Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
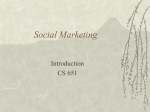
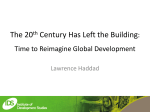
Pharmacist’s Role in Managing Special Patient Needs Related to Excipients Lindsay Snyder, PharmD, Pharmacy Practice resident, Blanchard Valley Medical Associates; Teresa Hoffman, PharmD, site preceptor; and Kelly Shields, PharmD, drug information specialist, ONU preceptor Objectives At the completion of this article, the reader should be able to: 1. Define inactive ingredients 2. Describe the purpose of inactive ingredients 3. Identify populations in which inactive ingredients are of concern 4. Recognize potential inactive ingredient problems in those populations 5. Formulate a plan to respond to inquiries about inactive ingredients Introduction Patients may not be aware of the role inactive ingredients play in the production of medications. Medication compounding or manufacture requires much more than just an active drug, other components or “inactive ingredients” serve multiple functions in the creation of effective dosage forms. Also named excipients, inactive ingredients may serve as coloring agents, fillers, diluents, preservatives, flavorings, sweeteners, solvents, lubricants, or vehicles. Such ingredients typically make up the majority of the mass or volume of a drug preparation, often five to ten times more than the mass of the active drug.1 Excipients are not only used in prescription drugs but also over-thecounter medications, vitamins, herbal products, or other dietary supplements. The FDA lists 10,437 inactive ingredients for human use as of 2008.2 Inactive ingredients are considered pharmacologically inert; however, they may pose problems to certain populations of patients. Types of patients who are especially vulnerable to the risks of inactive ingredients are patients with food allergies, pregnant women, children, or patients with medical dietary restrictions. These patient populations should avoid certain excipients for a myriad of different reasons. Possibly the most obvious reason is an allergy to an agent. Food allergies preclude the use of products containing derivatives of the allergen. Patients with drug allergies can have similar allergic reactions to certain dyes or sweeteners. Patients may be unable to use products containing alcohol due to pregnancy, previous ethanol abuse, or drug interactions. Medically necessary dietary restrictions such as gluten-free or ketogenic diets can also complicate medication selection. Religious sensitivities may also be taken into account because some common inactive ingredients may be animal-derived. It would seem that careful label reading would allow patients to avoid these excipients; however, problematic excipients may not be obviously stated on food or drug labeling. One common reason is that patients may not recognize the myriad of names under which a product may be listed. Also, substances used in manufacturing processes may not be listed as ingredients. Cross-contamination during production could possibly be an issue when multiple products are manufactured on the same line or in the same facility. Even though drug manufacturing confers less risk of cross-contamination than food manufacturing due to stringent regulations, cross-contamination can still be a significant risk for patients. Every pharmacist must be prepared to recognize and handle potential excipient problems because the pharmacist is typically the first person contacted for applicable information. Additionally, pharmacists are uniquely qualified to address these issues due to their training in pharmaceutics and their awareness of the variety of available dosage forms in which medications are available. This article provides a brief review of situations that may require excipient avoidance as well as corresponding management strategies. Food Allergies and Intolerances Food allergies or intolerances are an increasingly common complication in medication selection. Although reasons for the recent national rise in food allergies are poorly understood, more than 12 million Americans (about 4%) currently have food allergies.3 Though patients may not always recognize the difference, allergies and intolerances are classified based on the general mechanism of reaction. Figure 1 European Academy of Allergology and Clinical Immunology classification of adverse food reactions4 The majority of food allergies are IgE-mediated reactions.4 In 2003, the National Institutes of Health reported that 6-8% of children and 2% of adults had experienced IgE-mediated food allergy.5 The most common food allergens are listed in Table 1. Allergic reactions mediated by IgE are characterized by acute urticaria, atopic dermatitis, or anaphylactic symptoms.6 Reactions that begin minutes after allergen contact occur primarily through histamine release from basophils. Late phase reactions, beginning four to six hours later, can last for several days.4 Food allergies may also be immune-mediated without being solely due to IgE. Other antibody isotypes, immune complexes formed by the food and an antibody to the food, or cellmediated immune responses may be involved. For example, the autoimmune destruction of small intestine villi in response to gluten in celiac disease is T-cell mediated.6 Food intolerance, also called food sensitivity, may occur by several mechanisms including infections, enzyme abnormalities, or pharmacologic properties of foods. For example, an infection such as giardiasis may appear as intolerance to food. Lactose intolerance is caused by an abnormality of the lactase enzyme in the gastrointestinal tract. Pharmacologic food reactions can be caused by naturally occurring vasoactive amines such as histamine, dopamine, tyramine, phenylethylamine, serotonin, or norepinephrine. Reactions to vasoactive amines may manifest as paresthesias, burning sensation, headache, and/or pruritis.6 Table 1 Most Common IgE-mediated Food Allergens6 Children Adults Egg Shellfish Milk Tree nuts Soy Peanuts Wheat Fish Peanuts Food allergies and intolerances are often managed by strict avoidance of the allergen. Label reading becomes a significant component of food safety for these patients and also relates to drug safety. Detailed allergen labeling has become more common as labeling laws have become more stringent. The Food Allergen Labeling and Consumer Protection Act took effect on January 1, 2006, requiring the eight most common allergens (as listed in Table 1) to be disclosed in plain language on the label. These requirements apply even if the allergens are present in coloring, flavoring, or spices.7 The FDA continues to seek information from both manufacturers and consumers to improve allergen labeling.8 Ingredient nomenclature may make it difficult to identify ingredients that could pose a problem for food allergic patients. For example, if a patient is allergic to corn, and the label lists “starch” as an inactive ingredient, it may be overlooked by the patient as a potential source of allergenic corn protein. If label information is vague or the sources of ingredients are not listed, it may be necessary to contact the manufacturer for more information. Most companies will be able to provide some sort of allergen information, even if it is accompanied by a standard disclaimer statement. It is also important to obtain information about manufacturing processes and any substances used in production that are not listed as ingredients. Pregnancy and Pediatrics Although information on medication use during pregnancy is slowly accumulating, the fetal safety of inactive ingredients is largely unstudied. Some excipients are known to be problematic in pregnancy. Aluminum-containing aspirins and antacids pose a problem for pregnant women because aluminum is systemically absorbed, crosses the placenta, and can accumulate in the fetus. Aluminum has caused intoxication, neurologic symptoms, or osteopenia in newborns.1 The common inactive ingredients methylcellulose, polyethylene glycol (PEG), and polysorbate have undergone fetal safety testing in animals, but there is no conclusive human research for safety in pregnancy. A study of methylcellulose given to pregnant rats resulted in diaphragm abnormalities. Low molecular weight PEG compounds have caused congenital defects in mice and maternal toxicity in rabbits. Large molecular weight PEG (4000) has been studied for treatment of constipation in pregnant patients from 6-38 weeks gestation and appears to be safe. Polysorbate has been tested in numerous animal teratogenicity studies with mixed results. Using any of these products in pregnancy requires weighing the risks and benefits of treatment with the sparse available safety data.1 Benzyl alcohol is a preservative often used in parenteral products due to useful local anesthetic properties and poor palatability.9 Benzyl alcohol has been implicated in fatal “gasping syndrome” in premature neonates, characterized by hypotension, bradycardia, cardiovascular collapse, and metabolic acidosis. Gasping syndrome does not occur in infants older than 3 months, but hypersensitivity reactions including nausea, contact dermatitis, and angioedema can occur in older patients. Both the FDA and the American Academy of Pediatrics recommend against administering preparations preserved with benzyl alcohol to infants.10 Propylene glycol is a dihydroxy alcohol used as a pharmaceutical solvent, preservative, and humectant. Propylene glycol metabolism relies on alcohol and aldehyde dehydrogenase enzymes which may be inadequate for elimination in infants, children younger than 4, pregnant women, patients with renal or hepatic dysfunction, and patients taking disulfiram or metronidazole. These enzymes do not reach full capacity until children are 12 to 30 months old. Propylene glycol should be avoided in the above patient groups to prevent potential adverse effects such as hypotension, arrhythmia, or hemolysis.10 Ethanol, a known human teratogen and neurotoxin, is used in some liquid drug preparations. The ethanol threshold for fetal effects is unknown, but the small doses found in medications may be safe because of rapid maternal metabolism.1 Some elixir dosage formulations of medications for pediatric use may contain high concentrations of ethanol, for example Norvir® oral solution. Children are particularly affected by ethanol, with its well known adverse effects of CNS depression, confusion, and GI upset being more pronounced in children than other populations.10 Ethanol must also be avoided by those taking other medications that would cause a disulfiram-like reaction when combined with ethanol (ex. metronidazole). Patients with a history of alcohol abuse may also want minimize exposure to ethanol in medications.9 Religious Sensitivities Gelatin and stearic acid are commonly used inactive ingredients that are derived from animal sources. Specific sources of an excipient (ex. porcine, bovine) may vary from product to product, even from one lot to another. This may raise issues with patients because of religious beliefs. For example, consumption of pork products is forbidden in Judaism and Islam due to restrictions specified in the religious documents. Pork is also discouraged in some forms of Orthodox Christianity and in Seventh Day Adventist churches. Consumption of beef products can be controversial in Hinduism and Buddhism. Religious leaders are often responsible for determining what is acceptable for their individual religious groups, and they may make exceptions based on medical necessity. Patients are less likely to be adherent to medication regimens if they are concerned that they may contain religiously controversial ingredients.11 Pharmacists can help patients determine whether their medications are acceptable according to religious standards by obtaining more information on the source of the animal product. At times it may be difficult for even the manufacturing company to determine a source of gelatin or stearic acid, so alternative methods for dealing with religious sensitivities may be necessary. Because the inactive ingredients among similar drug products vary, another generic or brand name formulation that does not contain gelatin or stearic acid could be an alternative to the product in question. Many sustained release formulations contain gelatin, so switching a patient to appropriately timed immediate release preparations could solve the problem. Liquid preparations may be another alternative, as gelatin and stearic acid are primarily used in tablets or capsules. If other delivery systems such as transdermal patches or suppositories are available, they might also be appropriate choices. Depending on specific manufacturer recommendations, some drug powders could be removed from gelatin capsules before consumption. Because some religions also prohibit touching certain animal products, religious advisors may also need to be consulted before the powder from a gelatin capsule is consumed.11 Individually compounded preparations could be another potential solution, although this option may be too cost prohibitive for some patients. Celiac Disease Celiac disease is a genetically-linked autoimmune disorder that affects the small intestine in response to ingested gluten. Gluten proteins are found in wheat, barley, and rye. Although oats do not contain gluten peptides, they are often contaminated with gluten during growing and processing. It is controversial as to whether celiac patients can tolerate pure, uncontaminated oats, although certified gluten-free oats tested by ELISA assay have recently become available. Up to 1% of Americans may have celiac disease, but experts have estimated that 95% of cases are currently undiagnosed.12 Symptoms are often variable and can include malabsorption syndromes (ex. osteoporosis, iron-deficiency anemia), GI symptoms (bloating, diarrhea, constipation, abdominal pain, or dyspepsia), fatigue, depression, or dermatitis herpetiformis among many other symptoms. Diagnosis is often difficult due to variability in patient presentation, and celiac disease is frequently subject to misdiagnosis. Treatment is a strict gluten-free diet, which includes gluten-free medications.13 companies surveyed produced gluten-free products according to company policy. Many companies were hesitant to confirm the gluten status of their products in general, and some would only comment that no wheat, barley, rye, or oats were added to the product. Because many ingredient suppliers assessed in the survey did not guarantee gluten-free raw materials, some companies would not guarantee a gluten-free product without specific testing for the presence of gluten.14 Although food processing and preparation can lead to cross-contamination, it is unlikely to occur during the highly regulated drug manufacturing process.15 Ultimately, each company will place the responsibility of choosing a gluten-free product on the patient and physician even though the access to some information necessary for such decisions may be limited by the drug company. As the number of patients diagnosed with celiac disease increases, more patients will be requesting information about gluten-free medications. Some patients, while not diagnosed with celiac disease, may have a food intolerance to gluten and must also minimize or avoid gluten in food and medications. In addition to assistance with prescription and over the counter medications, pharmacists may play a role in helping this patient population by specifically identifying gluten-free vitamins and dietary supplements. Because of past or present malabsorption, celiac patients may wish to supplement iron, calcium, or other nutrients that could be deficient. Pharmacists can be a vital resource for selecting appropriate products. Gluten-containing excipients can be difficult to recognize. Excipients that could potentially contain gluten include starches, dextrates or dextrins, alcohols, caramel coloring, or barley-based brown rice syrup. These excipients can all be derived from gluten-free sources (ex. potato, rice, corn, or tapioca), but any such ingredient that does not list a glutenfree source on the label could potentially contain gluten. Many starch products made in the US come from gluten-free sources. For example, sodium starch glycolate manufactured in the US is usually derived from potato starch. It is important to consider, however, that some US drug companies may obtain ingredients from other countries. The ingredients of two common over-the-counter products are listed in Figure 2; the ingredients that might require more investigation to ensure the product is gluten-free are listed in bold type. Figure 2: Example Product Labels Tylenol® Tablets Active Ingredient: Acetaminophen 325 mg in each tablet Inactive Ingredients: Cellulose, corn starch, magnesium stearate, sodium starch glycolate. Motrin® IB Caplets Active Ingredient: Ibuprofen 200mg in each caplet Inactive Ingredients: carnauba wax, colloidal silicon dioxide, corn starch, FD&C yellow #6, hypromellose, iron oxide, magnesium stearate, polydextrose, polyethylene glycol, pregelatinized starch, propylene glycol, shellac, stearic acid, titanium dioxide As more people have been diagnosed with celiac disease, gluten information has become more available due to the need to assist these patients. In 2001, 5 of 100 pharmaceutical Ketogenic Diet The ketogenic diet is used as a treatment for patients with intractable seizure disorders, especially children. Although the exact anticonvulsant mechanism is unknown, this high lipid, low carbohydrate, and low protein diet in a 4:1 or 3:1 gram ratio leads to ketosis.16 Incomplete metabolism of fatty acids into ketone bodies produces acetone, acetoacetic acid, and α-hydroxybutyrate. Research into the anticonvulsive mechanism is ongoing, and it is hypothesized that the effect is not due to one single mechanism.17 Many patients take additional seizure medication along with the ketogenic diet. Since the diet is mostly used in children, and many of the children have swallowing difficulties, liquid medication preparations are frequently used. Carbohydrates from prescription medication can cause a problem because the total daily carbohydrate allowance for children 1-10 years on the ketogenic diet is 5-15 g. For example, one formulation of valproic acid syrup contains 20 grams of carbohydrates in a daily dose.16 Many excipients can contain other carbohydrates or proteins in addition to sugar–the more obvious culprit. It is important to remember that the words “sugar free” on the label does not mean that the product is free of carbohydrates. The most significant carbohydrate contributors are sucrose, fructose, sorbitol, glycerin, and alcohols, although the effect of ethyl alcohol on the ketogenic diet is unknown. Information about carbohydrate content may also be useful for patients with diabetes, metabolic disorders, alcohol intolerance, or gastrointestinal diseases. Table 2: Carbohydrate-containing Excipients Sweeteners Other sugars Misc. Sucrose, fructose, sorbitol, mannitol, xylitol, aspartame, saccharin, corn syrup Glucose, dextrose, lactulose Alcohols, glycerin, cellulose Planning ahead is essential to manage the carbohydrate contribution of medications to the allowed intake of the ketogenic diet. Include maintenance medication carbohydrates in the daily calculated carbohydrate totals. Plan for situations where additional medication might be quickly needed such as allergies, fever, or infection by knowing in advance which medications are available as low-carbohydrate formulations. If low carbohydrate formulations are not readily available, diet adjustments may be needed to allow for the carbohydrates from short-term medications.18 Sweetening agents can cause problem for additional patient populations. Sugar alcohols—sorbitol, mannitol, and xylitol— are commonly used as sweeteners in diabetic or lower-calorie foods. Medications containing large amounts of sugar alcohols may cause gas, bloating, or diarrhea. They are poorly absorbed in the gastrointestinal tract and are acted upon by colonic bacteria, causing osmotic diarrhea. Many oral liquid drug formulations use sorbitol as a vehicle and sweetener. Patients who receive large amounts of liquid medications, such as those receiving tube feedings, are at risk for sorbitol-induced diarrhea.19 Often, diarrhea associated with tube feeding is incorrectly blamed on the enteral solution itself when the medication formulations may be the true cause.20 Diarrhea can be a confusing symptom for patients with celiac disease or lactose intolerance because it can be a sign of gluten or lactose ingestion, respectively. If severe, diarrhea may preclude further use of sorbitol-containing medication, oftentimes on the assumption that the active drug itself is the cause. Switching to a formulation with no or less sorbitol may alleviate the diarrhea and allow the patient to continue taking the medication. Aspartame is a combination of L-aspartic acid and L-phenylalanine in methyl ester form. It is commonly found in food and drug products as a sweetener.9 It is 200 times sweeter than sugar, thus it contributes negligible caloric content if used in typical amounts. The FDA has determined that aspartame is safe based on review of more than 100 safety studies, although aspartame has had questionable links to cancer development.21 Aspartame is definitely risky, however, for patients with phenylketonuria (PKU) because it contains phenylalanine. PKU is a genetic disorder causing difficulty metabolizing phenylalanine, and phenylalanine can build up in the blood of PKU patients over time. Untreated PKU can cause growth failure, microcephaly, seizures and intellectual impairment from the accumulation of toxic metabolic by-products. The FDA requires PKU-specific labeling of all products containing aspartame to alert phenylketonurics to the presence of phenylalanine.21 Patients with sulfonamide allergies may also be sensitive to some sweeteners. Aspartame, as well as the sweetener saccharin, demonstrates cross-reactivity in patients allergic to sulfonamides. Caution is advised if sulfa-allergic patients take medications with these artificial sweeteners.28 Lactose Intolerance Lactose is a disaccharide also known as milk sugar. Lactose is found in dairy products and is also used as filler in many medications due to palatability and water solubility.22 Ingested lactose is broken down by lactase enzymes on the brush border of the small intestine. Lactose intolerance results from decreased activity or lack of lactase enzyme. When undigested lactose reaches the colon, it can cause symptoms such as bloating, flatulence, or diarrhea. Lactose intolerance is common, affecting between 30 and 50 million Americans.23 Treatment consists of either lactose avoidance or lactase enzyme supplementation. In a limited number of case reports, diarrhea has been reported after lactose-containing medications were started with an otherwise lactose-free diet.24 As an excipient in medications, the amount of lactose used is far smaller than that of standard portions of dairy products in the diet. Interestingly, in a randomized, double-blind, crossover study, self-identified severely lactose intolerant patients attributed GI symptoms to lactose even when lactose was not present in products they were receiving. Thirty patients, 21 of whom were determined by hydrogen breath tests to have lactose malabsorption, were given either 240mL of lactose-hydrolyzed or lactose-containing milk daily with breakfast for one week each. Minimal gastrointestinal symptoms were reported, and there were no significant differences in GI symptoms between the lactose and lactosehydrolyzed formulations.22 As this study demonstrates, it is difficult to definitively attribute GI symptoms to lactose ingestion as well as to identify individual thresholds for lactose intolerance. Whether the small amounts of lactose used as inactive ingredients cause symptoms of lactose intolerance is hard to determine; however, lactose in drug formulations continues to be a concern for many patients who are severely lactose intolerant. Allergies to Preservatives or Dyes Sulfiting agents are commonly used as preservatives due to their antioxidant and antimicrobial properties. Even though they are known to cause serious reactions, sulfites have generally regarded as safe (GRAS) status and are used in many foods and drugs. Reactions almost always occur with coexisting reactive airway disease and can manifest as asthma exacerbations or nonimmunologic anaphylactoid reactions.25 Contact dermatitis is also a common reaction from sulfites in topical products.26 In the course of food processing, sulfites may be added to salads, potatoes, dried fruits, beer, and wine among many other products.26 The FDA prohibits sulfite use on fruits or vegetables that are to be served or presented fresh to the public. They also require proper labeling of any food product with detectable sulfite levels, even if the sulfite is used as a processing aid.27 Sulfites may be added to drug products, often parenteral or topical formulations, and the medications must be labeled that they contain sulfites. For example some formulations of ketoconazole, parenteral chlorpromazine, chlorpheniramine, dopamine, and dexamethasone injections have added sulfites. Because sodium metabisulfite prevents the oxidation of epinephrine, it is often an ingredient in parenteral epinephrine formulations, local anesthetics, and sympathomimetic eye drops.26 Those who have a known sensitivity to sulfites should avoid medications that contain them, making an exception for injectable epinephrine in life-threatening anaphylactic situations.25 The parabens, other commonly used preservatives, may cause cross-reactivity in aspirin-sensitive patients and should be used with caution. The paraben metabolite hydroxyparabenzoic acid is structurally similar to aspirin, and anaphylactic reactions in aspirin-sensitive patients have been reported.29 Tartrazine (FD&C yellow no. 5) and sunset yellow (FD&C yellow no. 6) have demonstrated cross-reactivity with aspirin, sodium benzoate, indomethacin, and other azo dyes.28 Tartrazine can produce a reaction similar to aspirin intolerance including bronchospasm, urticaria, eosinophilia, or angioedema. Although rare, nonimmunologic anaphylactoid reactions have been reported. Between 2% and 20% of asthmatic individuals are aspirin-sensitive, and tartrazine has been shown to be particularly dangerous in aspirin-sensitive patients. Crossreactivity rates were once thought to be as high as 10%, but more recent research suggests less than 2.4% cross-reactivity.25 Sunset yellow (FD&C yellow no. 6) has been associated in case reports with gastrointestinal symptoms, with one case involving eosinophilia and hives. Aspirin-sensitive patients have also developed similar reactions to other dyes including amaranth, erythrosine, indigo carmine (FD&C blue no.2), ponceau, new coccine, brilliant blue (FD&C blue no. 1), methyl blue, quinoline yellow, and FD&C red no. 40. Dyes have also been purported to contribute to hyperactivity in children, but controlled trials have not shown such an association.25 Conclusion Many patient populations must be considered in a discussion of inactive ingredients, and there are more patient considerations than can be addressed in this article. It may be difficult to determine which drug products are appropriate in situations of excipient intolerance. The source with the most information is almost always the drug company itself. When calling a drug company, make sure to have in mind the questions that you would like to ask or the clarifications you would like to make before calling. It may be time-consuming to navigate automated answering systems, but having to call back usually means doing it all over again. Have the lot number of the drug handy, as inactive sources can vary from one lot to another. Most companies will provide information pertaining to a specific patient situation, but they may not guarantee that the information will apply to any future situations. Watch for clues to changes in inactives, such as “new formulation” notices on product label. Make sure to verify the status of the drug periodically, as the information is typically only accurate at the time of inquiry. If responses from drug companies are vague or seem like a legal disclaimer with little usable information, ask specific questions about the sources of individual inactive ingredients in a particular lot of drug. Usually, someone at the company can provide this information. In addition to contacting a drug company, pharmacists may be able to suggest therapeutic alternatives. Pharmacists can evaluate other dosage forms such as liquid medications, transdermal patches, a different generic or brand formulation, or switching from extended-release to immediate-release formulations. Compounded formulations may be an option if suitable dosage forms are not commercially available. When compounding, the pharmacist must also be aware of excipients in each ingredient involved in product preparation and realize that individualized drug formulations may be very costly to the patient. Sulfiting agents25 Sulfur dioxide Sodium sulfite Sodium bisulfite Sodium metabisulfite Potassium bisulfate Potassium metabisulfite Patients depend on their pharmacists—often their most accessible health care providers—to assist in making important decisions about medication suitability for their individual situations. Pharmacists are uniquely positioned to evaluate drug selection based on inactive ingredients. Understanding patient needs as well as being familiar with drug formulations, dosage forms, and sources of inactive ingredients make the pharmacist an invaluable resource.