Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Coronary artery disease wikipedia , lookup
Cardiac contractility modulation wikipedia , lookup
Cardiac surgery wikipedia , lookup
Myocardial infarction wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
Ventricular fibrillation wikipedia , lookup
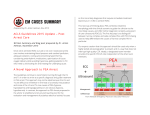
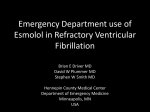
A Cure for the Code Blues? Vasopressin, Steroid and Epinephrine Cocktail for Use in Advanced Cardiac Life Support Hannah Davis, Pharm.D. PGY2 Emergency Medicine Pharmacy Resident University Health System, San Antonio, TX Division of Pharmacotherapy, The University of Texas at Austin College of Pharmacy Pharmacotherapy Education and Research Center, University of Texas Health Science Center at San Antonio August 28, 2015 Learning Objectives 1. Define therapeutic endpoints for basic life support and advanced cardiac life support (ACLS) 2. Describe the current level of evidence for vasopressor agents recommended by national ACLS guidelines 3. Identify complications following return of spontaneous circulation which may decrease survival 4. Analyze evidence for role of combination vasopressin, steroids and epinephrine in ACLS I. Cardiac arrest (CA) Figure 1. Introduction to CA Medical emergency Sudden cessation of effective blood circulation Prevents delivery of oxygen and nutrients Results in loss of consciousness and death A. Incidence1,2 i. Out-of-hospital cardiac arrests (OHCA): 94 per year per 100,000 people ii. In-hospital cardiac arrests (IHCA): 1-5 per 1,000 patient admissions a. Bias due to lack of official reporting and documenting B. Survival rates1-7 i. Favorable determinants a. Younger age b. Fewer comorbidities c. Ventricular fibrillation (VFib) or pulseless ventricular tachycardia (VTach) d. Witnessed arrest e. Shorter time to chest compressions and defibrillation f. Shorter duration of code g. IHCA h. Occurrence during the day on a weekday ii. National OHCA survival to hospital discharge: 3-16% iii. National IHCA survival to hospital discharge: 23% a. VFib or VTach: 18-64% b. Pulseless electrical activity (PEA) or asystole arrests: 1-14% iv. 60% of patients do not survive to discharge after return of spontaneous circulation (ROSC) a. Most deaths following ROSC occur within 24 hours v. Neurologic function a. Severe cerebral disability or vegetative state in 25-50% b. Post-cardiac arrest brain injury manifests as coma, seizures, myoclonus, neurocognitive dysfunction and brain death c. Contributory factors: microcirculatory failure, impaired cerebral autoregulation, hypercarbia, hyper/hypoxia, pyrexia, hyperglycemia and seizures H. Davis | Page 2 C. Pathophysiology of CA8-11 i. Lack of effective cardiac contraction with minimal cardiac output (CO) ii. Presenting rhythms a. Shockable 1. VTach – organized electrical activity of ventricles 2. VFib – disorganized electrical activity of ventricles b. Non-shockable 1. PEA – additional rhythms with lack of sufficient ventricular activity to generate pulse 2. Asystole – absence of detectable ventricular electrical activity aa. End-stage rhythm following prolonged VFib or PEA ab. Worst prognosis iii. Etiology a. Underlying cause 1. Non-reversible causes 2. Reversible causes, “H’s and T’s” (see Appendix A) iv. Physiologic response a. Activation of sympathetic nervous system 1. Increases plasma catecholamines 2. Releases vasopressin (VASO) and activates renin-angiotensinaldosterone system b. Hypothalamic-pituitary-adrenal (HPA) axis response Figure 2. HPA axis Posterior pituitary VASO www.paleomom.com H. Davis | Page 3 II. Basic Life Support (BLS) and Advanced Cardiac Life Support (ACLS) A. Guidelines8,12 i. American Heart Association (AHA) ACLS 2010 ii. European Resuscitation Council (ERC) 2010 Figure 3. Chest compressions8 Push hard and fast •Compression = systole •Recoil = diastole Generates CO •≥ 2 inches deep •Good recoil •≥ 100 per min •1 cycle = 2 min •Increases odds of defibrillation success Improves survival A. Defibrillation8 i. VFib or VTach rhythms following every cycle of chest compressions a. Biphasic preferred, initial 120-200 J ii. Increases survival B. Ventilation8 i. Bag-mask-valve with 100% FiO2 a. 2 breaths every 30 seconds without advanced airway b. 1 breath every 6-8 seconds with advanced airway ii. Minimize excessive ventilation a. Increases intrathoracic pressure, decreases blood flow to vital organs b. Other complications: gastric inflation, regurgitation, aspiration C. Medications in ACLS8,12,14,15 i. Administered by intravenous (IV) or intraosseous (IO) route ii. Increase cardiac and cerebral perfusion pressure iii. Facilitate restoration and maintenance of a perfusing spontaneous rhythm iv. Guideline recommended drug therapy (See Appendix B) a. All rhythms 1. Epinephrine (EPI) 2. VASO b. Refractory VFib/VTach 1. Amiodarone aa. α, β, Na+, K+, Ca++ channel antagonist ab. After 1st defibrillation attempt, following 2 minutes of chest compressions ac. Increases ROSC and survival to hospital admission H. Davis | Page 4 v. Clinically evaluated endpoints a. ROSC b. Short term survival/survival to hospital admission c. Survival to hospital discharge d. Survival to hospital discharge with favorable neurologic recovery 1. Cerebral Performance Category (CPC) (See Appendix C) e. Long term survival vi. Evidence for medications a. Increase ROSC and survival to hospital admission when compared to no medications b. Every 1 minute delay in vasopressor administration is a 4% decrease in ROSC c. None for long-term survival or favorable neurologic outcomes vii. Consider reversible causes and treat underlying pathophysiology (See Appendix A) II. EPI A. Background13,16 i. Catecholamine hormone and neurotransmitter ii. Chemical mediator conveying nerve impulses to organs (heart, lung, etc.) iii. First used in 1906 to treat CA iv. Integral part of CPR recommendations since 1974 Figure 4. EPI plasma concentrations10 250 201 (ng/mL) 200 145 150 100 50 14 25 23 10 0 Before EPI After EPI ROSC Achieved After ROSC 1 Hr After ROSC No ROSC B. Dosing8, i. 1 mg every 3-5 minutes IV/IO C. Mechanism of action8,12,17,19-24 i. α- and β-adrenergic receptor stimulation ii. α1/α2 – vasoconstriction a. Most potent catecholamine for α stimulation b. Increases coronary and cerebral perfusion pressures 1. Increases ROSC c. Decreases microcirculatory cerebral blood flow 1. Increases severity of cerebral ischemia during CPR 2. Impairs neurologic function H. Davis | Page 5 iii. β1 – inotropic, chronotropic a. No evidence of benefit from β-stimulation 1. β-agonism has demonstrated harm over BLS alone 2. Decreases survival vs. phenylephrine or EPI + esmolol 3. Increases defibrillation attempts required to attain ROSC b. Detrimental effects 1. Increases myocardial work, oxygen consumption and utilization of scarce energy reserves aa. Lactic acid production ab. Ectopic ventricular arrhythmias ac. Secondary VFib 2. Transient hypoxemia due to pulmonary arteriovenous shunting 3. Post-ROSC tachycardia and hypertension aa. Precipitates recurrence of VFib 4. Post-cardiac arrest myocardial dysfunction aa. Greater incidence of post-resuscitation shock iv. β2 – vasodilation a. Increases blood flow to skeletal muscles b. Predominantly masked by α1 effects D. Efficacy data14,25-28 Author Woodhouse et al. 1995 (n) 339 Patients Table 1. EPI vs. Placebo Intervention OHCA/IHCA Asystole or resistant VFib Prospective RCT HDE= 10 mg x 2 vs. SDE= 1 mg x 2 or placebo (not randomized) x 2 Followed by open label 1 mg EPI Retrospective EPI after ≥3 rounds defibrillation vs. no EPI regardless of defibrillation attempts Prospective observational Before vs. after protocol: EPI 1 mg x 1 prior to transport with 1 mg dose x 1 in ED Herlitz et al. 1995 1203 OHCA VFib Ong et al. 2007 1296 OHCA Olsveengen et al. 2010 851 OHCA Prospective RCT ACLS with vs. without IV access and standard drugs Jacobs et al. 2011 534 OHCA Prospective, DB, RCT EPI 1 mg vs. placebo every 3 min Results No difference in: Immediate survival Hospital discharge ↑ ROSC ↑ hospital admission No difference in: Hospital discharge No difference in: ROSC Hospital admission Hospital discharge ↑ ROSC ↑ hospital admission ↑ CPR time No difference in: Hospital discharge Favorable neurologic outcome ↑ ROSC ↑ hospital admission No difference in: Hospital discharge *All differences demonstrated statistical significance OHCA: out-of-hospital cardiac arrest; IHCA: in-hospital cardiac arrest; RCT: randomized controlled trial; HDE: high dose epinephrine; SDE: standard dose epinephrine; EPI: epinephrine; VFib: ventricular fibrillation; ROSC: return of spontaneous circulation; ED: emergency department; ACLS: advanced cardiac life support; IV: intravenous; CPR: cardiopulmonary resuscitation; DB: double blind H. Davis | Page 6 E. Bottom line19,29 i. EPI increases likelihood of achieving ROSC and survival to hospital admission ii. Effects on long-term survival remain uncertain iii. No role for higher doses a. No improvement in survival with EPI doses > 1 mg iv. Dose-dependent adverse effects a. Unfavorable neurologic outcomes III. VASO A. Background8,12 i. Endogenous peptide and antidiuretic hormone ii. Regulates water retention and electrolyte homeostasis iii. Increases peripheral vascular resistance iv. Guideline recommendations a. AHA: alternative to EPI since 2000 b. ERC: not enough evidence to recommend or refute use Figure 5. VASO plasma concentrations10 250 (pg/mL) 200 193 177 150 100 117 70 58 24 50 0 Before EPI After EPI ROSC Achieved After ROSC 1 Hr After ROSC No ROSC B. Dosing8 i. 40 units once IV/IO a. May replace first or second dose of EPI C. Mechanism of action12 i. Non-adrenergic peripheral vasoconstrictor a. Stimulates smooth muscle V1 receptors D. Physiologic effects31-35 i. Increases coronary perfusion pressure ii. Causes cerebral vasodilation iii. Minimal effect on pulmonary vasculature iv. Longer t1/2 and duration of effect than EPI a. Increases mean arterial pressure (MAP) post-resuscitation v. Potentiates release of ACTH and cortisol vi. Greater stability in acidic environment compared to catecholamines H. Davis | Page 7 E. Efficacy data35-38 Author (n) Patients Table 2. VASO vs. EPI Intervention Results ↑ ROSC Prospective, DB, RCT, VASO 40 ↑ hospital admission OHCA units x 1 vs. EPI 1 mg x 1 ↑ 24 hr survival Linder et al. 1997 40 Resistant VFib Followed by standard ACLS No difference in: medication Hospital discharge Good neurological outcome No difference in: Prospective, RCT, triple blind ROSC Stiell et al. 2001 200 IHCA VASO 40 units x 1 vs. EPI 1 mg x 1 Hospital discharge Followed by open label EPI Neurologic outcome Survival (↑ hospital admission, Prospective MC, DB, RCT ↑ hospital discharge in asystolic patients) VASO 40 units every 3 min x 2 vs. No difference in: Wenzel et al. 2004 1186 OHCA EPI 1 mg every 3 min x 2 Hospital admission Followed by open label EPI Hospital discharge Cerebral performance Results include both combo arms vs. only EPI: Prospective observational cohort ↑ ROSC (retrospective control) VASO 40 units x 1 then EPI every 3-5 ↑ hospital admission OHCA Grmec et al. 2005 109 min vs. ↑ 24 hr survival VFib/VTach EPI every 3-5 min x 3 then VASO 40 No difference in: units x 1 Hospital discharge vs. EPI every 3-5 min Neurologic outcomes *All differences demonstrated statistical significance OHCA: out-of-hospital cardiac arrest; VFib: ventricular fibrillation; DB: double blind; RCT: randomized controlled trial; EPI: epinephrine; VASO: vasopressin; ROSC: return of spontaneous circulation; hr: hour(s); IHCA: in-hospital cardiac arrest; MC: multi-centered; min: minute(s); CPR: cardiopulmonary arrest; ER: emergency room F. Bottom line35,37,38 i. Many studies included EPI administration in VASO arm ii. Conflicting results on benefit of VASO over EPI a. Some reports of increasing ROSC and hospital admission 1. Small studies 2. Predominantly with repeat dosing of VASO 3. Predominantly in asystolic patients G. EPI + VASO vs. EPI1,20,37,39,40 i. Stimulates both catecholamine and VASO receptors a. Improves perfusion of vital organs b. Decreases vasopressor-mediated adverse effects ii. EPI + VASO diminishes cerebral microvascular blood flow iii. Subgroup analysis suggests benefit in those requiring > 2 doses of initial vasopressor when VASO is combined with EPI iv. Subgroup analysis suggests benefit of EPI + VASO in patients with pH < 7.2 H. Davis | Page 8 H. Efficacy data1,32,39,41-44 Author (n) Table 3. EPI +VASO vs. EPI Patients Intervention Guyette et al. 2004 298 OHCA Callaway et al. 2006 325 OHCA Mally et al. 2006 598 OHCA Resistant to defibrillation Prospective observational VASO 40 units then EPI 1 mg every 3 min vs. EPI 1 mg every 3 min Prospective DB, MC, RCT VASO 40 units + EPI 1 mg every 3 minutes x 2 Followed by open label EPI vs. EPI 1 mg + placebo every 3 minutes x 2 Followed by open label EPI Gueugniaud et al. 2008 2894 OHCA resistant VFib/VTach Cody et al. 2010 191 OHCA Ducros et al. 2010 44 OHCA 727 OHCA/IHCA (ED patients) Ong et al. 2012 Results Retrospective VASO administration determined by physician on scene EPI 1 mg every 3-5 min + VASO 40 units x 1 vs. EPI 1 mg every 3-5 min Prospective, DB, RCT VASO 40 units x 1 vs. placebo x 1 after ≥ 1 EPI Followed by open label EPI No difference in: ROSC Hospital arrival ↑ petCO2; MAP ↑ ROSC ↑ 24 hr survival ↑ neurologic outcome upon discharge (↑ hospital discharge in asystole subgroup) No difference: Hospital discharge (↓ hospital discharge in PEA subgroup analysis) No difference in: ROSC Hospital admission Hospital discharge Neurologic recovery 1 year survival Retrospective cohort evaluating protocols VASO 40 units + EPI 1 mg Followed by EPI 1 mg every 3-5min vs. EPI 1 mg every 3 min Prospective, DB, RCT EPI 1 mg every + VASO 40 units every 5 min vs. EPI 1 mg every 5 min vs. EPI 1 mg + VASO 40 units + nitroglycerin 300 mcg every 5 min Prospective MC, DB, parallel, RCT VASO 40 units x 1 vs. EPI 1 mg x 1 Followed by open label EPI ↑ ROSC ↑ ER arrival No difference in: Hospital admission Hospital discharge No difference in: Diastolic BP ROSC ↑ hospital admission (when variables accounted for) No difference in: Hospital discharge *All differences demonstrated statistical significance OHCA: out-of-hospital cardiac arrest; EPI: epinephrine; mg: milligram; min: minute(s); VASO: vasopressin; ROSC: return of spontaneous circulation; ER: emergency room; DB: double blind; RCT: randomized controlled trial; petCO2: end-tidal carbon dioxide; hr: hour; MC: multicentered; mcg: micrograms; BP: blood pressure; IHCA: in-hospital cardiac arrest I. Bottom line40,45-48 i. Systematic reviews and meta-analyses failed to demonstrate benefit of VASO over EPI or in combination with EPI a. Secondary analysis suggests dose dependent increases in survival rates when treated with VASO vs. EPI in asystolic patients b. Largest OHCA study associated with mean time to medications > 20 minutes ii. Meta-analysis 2014, reviewing 10 RCTs a. No improvement in ROSC, survival to hospital admission or discharge H. Davis | Page 9 b. IHCA subgroup analysis 1. Higher ROSC 2. Higher survival to hospital admission and discharge 3. Favorable neurologic outcomes 4. Non-traditional, repeated dosing of vasopressin 5. All vasopressin, steroid, epinephrine (VSE) data IV. Complications after ROSC A. Adrenal insufficiency (AI) of CA11,49-52 i. Inability to adequately increase cortisol secretion in response to ACTH during and after ACLS ii. Etiology a. Adrenal gland ischemia b. Inflammatory response to ischemia results in further damage iii. Increases mortality iv. Diminishes response to catecholamines v. Leads to hemodynamic instability and circulatory collapse B. Inflammatory mediated ischemic/reperfusion injury50,52-54 i. Activation of cytokines, endotoxins, and reactive species after CA ii. Inflammatory response further damages ischemic organs a. Compounds neurologic damage b. Cytokines associated with mortality and unfavorable neurologic outcomes iii. Normal physiologic response to cytokines is stimulation of cortisol release a. Unable to adequately respond due to AI C. Post-resuscitation shock6,51,55-60 i. Precise definitions of hemodynamic instability/shock are lacking ii. Impaired contractile function and diastolic function that reverses several hours to days after resuscitation iii. Hyperdynamic phase, lasting minutes a. Tachycardia and hypertension iv. Post-resuscitation cardiovascular collapse phase a. Cardiac index (CI) and filling pressures are low 1. Lactic acid produced 2. Myocardial stunning results in left ventricular dysfunction 3. Pro-inflammatory response resulting in loss of vascular tone b. Occurs several hours after CA c. Results in multi-system organ dysfunction which may progress to mortality 1. Decreases cerebral blood flow H. Davis | Page 10 d. CI increases approximately 24 hours after arrest 1. Independent of filling pressures or inotropic agents e. Vasodilation continues and requires vasoactive drugs 1. Recovery often seen within 3 days v. Risk factors for development of post-resuscitation shock a. Fifteen minute time interval between onset of arrest and ROSC b. More frequent doses of EPI c. Greater number of defibrillation attempts vi. Treatment a. Avoid hypotension b. AHA recommends maintaining systolic blood pressure ≥ 90 mmHg and MAP ≥ 65 mmHg c. Other authors advocate for more aggressive goals 1. American Academy of Neurology and the Rocky Mountain Critical Care Conference recommend MAP goal of 80-100 mmHg aa. Based on expert opinion ab. Theoretical improvement in neurologic outcomes d. Hemodynamic instability was not associated with worse neurologic outcomes when aggressively treated 1. MAP goal ≥ 75 mmHg 2. Volume expansion based on left ventricle end diastolic pressure 3. Vasoactive drugs: epinephrine or dobutamine with advanced hemodynamic monitoring V. Steroids A. Background8,12 i. Decrease inflammatory response and regulate homeostasis ii. No role for steroids in AHA or ERC guidelines B. Cortisol plasma concentrations10,49,50,53 i. Normal range a. Without stress: 5-20 mcg/dL b. Under stress: 50-90 mcg/dL ii. Low levels during or after CA indicate lack of appropriate response a. Associated with early post-resuscitation mortality iii. Higher cortisol levels have been associated with neurologically intact survival and survival > 1 month C. Mechanism of action11 i. Regulates gene expression a. Decreases production of kinins, histamines, liposomal enzymes, prostaglandins, leukotrienes b. Inhibits cell migration to area of injury c. Decreases vessel permeability H. Davis | Page 11 D. Physiologic effects11,49,50,61,62 i. Homeostasis a. Fluid and electrolyte balance 1. Decreases cell apoptosis and provides positive inotropy through calcium homeostasis b. Maintains integrity of membrane structures ii. Anti-inflammatory a. Decreases ischemia/reperfusion injury iii. Vascular a. Decreases permeability, increases SVR b. Decreases production of vasodilators c. Increases vascular reactivity to catecholamines and angiotensin II iv. Cardiac a. Increases coronary perfusion pressure i. Increases production of coronary vasodilators b. Increases contractility v. Endocrine a. Supplements cortisol not produced during AI E. Detrimental effects62 i. Electrolyte disturbances, sodium or glucose ii. Infections iii. Negative regulation on HPA axis, may result in AI F. Dosing5,52,61 i. ACLS a. Hydrocortisone (HCT) 100 mg IV push once b. Methylprednisolone 40 mg IV push once ii. Stress dose steroids a. HCT 300 mg IV per day H. Davis | Page 12 G. Efficacy data49,52,63-66 i. Animal data demonstrates increase ROSC with corticosteroids Author (n) Patients White et al. 1976 5 IHCA Refractory VFib or asystole White et al. 1979 25 IHCA VFib or asystole Paris et al. 1984 86 OHCA PEA Grafton et al. 1988 458 After OHCA VFib or asystole Tsai et al. 2006 97 OHCA Table 4. Steroids Intervention Retrospective case series DEX 100 mg once after conventional therapy failed Plus: EPI, atropine, bicarbonate, isuprel Compared to historical control Retrospective case series DEX 100 mg once Plus: atropine, isoproterenol, EPI, calcium Compared to historical control Prospective, RCT, DB Pre-hospital DEX 100 mg vs. placebo Plus: bicarbonate, EPI, and atropine Retrospective Steroid use following ROSC for brain ischemia or lung injury Predominantly low dose DEX Prospective, non-randomized (required family member pre-approval) HCT 100 mg vs. placebo Plus: EPI, VASO in ~1/3 Results Corrected rhythm** ↑ ROSC** ↑ long term survival** No difference in: ROSC Long term survival No difference in: Regaining consciousness Hospital discharge ↑ ROSC No difference in: Adverse effects Survival Neurologic function *Unless specified, results demonstrated statistical significance **Statistical significance not evaluated IHCA: in-hospital cardiac arrest; VFib: ventricular fibrillation; DEX: dexamethasone, EPI: epinephrine; CO: cardiac output; PEA: pulseless electrical activity; ROSC: return of spontaneous circulation; OHCA: out-of-hospital cardiac arrest; RCT: randomized controlled trial; HCT: hydrocortisone; VASO: vasopressin; min: minutes H. Bottom line52,66,67 i. Weakly associated with increases in ROSC a. Time dependent b. Driven by subgroup receiving hydrocortisone within 6 min of ED arrival or 22 min from collapse ii. No role for steroid administration following ROSC to treat brain ischemia iii. No increases in adverse effects VI. VSE data A. Is a cocktail of stress hormones the solution? i. EPI has been the mainstay of ACLS drug therapy but is associated with consequences linked to worse outcomes after ROSC ii. VASO alone or in combination has not shown to be superior to EPI iii. VASO administration increases serum ACTH but does not result in an adequate physiologic response of cortisol iv. Evidence of relative AI and inflammatory mediated ischemia/reperfusion injury of CA linked to post-resuscitation shock which is known to increase mortality H. Davis | Page 13 B. Efficacy data61 Table 5. Mentzelopoulos S, Zakynthinos S, Tzoufi M, et al. Vasopressin, epinephrine, and corticosteroids for in-hospital cardiac arrest. Arch Intern Med. 2009;169:15-24. Determine if VSE supplementation during and after resuscitation improves survival in refractory IHCA Objective Prospective, single-center, double blind, placebo-controlled, parallel group, randomized controlled trial Study Design Intervention: Methylprednisolone 40 mg x 1 EPI 1 mg + VASO 20 units (per resuscitation cycle) Following ROSC, HCT 300 mg/day continuous infusion x 3-7 days, followed by taper, if postresuscitation shock present Control: Placebo x 1 EPI 1 mg + placebo (per resuscitation cycle) Following ROSC, placebo x 3-7 days, followed by taper, if post-resuscitation shock present Post-resuscitation shock – sustained > 4 hours, MAP ≤ 70 mmHg despite appropriate fluid resuscitation, or doubling of peri-arrest vasopressor requirements Patients Inclusion: IHCA with PEA/asystole or VFib/VTach after 2 defibrillation attempts Exclusion: pediatric, terminal illness, do not resuscitate order, arrest due to exsanguination, recent treatment with IV corticosteroids ITT analysis Dichotomous variables: χ or Fisher exact test Continuous variables: independent t test or Mann-Whitney exact test Linear mixed-model analysis for post-resuscitation shock Kaplan-Meier for survival Multivariate analysis for independent predictors of death VSE: n=100 ↑ ROSC: 39/48 (81%) vs. 27/52 (52%) p=0.003 ↑ survival to discharge: 9/48 (19%) vs. 2/52 (4%) p=0.02 Following ROSC: ↑ MAP, ↓ vasopressor requirements, ↓ cytokine levels, ↑ central venous oxygen saturation, ↓ in lactate, ↑ renal-failure free days Stress dose steroids: ↑ hospital discharge 8/27 (30%) vs. 0/15 (0%) p=0.02 ↑ organ failure free days 2 Statistics Results Authors’ Conclusions Critique VSE during resuscitation and stress-dose HCT in post-resuscitation shock improves survival by a factor of 4.5 in refractory IHCA Examined IHCA, did not exclude trauma patients Examined physiologic endpoints potentially associated with improvements in survival Predominantly asystole patients (75-80%) More reversible causes of CA in study group Use of multiple interventions; unclear if individual interventions are beneficial Used a previously unstudied dose of VASO Administered EPI and VASO every 2-3 minutes vs. 3-5 minutes Feasibility of administering VASO and EPI at the same time when not prepared ahead of time by study personnel C. Bottom line i. Combination VSE demonstrates improvement in ROSC and survival to hospital discharge compared to EPI alone ii. Benefits in ROSC likely from EPI + VASO iii. Benefits in survival likely from methylprednisolone iv. Neurologically favorable survival not demonstrated in this study H. Davis | Page 14 D. Efficacy data5 Table 6. Mentzelopoulos S, Malachias S, Charnos C, et al. Vasopressin, steroids, and epinephrine and neurologically favorable survival after in-hospital cardiac arrest: a randomized clinical trial. JAMA. 2013;310:270-279. Determine if combination VSE improves outcomes compared to standard of care for IHCA Objective Prospective, multi-centered, double blind, placebo-controlled, parallel-group, randomized controlled trial Study Design Intervention Methylprednisolone 40 mg x 1 EPI 1 mg + VASO 20 units (per resuscitation cycle) Following ROSC, HCT 300 mg/day continuous infusion x 3-7 days followed by taper, if postresuscitation shock present Control Placebo x 1 EPI 1 mg + placebo (per resuscitation cycle) Following ROSC, placebo x 3-7 days followed by taper, if post-resuscitation shock present Post-resuscitation shock – sustained > 4 hours, MAP ≤ 70 mmHg despite appropriate fluid resuscitation, or doubling of peri-arrest vasopressor requirements Patients Inclusion: IHCA, requiring EPI Exclusion: pediatric, terminally ill, do not resuscitate orders, arrests due to exsanguination, current treatment with steroids ITT analysis Kolmogorov-Smirnov for normality Dichotomous variables: 2-sided χ , Fishers exact test Continuous variables: 2-sided t test, Mann-Whitney exact U test Bonferroni correction Linear mixed model analysis to determine effect of groups Logistical regression for ORs with 95% Cis Multivariable Cox regression for HRs with 95% CIs VSE: n=268 ↑ ROSC: 109/130 (84%) vs. 91/138 (66%) p=0.005 ↑ discharge with CPC score 1 or 2: 18/130 (14%) vs. 7/138 (5%) p=0.02 ↓ duration ACLS, ↓ total EPI dose, ↑ hemodynamics, ↑ central venous oxygen saturation, ↑ cerebral perfusion pressure, ↑ renal-, neurologic-, ventilator-failure free days, ↓ organ dysfunction, similar adverse effects Stress dose steroids: ↑ discharge with CPC score of 1 or 2: 16/76 (21%) vs. 6/73 (8%) p=0.02 15 EPI patients received HCT, ↑ circulatory-, renal-, hepatic-, coagulation-, respiratory-failure free days No difference in incidence of adverse effects due to steroids VSE and stress-dose HCT vs. EPI results in ↑ survival to hospital discharge with favorable neurologic outcomes Post-arrest HCT may decrease poor outcomes, but requires further investigation Examined IHCA, large sample, did not exclude all trauma patients CPR quality assessed with diastolic blood pressures Utilized CPC score to evaluate neurologically favorable survival Detailed protocol for treatment of underlying conditions, therapeutic hypothermia, sedation/analgesia, etc Predominantly asystolic medicine patients Chest compression cycles lasted approximately 3-4 minutes Frequent use of atropine and bicarbonate 2 Statistics Results Authors’ Conclusions Critique E. Bottom line i. VSE increases ROSC and neurologically favorable survival a. ROSC, number needed to treat (NNT)= 6 b. Neurologically favorable survival, NNT = 12 ii. Overall reduction in EPI doses, length of ACLS, improved peri-arrest hemodynamics and perfusion which results in improved long-term outcomes iii. No increase in complications from steroids iv. Medications administered approximately every 3-4 minutes H. Davis | Page 15 VII. Summary of evidence A. Majority of studies are in OHCA vs. IHCA of non-traumatic origin and are powered for detecting differences in hospital admission B. Many variables throughout studies over the years i. Time to initiation of BLS/ACLS ii. Variation in protocols of emergency responders iii. Unknown quality of chest compressions and approach to ventilatory support iv. Change in availability of AEDs and defibrillators v. Change in standard medications and doses C. Many of the principles of therapy are based on data from previously healthy animals D. Prior to VSE, no ACLS medication or combination of medications has improved survival to discharge or neurologically favorable survival E. VSE demonstrated neurologically favorable survival VIII.Conclusions A. Addition of methylprednisolone complements EPI + VASO in improving ROSC rates i. Improves hemodynamic stability ii. Decreases ischemia/reperfusion injury iii. Reduces end-organ damage B. Improves neurologic outcomes and overall survival in IHCA requiring vasopressors IX. Recommendations A. IHCA i. Administer methylprednisolone 40 mg IV x 1 during first compression cycle requiring medications ii. Alternate every compression cycle (2 minutes) between a. EPI 1 mg IV every 4 minutes b. VASO 20 units IV every 4 minutes 1. Maximum of 5 doses iii. Continue standard use of other adjunctive treatments during ACLS when indicated based on clinical scenario B. If ROSC is obtained, observe for post-resuscitation shock i. At minimum maintain a MAP of ≥ 65 mmHg consider goals of ≥ 75 mmHg a. After appropriate volume resuscitation b. After appropriate vasopressors are initiated i. If norepinephrine requirements ≥ 0.2-0.5 mcg/kg/min, consider additional stress dose steroids ii. Avoid inotropes H. Davis | Page 16 Appendices Appendix A. “H’s & T’s” of Cardiac Arrest8 Cause Indications Treatment Hypoxia Distributive shock Anaphylactic shock Hemorrhagic shock ↓ oxygen saturation, cyanosis, PEA Hydrogen ion (acidosis) ↓ pH, ↓ CO2 Hypokalemia ↓ K ↓ Mg EKG progressing from peaked T waves to absent P waves to prolonged PR and QRS to sine-wave prior to loss of pulse Crystalloids Crystalloids, EPI, H1RA, H2RA, steroids Blood products Oxygen Sodium bicarbonate Treat underlying condition K , Mg replacement Shift K : Calcium, insulin, dextrose Sodium bicarbonate Prevent additional heat loss Rewarm Hypovolemia Hyperkalemia + Hypothermia Tension pneumothorax Cardiac tamponade Toxins Thrombosis (pulmonary) Thrombosis (cardiac) ++ Core temp ≤ 30°C Tracheal deviation away from tension, tachycardia, tachypnea, hypoxia resulting in CA associated with PEA ↓ ventricular filling and cardiac output causing hypotension and ultimately CA Toxidrome presentations, patient history, UDS or other laboratory indicators Tachycardia, tachypnea prior to arrest, right heart strain, PEA with rapid/narrow QRS, evidence of DVT Chest pain, diaphoretic, EKG findings prior to arrest, troponin elevation, cardiac history + ++ + Needle decompression initially Chest tube for definitive management Pericardiocentesis – needle aspiration Pericardial window –hole in pericardium CCB/β blockers: calcium, glucagon, high dose insulin/D50, fat emulsions Digoxin: antidigoxin Fab antibodies Cyanide: hydroxocobalamine or sodium nitrite/sodium thiosulfate Local anesthetics: fat emulsion Fibrinolytics and prolonged chest compressions Early coronary revascularization Fibrinolytics as a less favorable alternative Appendix B. Guideline Concordant ACLS Medication Dosing8 Medication Dose Indication Epinephrine 1 mg every 3-5 minutes Vasopressin 40 units x 1 All rhythms To replace the 1 or 2 dose of epinephrine per AHA guidelines All rhythms st nd 1 dose: 300 mg x 1 st Amiodarone After 3-5 minutes 2 dose: 150 mg x 1 After 3-5 minutes Per ERC guidelines: 900 mg IV drip over 24 hours nd Refractory VFib or VTach All medications may be administered by IV or IO routes H. Davis | Page 17 Appendix C. Cerebral-preformance Category5,61 CPC Indicates 1 Conscious with normal function or only slight disability 2 Conscious with moderate disability 3 Conscious with severe disability 4 5 Comatose or in a vegetative state Brain-dead or dead References 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. 11. 12. 13. 14. 15. 16. 17. 18. 19. Guyette F, Guimond G, Hostler D, et al. Vasopressin administered with epinephrine is associated with a return of a pulse in out-of-hospital cardiac arrest. Resuscitation. 2004;63:277-82. Sandroni C, Nolan J, Cavallaro F, et al. In-hospital cardiac arrest: incidence, prognosis, and possible measures to improve survival. Intensive Care Med, 2007;33:237-45. Moulaert V, Verbunt J, vanHeugten C, et al. Cognitive impairments in survivors of out-of-hospital cardiac arrest: a systematic review. Resuscitation. 2009;80:297-305. Stiell I, Wells G, Field B, et al. Advanced cardiac life support in out-of-hospital cardiac arrest. N Engl J Med. 2004;351(7):647-56. Mentzelopoulos S, Malachias S, Chamos C, et al. Vasopressin, steroids, and epinephrine and neurologically favorable survival after in-hospital cardiac arrest: a randomized clinical trial. JAMA. 2013;310(3):270-9. Laurent I, Monchi M, Chiche J, et al. Reversible myocardial dysfunction in survivors of out-of-hospital cardiac arrest. J Am Coll Cardiol. 2002;40(12):2110-16. Ruiz-Bailen M, Aguayo de Hoyos E, Ruiz-Navarro S, et al. Reversible myocardial dysfunction after cardiopulmonary resuscitation. Resuscitation. 2005;66:175-81. Neumar R, Otto C, Link M, et al. Adult advanced cardiovascular life support: 2010 American Heart Association guidelines for cardiopulmonary resuscitation and emergency cardiovascular care. Circulation. 2010;122:729-67. Vanden Hoek T, Morrison L, Shuster M, et al. Cardiac arrest in special situations: 2010 American Heart Association guidelines for cardiopulmonary resuscitation and emergency cardiovascular care. Circulation. 2010;122:829-61. Linder K, Haak T, Keller A, et al. Release of endogenous vasopressors during and after cardiopulmonary resuscitation. Heart. 1996;75:145-50. Varvarousi G, Stefaniotou A, Varavaroussis D, et al. Glucocorticoids as an emergency pharmacologic agent for cardiopulmonary resuscitation. Cardiovasc Drugs Ther. 2014;28:477-88. Nolan J, Soar J, Zideman D, et al. European Resuscitation Council guidelines for resuscitation 2010. Resuscitation. 2010;81:1219-444. Sunde K, Steen P. The use of vasopressor agents during cardiopulmonary resuscitation. Crit Care Clin. 2012;28:189-98. Olasveengen T, Sunde K, Brunborg C, et al. Intravenous drug administration during out-of-hospital cardiac arrest. JAMA. 2009;302(20):2222-29. Hubble M, Johnson C, Blackwelder J, et al. Probability of return of spontaneous circulation as a function of timing of vasopressor administration in out-of-hospital cardiac arrest. Prehosp Emerg Car. 2015; 1-7. Crile G, Dolley D. An experimental research into the resuscitation of dogs killed by anesthetics and asphyxia. J Exp Med. 1906;8:713-25. Epinephrine. Clinical Pharmacology. http://www.clinicalpharmacologyip.com/Forms/Monograph/monograph.aspx?cpnum=223&sec=monmech&t=0. July 14, 2015. Accessed: August 25, 2015. Ditchey R, Lindenfeld J. Failure of epinephrine to improve the balance between myocardial oxygen supply and demand during closed-chest resuscitation in dogs. Circulation. 1988;78:382-9. Dumas F, Bougouin W, Geri G, et al. Is epinephrine during cardiac arrest associated with worse outcomes in resuscitated patients? J Am Coll Cardiol. 2014;64(22):2360-7. H. Davis | Page 18 20. Ristagno G, Tang W, Huang L, et al. Epinephrine reduces cerebral perfusion during cardiopulmonary resuscitation. Crit Care Med. 2009;37(4)1408-15. 21. Niemann J, Haynes K, Garner D, et al. Postcountershock pulseless rhythms: response to CPR, artificial cardiac pacing, and adrenergic agonists. Ann Emerg Med. 1986;15(2):112-20. 22. Tang W, Weil M, Sun S, et al. Epinephrine increases the severity of postresuscitation myocardial dysfunction. Circulation. 1995; 92:3089-93. 23. Prengel A, Linder K, Ensinger H, et al. Plasma catecholamine concentrations after successful resuscitation in patients. Crit Care Med. 1992;20:609-14. 24. Ristagno G, Sun S, Tang W, et al. Effects of epinephrine and vasopressin on cerebral microcirculatory flows during and after cardiopulmonary resuscitation. Crit Care Med. 2007;35(9):2145-9. 25. Woodhouse S, Cox S, Boyd C, et al. High dose and standard dose adrenaline do not alter survival compared with placebo, in cardiac arrest. Resuscitation. 1995;30:243-9. 26. Herlitz J, Ekstrom L, Wennerblom B, et al. Adrenaline in out-of-hospital ventricular fibrillation, does it make any difference? Resuscitation. 1995;29:195-201. 27. Ong M, Tiah L, Leong B, et al. A randomized, double-blind, multi-center trial comparing vasopressin and adrenaline in patients with cardiac arrest presenting to or in the emergency department. Resuscitation. 2012;83:953-60. 28. Jacobs I, Finn J, Jelinek G, et al. Effect of adrenaline on survival in out-of-hospital cardiac arrest: a randomized double-blind placebo-controlled trial. Resuscitation. 2011;82:1138-43. 29. Vandycke C, Martens P. High dose versus standard dose epinephrine in cardiac arrest- a meta-analysis. Resuscitation. 2000;45(3):161-6. 30. Holmberg M, Holmberg S, Herlitz J. Low chance of survival among patients requiring adrenaline or intubation after out-of-hospital cardiac arrest in Sweden. Resuscitation. 2002;54(1):37-45. 31. Morris D, Dereczyk B, Gryzybowski M, et al. Vasopressin can increase coronary perfusion pressure during human cardiopulmonary resuscitation. Acad Emerg Med. 1997;4(9):878-83. 32. Mally S, Jelatancev A, Grmec S. Effects of epinephrine and vasopressin on end-tidal carbon dioxide tension and mean arterial blood pressure in out-of-hospital cardiopulmonary resuscitation: an observational study. Crit Care Med. 2006;11:1-8. 33. Kornberer E, Prengel A, Krismer A, et al. Vasopressin-mediated adrenocorticotropin release increases plasma cortisol concentrations during cardiopulmonary resuscitation. Crit Care Med. 2000;28(10):3517-21. 34. Larabee T, Liu K, Campbell J, et al. Vasopressors in cardiac arrest: a systematic review. Resuscitation. 2012;83:ndi932-9. 35. Linder K, Dirks B, Strohmenger H, et al. Randomized comparison of epinephrine and vasopressin in patients with out-of-hospital ventricular fibrillation. Lancet. 1997;349:535-7. 36. Stiell I, Hebert P, Wells G, et al. Vasopressin versus epinephrine for in-hospital cardiac arrest: a randomized controlled trial. Lancet. 2001;358:105-9. 37. Wenzel V, Krismer A, Arntz R, et al. A comparison of vasopressin and epinephrine for out-of-hospital cardiopulmonary resuscitation. N Engl J Med. 2004;350(2):105-13. 38. Grmec S, Mally S. Vasopressin improves outcomes in out-of-hospital cardiopulmonary resuscitation of ventricular fibrillation and pulseless ventricular tachycardia: a observational cohort study. Crit Care. 2006;10:1-7. 39. Gueugniaud P, David J, Chanzy E, et al. Vasopressin and epinephrine vs. epinephrine alone in cardiopulmonary resuscitation. New Engl J Med. 2008;359(1):21-30. 40. Turner D, Attridge R, Hughes D. Vasopressin associated with an increase in return of spontaneous circulation in acidotic cardiopulmonary arrest patients. Ann Pharmacother. 2014; 48(8):986-91. 41. Callaway C, Hostler D, Doshi A, et al. Usefulness of vasopressin administered with epinephrine during outof-hospital cardiac arrest. Am J Cardiol. 2006;98:1316-21. 42. Cody P, Lauderdale S, Hogan D, et al. Comparison of two protocols for pulseless cardiopulmonary arrest: vasopressin combined with epinephrine versus epinephrine alone. Prehosp Emerg Car. 2009;25(5):419-23. 43. Ducros L, Vicaut E, Soleil C, et al. Effect of the addition of vasopressin or vasopressin plus nitroglycerin to epinephrine on arterial blood pressure during cardiopulmonary resuscitation in humans. J Emerg Med. 2010;41(5):453-9. 44. Ong M, Tan E, Pen F, et al. Survival outcomes with the introduction of intravenous epinephrine in the management of out-of-hospital cardiac arrest. Ann Emerg Med. 2007;50(6):635-42. 45. Biondi-Zoccai G, Abbae A, Parisi Q, et al. Vasopressin superior to adrenaline or placebo in the management of cardiac arrest? A meta-analysis. Resuscitation. 2003;59:221-4. H. Davis | Page 19 46. Aung K, Htay T. Vasopressin for cardiac arrest. Arch Intern Med. 2005;165:17-24. 47. Mentzelopoulos S, Zakynthinos S, Siempos I, et al. Vasopressin for cardiac arrest: meta-analysis of randomized controlled trials. Resuscitation. 2012;83:32-9. 48. Layek A, Maitra S, Pal S, Bhattacharjee S, et al. Efficacy of vasopressin during cardio-pulmonary resuscitation in adult patients: a meta-analysis. Resuscitation. 2014;85:855-63. 49. Smithline H, Rivers E, Appleton T, et al. Corticosteroid supplementation during cardiac arrest in rats. Resuscitation. 1993;25:257-64. 50. Ito T, Saitoh D, Takasu A, et al. Serum cortisol as a predictive marker of the outcome in patients resuscitated after cardiopulmonary arrest. Resuscitation. 2004;62:55-60. 51. Wijdicks E, Hijdra A, Young G, et al. Quality standards subcommittee of the American Academy of Neurology. Practic parameter: prediction of outcome in comatose survivors after cardiopulmonary resuscitation (an evidence-based review): report of the quality standards subcommittee of the American Academy of Neurology. Neurology. 2006;67(2):203-10. 52. Tsai M, Huang C, Chang W, et al. The effect of hydrocortisone on the outcome of out-of-hospital cardiac arrest patients: a pilot study. Am J Emerg Med. 2007;25:318-25. 53. Tavakoli N, Bidari A, Vahdati S. Serum cortisol levels as a predictor of neuroloigic survival in successfully resuscitated victims of cardiopulmonary arrest. J Cardio Thor Res. 2012;4(4):107-11. 54. Adriel C, Adib-Conquy M, Laurent I, et al. Successful cardiopulmonary resuscitation after cardiac arrest as a “sepsis-like” syndrome. Circulation. 2002;106:562-68. 55. Menegazzi J, Ramos R, Wang H, et al. Post-resuscitation hemodynamics and relationship to the duration of ventricular fibrillation. Resuscitation. 2008;78:355-8. 56. Mayr V, Luckner G, Jochberger S, et al. Arginine vasopressin in advanced cardiovascular failure during the post-resuscitation phase after cardiac arrest. Resuscitation. 2007;72:35-44. 57. Jones A, Shapiro N, Kilgannon J, et al. Goal-directed hemodynamic optimization in the post-cardiac arrest syndrome: a systematic review. Resuscitation. 2008;77:2-29. 58. Bell D, Brindley P, Forrest D, et al. Management following resuscitation from cardiac arrest: recommendations from the 2003 Rocky Mountain Critical Care Conference. Can J Anesth. 2005;52(3):30922. 59. Pene F, Hyvernat H, Mallet V, et al. Prognostic value of relative adrenal insufficiency after out-of-hospital cardiac arrest. Intensive Care Med. 2005;31:627-33. 60. Rittenberger J, Doshi A, Reynolds J. Postcardiac arrest management. Emerg Med Clin N Am. 2015;33:691712. 61. Mentzelopoulos S, Zakynthinos S, Tzoufi M, et al. Vasopressin, epinephrine, and corticosteroids for inhospital cardiac arrest. Arch Intern Med. 2009;169:15-24. 62. Czock D, Keller F, Rasche F, et al. Pharmacokinetics and pharmacodynamics of systemically administered glucocorticoids. Clin Pharmacokinet. 2005;44(1):61-98. 63. White B. Pulseless idioventricular rhythm during CPR: an indication for massive intravenous bolus glucocorticoids. JACEP. 1976;5(6):449-54. 64. White B, Petinga T, Hoehner P, et al. Incidence, etiology, and outcome of pulseless idioventricular rhythm treated with dexamethasone during advanced CPR. JACEP. 1979;8(5):188-93. 65. Paris P, Stweart R, Deggler F. Prehospital use of dexamethasone in pulseless idioventricular rhythm. Ann Emerg Med. 1984;13(11):1008-10. 66. Grafton S, Longstreth W. Steroids after cardiac arrest: a retrospective study with concurrent nonrandomized controls. Neurology. 1988;38:1315-6. 67. Jastermski M, Sutton-Tyrrell K, Vaagenes P, et al. Glucocorticoid treatment does not improve neurological recovery following cardiac arrest. JAMA. 1989;262(24):3427-30. H. Davis | Page 20