jaundice is a yellowish coloration of the sclera, skin, and mucous membranes due to buildup of a yellow compound called bilirubin. As RBCs break down they release bilirubin. Jaundice Bilirubin is processed by the liver and excreted into bile. 3 categories of jaundice: Prehepatic jaundice – excess production of bilirubin. Hepatic jaundice – congenital liver disease, cirrhosis of the liver, or hepatitis. Extrahepatic jaundice – blockage of bile drainage by gallstones, cancer of the bowel or pancreas. Bile Bile is a yellow, brownish, or olive-green liquid. Bile salts play a role in emulsification, the breakdown of large lipid globules into a suspension of droplets. This also aids in the absorption of lipids following digestion. These droplets increase the surface area allowing pancreatic lipase to function more efficiently. Functions Of The Liver Carbohydrate metabolism. Lipid metabolism. Protein metabolism. Processing of drugs and hormones. Functions Of The Liver Excretion of bilirubin. Synthesis of bile salts. Storage. Phagocytosis. Activation of vitamin D. Gallstones If bile contains insufficient bile salts, insufficient lecithin, or excessive cholesterol, the cholesterol may crystallize to form gallstones. As the gallstones grow in size or number, they may cause minimal, intermittent, or complete obstruction to the flow of bile from the gallbladder to the duodenum. Gallstones Treatment consists of using gallstone-dissolving drugs, lithotripsy (shock-wave therapy), or surgery. Recurrent gallstones, failure of drugs, or contraindication to lithotripsy may warrant cholecystectomy (removal of the gallbladder). Digestive Hormones Gastrin promotes secretion of gastric juice, increases gastric motility, and promotes growth of the gastric mucosa. Secretin stimulates the secretion of pancreatic juice and bile. Inhibits secretion of gastric juice. Cholecystokinin stimulates secretion of pancreatic juice and causes ejection of bile from the gallbladder. Enhances the effects of secretin. Small Intestine (SI) The major events of digestion and absorption occur in the small intestine. The length of the SI provides great surface area for this to occur. Circular folds, villi, and microvilli also serve to increase the surface area of the SI. The SI begins at the pyloric sphincter of the stomach, coils through the central and inferior parts of the abdomen, and eventually opens into the LI. Functions Of The SI Segmentations mix chyme with digestive juices and bring food into contact with the mucosa for absorption. Peristalsis propels food through the SI. Functions Of The SI Completes the digestion of carbohydrates, proteins, and lipids. Begins and completes the digestion of nucleic acids. Absorption of 90% of nutrients and water. Anatomy Of The SI The SI is divided into 3 regions: Duodenum – shortest region, retroperitoneal, starts at the pyloric sphincter of the stomach. Jejunum – between the duodenum and ileum. Ileum – the longest region, joins the large intestine at the ileocecal sphincter. Anatomy Of The SI Circular folds – permanent ridges in the mucosa. They enhance absorption by increasing the surface area of the SI and by causes the chyme to spiral, rather than move in a straight line. Histology Of The SI The same 4 basic layers that make up the rest of the GI tract exist in the SI as well, with some basic exceptions. The mucosa forms a series of fingerlike villi (tufts of hair) projections, which increase the surface area available for absorption. Histology Of The SI Each villus contains an arteriole, a venule, a blood capillary network, and a lacteal through which nutrients are absorbed. Histology Of The SI The mucosa is simple columnar epithelium, which contains absorptive cells, goblet cells, enteroendocrine cells, and Paneth cells. The apical surface of the absorptive cells contains microvilli (bundles of actin filaments). Collectively, they are referred to as the brush border. They increase the surface area. Histology Of The SI The mucosa contains deep crevices lined with glandular epithelium. Cells lining the crevices form the intestinal glands (crypts of Lieberkuhn), which secrete intestinal juice. Histology Of The SI Paneth cells secrete lysozyme, a bactericidal enzyme. The lamina propria of the SI has an abundance of mucosa-associated lymphatic tissue (MALT). Solitary lymphatic nodules are present as well as groups of aggregated lymphatic nodules (Peyer’s patches). Duodenal (Brunner’s) glands of the submucosa secrete an alkaline mucus. Intestinal Juice Intestinal juice is a clear yellow fluid that contains water and mucus. It is slightly alkaline (pH 7.6). It provides a liquid medium to assist in the absorption of substances from chyme. Brush Border Enzymes The absorptive epithelial cells synthesize several digestive enzymes, called brush border enzymes, and insert them into the plasma membrane of the microvilli. Consequently, some digestion occurs at the surface of the epithelial cells and not exclusively in the lumen of the SI. Mechanical Digestion In The Small Intestine Segmentations – localized mixing contractions that occur in portions of the intestines distended by a large volume of chyme. Sloshes chyme back and forth. Migrating motility complexes – a type of peristalsis that moves the chyme down the length of the SI after segmentation has occurred. Chemical Digestion In The SI Chyme entering the small intestines contains partially digested carbohydrates, proteins, and lipids. Pancreatic juice, bile, and intestinal juice complete the effort of digestion. Digestion Of Carbohydrates Pancreatic amylase, sucrase, lactase, and maltase complete the digestion of carbohydrates. These enzymes break complex carbohydrates into monosaccharides, which can be absorbed. Lactose intolerance occurs in people whose mucosal cells fail to produce enough of the enzyme lactase. Symptoms include siarrhea, gas, bloating, and abdominal cramps after the consumption of dairy products. Digestion Of Proteins Pepsin, trypsin, chymotrypsin, carboxypeptidase, elastase, and peptidases complete the process of protein digestion. Proteins are broken down into single amino acids, which can be absorbed. Digestion Of Lipids Lipases complete the process of lipid digestion in the SI. Bile salts increase the surface area of triglycerides through the process of emulsification. The globules are converted into droplets. Lipids are broken down into monoglycerides, which can then be absorbed. Digestion Of Nucleic Acids Pancreatic juice contains two nucleases: ribonuclease (breaks down RNA) and deoxyribonuclease (breaks down DNA). Brush border enzymes further break these down into pentoses, phosphates, and nitrogenous bases, which can be absorbed. Absorption In The SI Forms that can be absorbed: Monosaccharides (glucose, fructose, and galactose) from carbohydrates. Single amino acids, dipeptides, and tripeptides from proteins. Fatty acids, glycerol, and monoglycerides from triglycerides. Absorption In The SI Mechanisms of absorption: Diffusion. Facilitated diffusion. Osmosis. Active transport. Absorption In The SI Passage of digested nutrients from the gastrointestinal tract into the blood or lymph is called absorption. About 90% of the nutrients are absorbed in the SI. The other 10% occurs in the stomach and the large intestine. Any undigested or unabsorbed material passes through to the LI. Absorption Of Monosaccharides All carbohydrates are absorbed as monosaccharides. They are absorbed via facilitated diffusion and active transport. The SI can absorb up to 120 grams of carbohydrates per hour. Absorption Of Amino Acids, Dipeptides, & Tripeptides Most proteins are absorbed as amino acids via active transport processes. About half of the amino acids come from food. The other half of the amino acids come from proteins in digestive juices and dead cells that slough off the mucosal surface. Absorption Of Lipids All dietary lipids are absorbed via simple diffusion. Adults absorb about 95% of the lipids present in the SI. Most dietary fatty acids require bile for adequate absorption. When lipids are not absorbed properly, the fat-soluble vitamins A, D, E, & K are not absorbed properly. Absorption Of Electrolytes Most of the electrolytes absorbed by the SI come from gastrointestinal secretions, and some come from ingested foods and liquids. Active transport mechanisms are utilized to absorb Na+ ions. Absorption Of Electrolytes Negatively charged bicarbonate, chloride, iodide, and nitrate ions can passively follow Na+ or be actively transported. Iron, potassium, magnesium, and phosphate ions are absorbed via active transport. Absorption Of Vitamins The fat-soluble vitamins A, D, E, & K are included with dietary lipids and absorbed via simple diffusion. Most water-soluble vitamins are absorbed via simple diffusion. Vitamin B12 combines with intrinsic factor and the combination is absorbed via active transport. Absorption Of Water The volume of water in the SI (about 9.3 liters daily) comes from ingested liquids and gastric secretions. The SI absorbs about 8.3 liters of it. 90% of the remaining water (about 0.9 liters) is absorbed in the large intestine. Water absorption occurs via osmosis. Absorption Of Alcohol Alcohol is lipid soluble and begins to be absorbed in the stomach. There is greater surface area for absorption in the SI; therefore, the longer alcohol remains in the stomach, the more slowly blood alcohol rises. Fatty acids in the chyme slow gastric emptying; therefore, eating fatty foods with alcohol will cause a slower rise in blood alcohol. Large Intestine (LI) The large intestine is the terminal portion of the GI tract. It is divided into four principal regions. Large Intestine Functions Completion of absorption (water, ions, and vitamins). Production of some B vitamins and vitamin K by bacteria in the LI. Formation of feces. Expulsion of feces (defecation) from the body through haustral churning and peristalsis. LI Anatomy The LI extends from the ileum to the anus. It is about 1.5 m long and 6.5 cm in diameter. It is attached to the posterior abdominal wall by mesocolon. Major Regions Of The LI Cecum. Colon. Rectum. Anal canal. LI Anatomy Continued… The iliocecal valve guards the opening to the LI from the ileum. The cecum hangs inferior to the iliocecal valve. The appendix is a twisted, coiled tube hanging on the cecum. The open end of the cecum merges with the colon, which is divided into ascending, transverse, descending, and sigmoid portions. LI Anatomy Continued… The last 20 cm of the GI tract make up the rectum. The anal canal is the termination of the rectum. The anus is the opening of the anal canal to the exterior. This opening is guarded by an internal anal sphincter (involuntary) and an external anal sphincter (voluntary). Appendicitis Inflammation of the appendix is termed appendicitis. Obstruction of the lumen of the appendix by chyme, inflammation, a foreign body, carcinoma, stenosis, or kinking of the organ precedes the appendicitis. It is characterized by high fever, elevated WBC count, and a neutrophil count higher than 75%. Subsequent infection can produce edema and ischemia. Perforation can occur within 24 hours. Appendicitis An appendicitis typically begins with referred pain to the umbilical region of the abdomen, followed by anorexia, nausea, and vomiting. After several hours, pain localizes in the right lower quadrant. Appendicitis The pain is continuous, dull or severe. Coughing, sneezing, or body movements can exacerbate the pain. Early appendectomy (removal of the appendix) is recommended, because it is safer to undergo surgery than to risk rupture and peritonitis. Histology Of The Large Intestine No villi or permanent circular folds are found in the mucosa of the large intestine. The epithelium contains mostly absorptive and goblet cells. The absorptive cells participate mainly in water absorption. Histology Of The Large Intestine The submucosa is similar to that found in the rest of the GI tract. The muscularis consists of an external layer of longitudinal smooth muscle and an internal layer of circular smooth muscle. This forms three conspicuous longitudinal bands called the teniae coli. Tonic contractions of the bands draw the LI together into pouches called haustra. Mechanical Digestion In LI The iliocecal sphincter regulates the passage of chyme from the ileum into the cecum. Normally, the valve remains partially closed to limit passage of chyme. After a meal, the gastroileal reflex intensifies ileal peristalsis. The hormone gastrin also relaxes the sphincter. Mechanical Digestion In LI Haustral churning – The haustra remain relaxed and become distended while they fill up. When the distention reaches a certain point, the walls contract and squeeze the contents into the next haustrum. Peristalsis occurs. Mass peristalsis is a movement that occurs at the middle of the transverse colon and quickly drives contents into the rectum. Food in the stomach initiates the gastrocolic reflex. Chemical Digestion LI Mucous is secreted by the glands of the LI, but no enzymes are secreted. The bacteria of the LI perform the final stages of digestion. Chemical Digestion LI Bacteria ferment any remaining carbohydrates, which releases hydrogen, carbon dioxide, and methane gases. These gases constitute the flatus (gas) in the colon. When the gas is excessive it is termed flatulence. Bacteria convert any remaining proteins into amino acids. Some B vitamins and vitamin K are produced by the bacteria in the colon. Absorption & Feces Formation In The LI Water is absorbed from the chyme over a period of 3-10 hours. As the water becomes absorbed it becomes solid or semi-solid and is termed feces. The feces consists of water, inorganic salts, sloughed off epithelial cells, bacteria, products of bacterial decomposition, unabsorbed digested materials, and indigestible parts of food. The LI absorbs water, vitamins and ions (I.e. sodium and chloride). Occult Blood Occult Blood refers to blood that is hidden and not detectable by the human eye. Urine and feces are often examined for occult blood. Occult blood testing is utilized to screen for colorectal cancer. Defecation Reflex Mass peristalsis movements push fecal material from the sigmoid colon into the rectum. This causes distention of the rectal wall, which stimulates stretch receptors and initiates a defecation reflex that empties the rectum. This reflex opens the internal anal sphincter. The external anal sphincter is voluntarily controlled. Diarrhea Diarrhea is an increase in the frequency, volume, and fluid content of the feces caused by increased motility and decreased absorption by the intestines. Frequent diarrhea can result in dehydration and electrolyte imbalances. Excessive motility can be caused by lactose intolerance, stress, and microbes that irritate the gastrointestinal mucosa. Constipation Constipation refers to infrequent or difficult defecation caused by decreased motility of the intestines. Feces remain in the LI for prolonged periods of time. This causes increased water absorption and the feces become dry and hard. Constipation Constipation can be caused by poor habits (delaying defecation), spasms, insufficient fiber in the diet, inadequate fluid intake, lack of exercise, emotional stress, and certain drugs. Constipation Treatment often involves laxatives to induce defecation. Laxatives can be habit forming; therefore, adding fiber to the diet, increasing the amount of exercise, and increasing fluid intake are safer ways to control the problem. Dietary Fiber Dietary fiber consists of indigestible plant carbohydrates such as cellulose, lignin, and pectin. These are found in fruits, vegetables, grains, and beans. Dietary Fiber Insoluble fiber does not dissolve in water. Insoluble fiber speeds up passage of materials through the track. Woody or structural parts of plants include the skins of fruits and vegetables and the bran coating around wheat and corn kernels. Dietary Fiber Soluble fiber dissolves in water and forms a gel that slows passage of material through the tract. Soluble fiber is found in beans, oats, barley, broccoli, prunes, apples, and citrus fruits.