Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
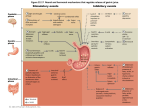
PowerPoint® Lecture Slides prepared by Janice Meeking, Mount Royal College CHAPTER 23 The Digestive System: Part B Copyright © 2010 Pearson Education, Inc. Pharynx • Oropharynx and laryngopharynx • Allow passage of food, fluids, and air • Stratified squamous epithelium lining • Skeletal muscle layers: inner longitudinal, outer pharyngeal constrictors Copyright © 2010 Pearson Education, Inc. Esophagus • Flat muscular tube from laryngopharynx to stomach • Pierces diaphragm at esophageal hiatus • Joins stomach at the cardiac orifice Copyright © 2010 Pearson Education, Inc. Esophagus • Esophageal mucosa contains stratified squamous epithelium • Changes to simple columnar at the stomach • Esophageal glands in submucosa secrete mucus to aid in bolus movement • Muscularis: skeletal superiorly; smooth inferiorly • Adventitia instead of serosa Copyright © 2010 Pearson Education, Inc. (a) Copyright © 2010 Pearson Education, Inc. Mucosa (contains a stratified squamous epithelium) Submucosa (areolar connective tissue) Lumen Muscularis externa • Longitudinal layer • Circular layer Adventitia (fibrous connective tissue) Figure 23.12a Mucosa (contains a stratified squamous epithelium) (b) Copyright © 2010 Pearson Education, Inc. Figure 23.12b Go to GI Diseases (Esophagus) Copyright © 2010 Pearson Education, Inc. Digestive Processes: Mouth • Ingestion • Mechanical digestion • Mastication is partly voluntary, partly reflexive • Chemical digestion (salivary amylase and lingual lipase) • Propulsion • Deglutition (swallowing) Copyright © 2010 Pearson Education, Inc. Deglutition • Involves the tongue, soft palate, pharynx, esophagus, and 22 muscle groups • Buccal phase • Voluntary contraction of the tongue • Pharyngeal-esophageal phase • Involuntary • Control center in the medulla and lower pons Copyright © 2010 Pearson Education, Inc. Bolus of food Tongue Uvula Pharynx Bolus Epiglottis Epiglottis Glottis Trachea Bolus Esophagus 1 Upper esophageal sphincter is contracted. During the buccal phase, the tongue presses against the hard palate, forcing the food bolus into the oropharynx where the involuntary phase begins. Relaxed muscles 2 The uvula and larynx rise to prevent food from entering respiratory passageways. The tongue blocks off the mouth. The upper esophageal sphincter relaxes, allowing food to enter the esophagus. 4 Food is moved through the esophagus to the stomach by peristalsis. Circular muscles contract Bolus of food 3 The constrictor muscles of the pharynx contract, forcing food into the esophagus inferiorly. The upper esophageal sphincter contracts (closes) after entry. Relaxed muscles 5 The gastroesophageal sphincter opens, and food enters the stomach. Longitudinal muscles contract Gastroesophageal sphincter closed Gastroesophageal sphincter opens Stomach Copyright © 2010 Pearson Education, Inc. Figure 23.13 Bolus of food Tongue Pharynx Epiglottis Glottis Trachea 1 Upper esophageal sphincter is contracted. During the buccal phase, the tongue presses against the hard palate, forcing the food bolus into the oropharynx where the involuntary phase begins. Copyright © 2010 Pearson Education, Inc. Figure 23.13, step 1 Bolus 3 The constrictor muscles of the pharynx contract, forcing food into the esophagus inferiorly. The upper esophageal sphincter contracts (closes) after entry. Copyright © 2010 Pearson Education, Inc. Figure 23.13, step 3 Uvula Bolus Epiglottis Esophagus 2 The uvula and larynx rise to prevent food from entering respiratory passageways. The tongue blocks off the mouth. The upper esophageal sphincter relaxes, allowing food to enter the esophagus. Copyright © 2010 Pearson Education, Inc. Figure 23.13, step 2 Relaxed muscles Circular muscles contract 4 Food is moved through the esophagus to the stomach by peristalsis. Bolus of food Longitudinal muscles contract Gastroesophageal sphincter closed Stomach Copyright © 2010 Pearson Education, Inc. Figure 23.13, step 4 Relaxed muscles 5 The gastroesophageal sphincter opens, and food enters the stomach. Gastroesophageal sphincter opens Copyright © 2010 Pearson Education, Inc. Figure 23.13, step 5 Bolus of food Tongue Uvula Pharynx Bolus Epiglottis Epiglottis Glottis Trachea Bolus Esophagus 1 Upper esophageal sphincter is contracted. During the buccal phase, the tongue presses against the hard palate, forcing the food bolus into the oropharynx where the involuntary phase begins. Relaxed muscles 2 The uvula and larynx rise to prevent food from entering respiratory passageways. The tongue blocks off the mouth. The upper esophageal sphincter relaxes, allowing food to enter the esophagus. 4 Food is moved through the esophagus to the stomach by peristalsis. Circular muscles contract Bolus of food 3 The constrictor muscles of the pharynx contract, forcing food into the esophagus inferiorly. The upper esophageal sphincter contracts (closes) after entry. Relaxed muscles 5 The gastroesophageal sphincter opens, and food enters the stomach. Longitudinal muscles contract Gastroesophageal sphincter closed Gastroesophageal sphincter opens Stomach Copyright © 2010 Pearson Education, Inc. Figure 23.13 Stomach: Gross Anatomy • Cardiac region (cardia) • Surrounds the cardiac orifice • Fundus • Dome-shaped region beneath the diaphragm • Body • Midportion Copyright © 2010 Pearson Education, Inc. Stomach: Gross Anatomy • Cardiac region (cardia) • Surrounds the cardiac orifice • Fundus • Dome-shaped region beneath the diaphragm • Body • Midportion Copyright © 2010 Pearson Education, Inc. Stomach: Gross Anatomy • Pyloric region: antrum, pyloric canal, and pylorus • Pylorus is continuous with the duodenum through the pyloric valve (sphincter) • Greater curvature • Convex lateral surface • Lesser curvature • Concave medial surface Copyright © 2010 Pearson Education, Inc. Cardia Esophagus Muscularis externa • Longitudinal layer • Circular layer • Oblique layer Lesser curvature Fundus Serosa Body Lumen Rugae of mucosa Greater curvature Duodenum (a) Copyright © 2010 Pearson Education, Inc. Pyloric Pyloric canal antrum Pyloric sphincter (valve) at pylorus Figure 23.14a Stomach: Gross Anatomy • Lesser omentum • From the liver to the lesser curvature • Greater omentum • Drapes from greater curvature • Anterior to the small intestine • The omenta have fat deposits and lots of lymph nodes. The immune cells and macrophages in the omenta police the peritoneal cavity. The omenta can wall off peritoneal infections. Copyright © 2010 Pearson Education, Inc. Greater and Lesser Omentums Copyright © 2010 Pearson Education, Inc. • ANS nerve supply to stomach • Sympathetic via splanchnic nerves and celiac plexus • Parasympathetic via vagus nerve Copyright © 2010 Pearson Education, Inc. • Blood supply to Stomach • Celiac trunk – branches go to liver, stomach, spleen, pancreas • Veins of the hepatic portal system Copyright © 2010 Pearson Education, Inc. Inferior vena cava (not part of hepatic portal system) Hepatic veins Liver Hepatic portal vein Small intestine Gastric veins Spleen Inferior vena cava Splenic vein Right gastroepiploic vein Inferior mesenteric vein Superior mesenteric vein Large intestine Rectum (c) The hepatic portal circulation. Copyright © 2010 Pearson Education, Inc. Figure 19.29c Diaphragm Abdominal aorta Inferior phrenic arteries Celiac Trunk L. gastric artery Common hepatic artery Celiac trunk Splenic artery Middle suprarenal arteries R. gastric artery Hepatic L artery proper Gastroduodenal R artery R. gastroepiploic artery L. gastroepiploic artery Middle Intestinal arteries colic artery Superior mesenteric artery R. colic artery Renal arteries Gonadal arteries Ileocolic artery Sigmoidal arteries Inferior mesenteric artery L. colic artery Lumbar arteries (a) Schematic flowchart. Copyright © 2010 Pearson Education, Inc. Superior rectal artery Median sacral artery Common iliac arteries Figure 19.24a Liver (cut) Inferior vena cava Diaphragm Esophagus Celiac trunk Common hepatic artery Hepatic artery proper Gastroduodenal artery Right gastric artery Gallbladder Left gastric artery Stomach Splenic artery Pancreas (major portion lies posterior to stomach) Right gastroepiploic artery Superior mesenteric mesenteric Duodenum Abdominal aorta Left gastroepiploic artery Spleen (b) The celiac trunk and its major branches. The left half of the liver has been removed. Copyright © 2010 Pearson Education, Inc. Figure 19.24b Falciform ligament Liver Gallbladder Spleen Stomach Ligamentum teres Greater omentum Small intestine Cecum (a) The Ligamentum Teres Hepatis is the remnant of the umbilical vein Copyright © 2010 Pearson Education, Inc. Figure 23.30a Stomach: Microscopic Anatomy • Four tunics • Muscularis and mucosa are modified • Muscularis externa • Three layers of smooth muscle • Inner oblique layer allows stomach to churn, mix, move, and physically break down food Copyright © 2010 Pearson Education, Inc. Liver Gallbladder Lesser omentum Stomach Duodenum Transverse colon Small intestine Cecum Urinary bladder Copyright © 2010 Pearson Education, Inc. (b) Figure 23.30b Surface epithelium Mucosa Lamina propria Submucosa (contains submucosal plexus) Muscularis externa (contains myenteric plexus) Serosa Muscularis mucosae Oblique layer Circular layer Longitudinal layer (a) Layers of the stomach wall (l.s.) Copyright © 2010 Pearson Education, Inc. Stomach wall Figure 23.15a Stomach: Microscopic Anatomy • Mucosa • Simple columnar epithelium composed of mucous cells – they produce a cloudy two layer coat of alkaline mucus which the surface layer consists of a viscous-insoluble mucus that traps bicarbonate-rich fluid beneath it • The smooth lining is lined with dotted Gastric pits that lead into gastric glands that produce the various gastric juices Copyright © 2010 Pearson Education, Inc. • The cells forming the walls of the gastric pits are primarily mucous cells – but the gastric gland cells differ in the different regions of the stomach. • Cardia (entrance) and pylorus (exit) are primarily mucus secreting cells • Pyloric Antrum produce mucus and hormones (enteroendocrine cells) • Fundus and body – where most chemical digestion occurs produce the majority of stomach secretions Copyright © 2010 Pearson Education, Inc. Gastric pits Surface epithelium (mucous cells) Gastric pit Mucous neck cells Parietal cell Chief cell Gastric gland Enteroendocrine cell (b) Enlarged view of gastric pits and gastric glands Copyright © 2010 Pearson Education, Inc. Figure 23.15b Gastric Glands • Cell types • Mucous neck cells (secrete thin, acidic mucus) • Parietal cells • Chief cells • Enteroendocrine cells Copyright © 2010 Pearson Education, Inc. Pepsinogen HCl Pepsin Mitochondria Parietal cell Chief cell Enteroendocrine cell (c) Location of the HCl-producing parietal cells and pepsin-secreting chief cells in a gastric gland Copyright © 2010 Pearson Education, Inc. Figure 23.15c Gastric Gland Secretions • Glands in the fundus and body produce most of the gastric juice • Parietal cell secretions • HCl • pH 1.5–3.5 denatures protein in food, activates pepsin, and kills many bacteria • Intrinsic factor • Glycoprotein required for absorption of vitamin B12 in small intestine Copyright © 2010 Pearson Education, Inc. Gastric Gland Secretions • Chief cell secretions • Inactive enzyme pepsinogen • Activated to pepsin by HCl and by pepsin itself (a positive feedback mechanism) • Chief cells also secrete insignificant amounts of gastric lipase Copyright © 2010 Pearson Education, Inc. Gastric Gland Secretions • Enteroendocrine cells • Secrete chemical messengers into the lamina propria • Paracrines • Serotonin and histamine • Hormones • Somatostatin and gastrin Copyright © 2010 Pearson Education, Inc. Mucosal Barrier • Layer of bicarbonate-rich mucus • Tight junctions between epithelial cells • Damaged epithelial cells are quickly replaced by division of stem cells – that reside where the gastric pits join the gastric glands. • The surface epithelia are replaced every three to six days Copyright © 2010 Pearson Education, Inc. Homeostatic Imbalance • Gastritis: inflammation caused by anything that breaches the mucosal barrier • Peptic or gastric ulcers: erosion of the stomach wall • Most are caused by Helicobacter pylori bacteria • Go to GI Diseases PowerPoint Copyright © 2010 Pearson Education, Inc. Bacteria Mucosa layer of stomach (a) A gastric ulcer lesion Copyright © 2010 Pearson Education, Inc. (b) H. pylori bacteria Figure 23.16 Digestive Processes in the Stomach • Physical digestion • Denaturation of proteins • Enzymatic digestion of proteins by pepsin (and rennin in infants) • Secretes intrinsic factor required for absorption of vitamin B12 • Lack of intrinsic factor pernicious anemia • Delivers chyme to the small intestine Copyright © 2010 Pearson Education, Inc. Regulation of Gastric Secretion • Gastric Secretion has three phases – (1) Cephalic (2) Gastric and (3) Intestinal. • Some are more stimulatory – Cephalic and Gastric and one is more inhibitory – Intestinal Phase • Neural (vagus and enteric plexus) and hormonal mechanisms control the secretions 1. Cephalic (reflex) phase: last just a few minutes prior to food entry into the stomach. It occurs even if you don’t actually get the food – if you desire the food and are not depressed or have a lack of appetite Copyright © 2010 Pearson Education, Inc. Gastric Phase • Lasts approximately 3–4 hours after food enters the stomach • Stimuli for this phase is gastric distention, peptides, and low acidity • Gastric Distention activates stretch receptors and initiates both local (myenteric) reflexes and vagovagal – both stimulate acetylcholine release Copyright © 2010 Pearson Education, Inc. Gastrin (1) • Gastrin is secreted by G-cells in the Pyloric Antrum in accordance with chemical stimuli and neural stimuli • The chemical stimuli for Gastrin secretion are partially digested proteins, caffeine, and rising alkaline pH. High acidity less than a pH of 2 inhibits Gastrin secretion • Gastric stimulates release of enzymes, also Histamine from the enterochromaffin cells – but its main targets are the Parietal cells in body of the stomach that secrete HCl- prodding them to secrete increased amounts of HCl Copyright © 2010 Pearson Education, Inc. Gastrin (2) • When protein products enter the stomach, the pH generally rises due to the proteins buffering H+. • The rising pH stimulates Gastrin which causes HCl to spew out thus denaturing the proteins. The more proteins the more Gastrin. • As proteins are decomposed the acidity rises and Gastrin is inhibited Copyright © 2010 Pearson Education, Inc. Gastrin (3) • In addition to G-cells being stimulated chemically – they are also stimulated neurally. The parasympathetic turns on secretion via acetylcholine from the Vagus and Sympathetic turns it off • The vagus was activated in the Cephalic Phase and Gastric Phase due to stomach distention • Emotional upset, fear, anxiety, and anything that triggers the fight and flight response turns off Gastric secretion. Copyright © 2010 Pearson Education, Inc. Stimulatory events Cephalic phase Gastric phase 1 Sight and thought of food Cerebral cortex Conditioned reflex 2 Stimulation of taste and smell receptors Hypothalamus and medulla oblongata 1 Stomach distension activates stretch receptors Vagovagal reflexes 1 Presence of low pH, partially digested foods, fats, or hypertonic solution in duodenum when stomach begins to empty Stimulate Inhibit Copyright © 2010 Pearson Education, Inc. Medulla Vagus nerve Vagus nerve Local reflexes 2 Food chemicals G cells (especially peptides and caffeine) and rising pH activate chemoreceptors Intestinal phase Inhibitory events Gastrin release to blood Intestinal (enteric) gastrin release to blood Lack of stimulatory impulses to parasympathetic center Cerebral cortex Gastrin secretion declines G cells Overrides parasympathetic controls Sympathetic nervous system activation 1 Excessive acidity (pH <2) in stomach 2 Emotional upset Stomach secretory activity Enterogastric reflex Brief effect 1 Loss of appetite, depression Local reflexes Vagal nuclei in medulla Pyloric sphincter 1 Distension of duodenum; presence of fatty, acidic, hypertonic chyme, and/or irritants in the duodenum 2 Distension; Release of intestinal presence of hormones (secretin, cholecystokinin, vasoactive fatty, acidic, partially intestinal peptide) digested food in the duodenum Figure 23.17 Regulation and Mechanism of HCl Secretion • Three chemicals (ACh, histamine, and gastrin) stimulate parietal cells through second-messenger systems • All three are necessary for maximum HCl secretion • Antihistamines block H2 receptors and decrease HCl release Copyright © 2010 Pearson Education, Inc. Secondary Messenger Systems for HCl release • Acetylcholine and Gastrin increase intracellular Calcium levels. • Histamine released by the enterochromaffinlike cells in response to Gastrin and to a lesser extent by Ach acts through the cyclic AMP system. Copyright © 2010 Pearson Education, Inc. Blood capillary Chief cell CO2 CO2 + H2O Carbonic H2CO3 anhydrase H+ K+ Stomach lumen H+-K+ ATPase H+ K+ HCO3– Alkaline tide HCI Parietal cell HCO3– Cl– Cl– HCO3–- Cl– antiporter Cll– Interstitial fluid Copyright © 2010 Pearson Education, Inc. Figure 23.18 Regulation of Gastric Secretion 3. Intestinal phase: brief stimulatory effect as partially digested food enters the duodenum, followed by inhibitory effects (enterogastric reflex and enterogastrones) Some actions are excitatory and some are inhibitory As partially digested foods fill the initial part of the small intestine (duodenum). This action stimulates the release of intestinal Gastrin. This stimulates the stomach to continue its secretory activity. However, this action is brief. Copyright © 2010 Pearson Education, Inc. • The action is brief due to the fact that as the intestines fill with chyme containing large amounts of H+, fats, partially digested proteins and various irritating substances, the inhibitory component is triggered in the form of the enterogastric reflex • The enterogastric reflex is a trio of reflexes that (1) inhibit the vagal nuclei in the medulla (2) inhibit local reflexes and (3) activate sympathetic fibers that cause the pyloric sphincter to tighten and prevent further food entry. • The purpose of this inhibitory action is to not fill the duodenum with excess acidity and match the small intestines processing time. • Additionally there is a release of several intestinal hormones – termed enterogastrones (Secretin, Cholecystokinin, and Vasoactive Intestinal Peptide). All are inhibitory on the stomach. Copyright © 2010 Pearson Education, Inc. Response of the Stomach to Filling • Stretches to accommodate incoming food • Reflex-mediated receptive relaxation • Coordinated by the swallowing center of the brain stem and mediated by the vagus nerves acting on Serotonin and Nitric Oxide releasing enteric neurons • Gastric accommodation • Plasticity (stress-relaxation response) of smooth muscle Copyright © 2010 Pearson Education, Inc. • Small rippling waves in the body and fundus of stomach where good (food storage) chemical digestion occur • Waves get stronger in pyloric antrum. The pyloric region which holds about 30 cc of chyme acts as a dynamic filter that allows only liquids and small particles to pass through the barely open pyloric valve during the digestive process. • Normally each peristaltic wave reaching the pyloric muscle squirts only 3 cc or less of chyme into the small intestines. Because the contraction also closes the pyloric valve, which is normally partially relaxed, the rest (27 cc) goes back into the stomach to be better mixed. Copyright © 2010 Pearson Education, Inc. Gastric Contractile Activity • The intensity of peristaltic waves can be changed but the rate is constant – about 3 waves per minute. • Pacemaker cells (cells of Cajal) located in the longitudinal muscle layer – automatically depolarize and repolarize setting the cyclic slow waves – also known as the Basic electrical rhythm (BER) • The smooth muscle cells are connected by gap junctions to the rest of muscularis – the waves are efficiently transmitted. Copyright © 2010 Pearson Education, Inc. • The pacemakers set the maximum rate of contraction, but they do not initiate the contractions or regulate the force. • They generate subthreshold depolarization waves, which are then ignited (enhanced by further depolarization and brought to threshold) by neural and hormonal factors. • Factors that increase the strength of contractions are the same factors that enhance stomach secretions. Copyright © 2010 Pearson Education, Inc. Gastric Contractile Activity • Most vigorous near the pylorus • Chyme is either • Delivered in ~ 3 ml spurts to the duodenum, or • Forced backward into the stomach Copyright © 2010 Pearson Education, Inc. Pyloric valve closed 1 Propulsion: Peristaltic waves move from the fundus toward the pylorus. Copyright © 2010 Pearson Education, Inc. Pyloric valve closed 2 Grinding: The most vigorous peristalsis and mixing action occur close to the pylorus. Pyloric valve slightly opened 3 Retropulsion: The pyloric end of the stomach acts as a pump that delivers small amounts of chyme into the duodenum, simultaneously forcing most of its contained material backward into the stomach. Figure 23.19 Regulation of Gastric Emptying • The stomach usually empties completely within 4 hours after a meal. • The larger the meal (more stomach distention) and the more liquid the meal is – the faster it empties. • Fluids pass quickly through the stomach. • Solids take longer in that they need to be processed more • The rate of gastric emptying depends not only on the stomach but just as much on the small intestines processing time. Too much release into the small intestine (too much stretch) initiates the enterogastric reflex. Copyright © 2010 Pearson Education, Inc. Gastric Emptying • Carbohydrate-rich chyme moves quickly through the duodenum • Fatty chyme remains in the duodenum 6 hours or more Copyright © 2010 Pearson Education, Inc. Presence of fatty, hypertonic, acidic chyme in duodenum Duodenal enteroendocrine cells Chemoreceptors and stretch receptors Secrete Enterogastrones (secretin, cholecystokinin, vasoactive intestinal peptide) Duodenal stimuli decline Initial stimulus Physiological response Result Copyright © 2010 Pearson Education, Inc. Target Via short reflexes Enteric neurons Contractile force and rate of stomach emptying decline Via long reflexes CNS centers sympathetic activity; parasympathetic activity Stimulate Inhibit Figure 23.20 Vomiting and Gastroparesis • Vomiting is caused by many factors – with the most common being extreme stretching of the stomach and/or intestines. Other factors are bacterial toxins, excessive alcohol, spicy foods, and certain drugs. • Both bloodborne molecules and sensory impulses going to the emetic center in the medulla initiate the events for vomiting. Copyright © 2010 Pearson Education, Inc. Gastroparesis • Gastroparesis, also called delayed gastric emptying, is a medical condition consisting of a paresis (partial paralysis) of the stomach, resulting in food remaining in the stomach for a longer period of time than normal. Normally, the stomach contracts to move food down into the small intestine for digestion. The vagus nerve controls these contractions. Gastroparesis may occur when the vagus nerve is damaged and the muscles of the stomach and intestines do not work normally. Food then moves slowly or stops moving through the digestive tract. Copyright © 2010 Pearson Education, Inc. Causes • Gastroparesis may be chronic or transient; transient gastroparesis may arise in acute illness of any kind, with the use of certain cancer treatments or other drugs which affect digestive action, or due to anorexia nervosa, bulimia and other abnormal eating patterns. • Chronic gastroparesis is frequently due to autonomic neuropathy. This may occur in people with type 1 diabetes or type 2 diabetes. The vagus nerve becomes damaged by years of high blood glucose, resulting in gastroparesis. Gastroparesis has also been associated with various autoimmune diseases and syndromes, such as fibromyalgia and Parkinson's disease, and may occur as part of a mitochondrial disorder. Copyright © 2010 Pearson Education, Inc. Small Intestine: Gross Anatomy • Major organ of digestion and absorption • 2–4 m (20 feet long in cadaver but 7 -13 feet long in living person); extends from pyloric sphincter to ileocecal valve – approximately 200 square meters of surface area (doubles tennis court) • Subdivisions 1. Duodenum (retroperitoneal) 10 inches 2. Jejunum (attached posteriorly by mesentery) 8 feet 3. Ileum (attached posteriorly by mesentery) 12 feet Copyright © 2010 Pearson Education, Inc. • The Ligament of Treitz (named after Václav Treitz) connects the duodenum of the small intestines to the diaphragm. It contains a slender band of skeletal muscle from the diaphragm and a fibromuscular band of smooth muscle from the horizontal and ascending parts of the duodenum. When it contracts, the suspensory muscle of the duodenum widens the angle of the duodenojejunal flexure, allowing movement of the intestinal contents Copyright © 2010 Pearson Education, Inc. Mouth (oral cavity) Tongue Esophagus Liver Gallbladder Duodenum Jejunum Small intestine Ileum Anus Copyright © 2010 Pearson Education, Inc. Parotid gland Sublingual gland Salivary Submandibular glands gland Pharynx Stomach Pancreas (Spleen) Transverse colon Descending colon Ascending colon Large Cecum intestine Sigmoid colon Rectum Vermiform appendix Anal canal Figure 23.1 Duodenum • The bile duct and main pancreatic duct • Join at the hepatopancreatic ampulla • Enter the duodenum at the major duodenal papilla • Are controlled by the hepatopancreatic sphincter Copyright © 2010 Pearson Education, Inc. Right and left hepatic ducts of liver Cystic duct Common hepatic duct Bile duct and sphincter Accessory pancreatic duct Mucosa with folds Gallbladder Major duodenal papilla Hepatopancreatic ampulla and sphincter Copyright © 2010 Pearson Education, Inc. Tail of pancreas Pancreas Jejunum Duodenum Main pancreatic duct and sphincter Head of pancreas Figure 23.21 Structural Modifications • Increase surface area of proximal part for nutrient absorption • Circular folds (plicae circulares) 1 cm tall – permanent folds of mucosae and submucosa • Villi – 1 mm high • Microvilli Copyright © 2010 Pearson Education, Inc. Structural Modifications • Circular folds • Permanent (~1 cm deep) • Force chyme to slowly spiral through lumen Copyright © 2010 Pearson Education, Inc. Vein carrying blood to hepatic portal vessel Muscle layers Circular folds Villi Lumen (a) Copyright © 2010 Pearson Education, Inc. Figure 23.22a Structural Modifications • Villi (gives a velvety look) • Motile fingerlike extensions (~1 mm high) of the mucosa • Villus epithelium • Simple columnar absorptive cells (enterocytes) • Goblet cells • In the core of each villus is a dense capillary bed and a wide lymph capillary called a lacteal. Copyright © 2010 Pearson Education, Inc. • The villi are large and leaflike in the duodenum and gradually narrow and shorten along the length of the small intestine. • A slip of smooth muscle in the villus core allows it to alternatively shorten and lengthen. • The pulsations (1) increase the contact between the villus and contents of the intestinal lumen making better absorption and (2) milk lymph along the lacteals. Copyright © 2010 Pearson Education, Inc. Structural Modifications • Microvilli • Projections (brush border) of absorptive cells • Bear brush border enzymes – these enzymes complete the digestive process Copyright © 2010 Pearson Education, Inc. Histology of Intestinal Wall • Epithelium of the villus is largely simple columnar absorptive cells bound by tight junctions and richly endowed with microvilli. • Goblet cells • Between the villi are intestinal pits that lead into tubular glands called intestinal crypts – also known as the crypts of Lieberkühn. Copyright © 2010 Pearson Education, Inc. Intestinal Crypts • Intestinal crypt epithelium • Primarily composed of secretory cells that produce intestinal juice – a watery mixture containing mucus that serves as a carrier fluid for absorbing nutrients from chyme • Enteroendocrine cells – source of the enterogastrones (Secretin and CCK) • Intraepithelial lymphocytes (IELs) – these are T-cells that do not need priming – upon encountering antiges they immediately release killing cytokines • Release cytokines that kill infected cells • Paneth cells – release defensins and lysozyme • Stem cells – can differentiate – become specialized absorptive cells, goblet cells, and enteroendocrine cells. Copyright © 2010 Pearson Education, Inc. • The stem cells migrate up to become the epithelial cells – the existent epithelial cells undergo apoptosis and are shed from the villus tips, renewing the villus epithelium every two days. • but when the stem cells differentiate into Paneth cells – they stay at the base • The crypts decrease in number along the length of the small intestine, but the goblet cells become more abundant. Copyright © 2010 Pearson Education, Inc. Microvilli (brush border) Absorptive cells Lacteal Goblet cell Blood capillaries Mucosa associated lymphoid tissue Intestinal crypt Muscularis mucosae Duodenal gland (b) Copyright © 2010 Pearson Education, Inc. Vilus Enteroendocrine cells Venule Lymphatic vessel Submucosa Figure 23.22b Submucosa • Typical areolar connective tissue • Contains individual and aggregated lymphoid follicles • Peyer’s patches (aggregated lymphoid follicles) – increase in number as go towards end of small intestine. They protect distal part against bacteria since normal flora increases there. • Also contains proliferating lymphocytes that leave the intestine enter blood stream and then return to home in the submucosa to produce IgA Copyright © 2010 Pearson Education, Inc. Submucosal Duodenal Glands • Duodenal (Brunner’s) glands of the duodenum secrete alkaline mucus • The glands help neutralize acidic chyme moving in from the stomach • When this protection is absent or insufficient – duodenal ulcers can occur • The muscularis of the small intestine is bilayered and except for the duodenum which is retroperitoneal and has an adventitia, the external intestinal surface is covered by a visceral peritoneum Copyright © 2010 Pearson Education, Inc. Intestinal Juice • Normally secrete 1 to 2 ml of intestinal juice daily – that facilitates transport and absorption of nutrients • Secreted in response to distension or irritation of the mucosa by hypertonic or acidic chyme. • Slightly alkaline (7.4 – 7.8) and isotonic with blood plasma • Largely water, enzyme-poor, due to the fact that enzymes are limited to the intestinal enzymes bound to brush border. It does contain contains mucus – secreted by goblet cells and duodenal glands Copyright © 2010 Pearson Education, Inc. Liver • Largest gland in the body • Four lobes—right, left, caudate, and quadrate Copyright © 2010 Pearson Education, Inc. Liver • Falciform ligament • Separates the (larger) right and (smaller) left lobes • Suspends liver from the diaphragm and anterior abdominal wall • Round ligament (ligamentum teres) • Remnant of fetal umbilical vein along free edge of falciform ligament Copyright © 2010 Pearson Education, Inc. Sternum Nipple Liver Bare area Falciform ligament Left lobe of liver Right lobe of liver Gallbladder (a) Copyright © 2010 Pearson Education, Inc. Round ligament (ligamentum teres) Figure 23.24a Sternum Nipple Liver Lesser omentum (in fissure) Left lobe of liver Porta hepatis containing hepatic artery (left) and hepatic portal vein (right) Quadrate lobe of liver Ligamentum teres Bare area Caudate lobe of liver Sulcus for inferior vena cava Hepatic vein (cut) Bile duct (cut) Right lobe of liver Gallbladder (b) Copyright © 2010 Pearson Education, Inc. Figure 23.24b Liver: Associated Structures • Lesser omentum anchors liver to stomach • Hepatic artery and vein at the porta hepatis • Bile ducts • Common hepatic duct leaves the liver • Cystic duct connects to gallbladder • Bile duct formed by the union of the above two ducts Copyright © 2010 Pearson Education, Inc. Right and left hepatic ducts of liver Cystic duct Common hepatic duct Bile duct and sphincter Accessory pancreatic duct Mucosa with folds Gallbladder Major duodenal papilla Hepatopancreatic ampulla and sphincter Copyright © 2010 Pearson Education, Inc. Tail of pancreas Pancreas Jejunum Duodenum Main pancreatic duct and sphincter Head of pancreas Figure 23.21 Liver: Microscopic Anatomy • Liver lobules • Hexagonal structural and functional units • Filter and process nutrient-rich blood • Composed of plates of hepatocytes (liver cells) • Longitudinal central vein Copyright © 2010 Pearson Education, Inc. (a) Lobule Copyright © 2010 Pearson Education, Inc. (b) Central vein Connective tissue septum Figure 23.25a, b Liver: Microscopic Anatomy • Portal triad at each corner of lobule • Bile duct receives bile from bile canaliculi • Portal arteriole is a branch of the hepatic artery • Hepatic venule is a branch of the hepatic portal vein • Liver sinusoids are leaky capillaries between hepatic plates • Kupffer cells (hepatic macrophages) in liver sinusoids Copyright © 2010 Pearson Education, Inc. Interlobular veins (to hepatic vein) Central vein Sinusoids Bile canaliculi Plates of hepatocytes Bile duct (receives bile from bile canaliculi) Fenestrated lining (endothelial cells) of sinusoids Portal vein Hepatic macrophages in sinusoid walls Bile duct Portal venule Portal arteriole Portal triad (c) Copyright © 2010 Pearson Education, Inc. Figure 23.25c Liver: Microscopic Anatomy • Hepatocyte functions (see MS Word Liver Functions for complete list) • Process bloodborne nutrients • Store fat-soluble vitamins • Perform detoxification • Produce ~900 ml bile per day • Stores glycogen Copyright © 2010 Pearson Education, Inc. Liver Regeneration • The regenerative ability of the liver is exceptional. It can regenerate to its former size even if 70% is removed. • Liver cells secrete VEGF (Vascular Endothelial Growth Factor) which binds to specific receptors on endothelial cells lining the sinusoids. • The endothelial cells proliferate and release other growth factors, such as hepatocyte growth factor (HGF) and interleukin 6. Copyright © 2010 Pearson Education, Inc. Bile • Yellow-green, alkaline solution containing • Bile salts: cholesterol derivatives that function in fat emulsification and absorption • Bilirubin: pigment formed from heme • Cholesterol, neutral fats, phospholipids, and electrolytes Copyright © 2010 Pearson Education, Inc. Copyright © 2010 Pearson Education, Inc. Bile • Enterohepatic circulation • Recycles bile salts • Bile salts duodenum reabsorbed from ileum hepatic portal blood liver secreted into bile Copyright © 2010 Pearson Education, Inc. The Gallbladder • Thin-walled muscular sac on the ventral surface of the liver • Stores and concentrates bile by absorbing its water and ions • Releases bile via the cystic duct, which flows into the bile duct Copyright © 2010 Pearson Education, Inc.