Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
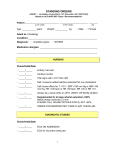
STANDING ORDERS ADMIT – Unstable Angina/Non–ST-Elevation MI (NSTEMI) ACC/AHA Class I Recommendations* in Bold Patient ___________________________ ______________________ _______ (LAST NAME) Age: ___________ years (FIRST NAME) Weight: __________ kg (MI) Male Female Admit to: Cardiology Condition:_______________________________________________________ Diagnosis: Unstable angina NSTEMI Check/Initial/Date _____/_____ Allergies: ________________________________________ ________________________________________________ _____/_____ EARLY RISK STRATIFICATION High risk Intermediate risk Low risk High risk: elevated cardiac biomarkers, ST depression, transient ST elevation, >20 min of rest pain, hemodynamic instability, signs of CHF → EARLY INVASIVE STRATEGY Intermediate risk: no high-risk features, prior MI, prior CABG, T-wave inversions, rest angina <20 min relieved promptly with nitroglycerin, age >70 years → EITHER EARLY INVASIVE OR EARLY CONSERVATIVE STRATEGY Low risk: No high- or moderate-risk features, progressive angina without prolonged rest pain, normal cardiac markers, normal ECG with pain → EARLY CONSERVATIVE STRATEGY ACC/AHA Class I A rapid clinical determination of the likelihood risk of Recommendation obstructive CAD (ie, high, intermediate, or low) should be made in all patients with chest discomfort or other symptoms suggestive of an ACS and considered in patient management [Level of Evidence: C]. Patients who present with chest discomfort or other ischemic symptoms should undergo early risk stratification for the risk of cardiovascular events (eg, death or [re]MI) that focuses on history, including anginal symptoms, physical findings, ECG findings, and biomarkers of cardiac injury, and results should be considered in patient management [Level of Evidence: C]. 1 STANDING ORDERS ADMIT – Unstable Angina/Non–ST-Elevation MI (NSTEMI) ACC/AHA Class I Recommendations* in Bold Check/Initial/Date NURSING _____/_____ Activity – Bed rest _____/_____ Cardiac monitor ACC/AHA Class I Bed/chair rest with continuous ECG monitoring is Recommendation recommended for all patients during the early hospital phase [Level of Evidence: C]. _____/_____ Vital signs q4h x 24 h then q8h _____/_____ Diet: house/no added salt/low saturated fat; low cholesterol _____/_____ Call house officer for T >101°, SBP >190 mm Hg or SBP <90 mm Hg, HR >120 bpm or HR <50 bpm, RR >30 or RR <10 _____/_____ Guaiac ALL stools while on heparin, LMWH, IIb/IIIa inhibitor _____/_____ O2: Nasal prongs (cannula) 2 L/min PLEASE CALL HOUSE OFFICER FOR O2 SAT <90% _____/_____ ORDER FOR RESPIRATORY CARE O2 SAT CHECK q8h ACC/AHA Class I Supplemental oxygen should be administered to Recommendation patients with an arterial saturation less than 90%, respiratory distress, or other high-risk features for hypoxemia [Level of Evidence: B]. 2 STANDING ORDERS ADMIT – Unstable Angina/Non–ST-Elevation MI (NSTEMI) ACC/AHA Class I Recommendations* in Bold Check/Initial/Date DIAGNOSTIC STUDIES _____/_____ ECG ON ADMISSION _____/_____ ECG for recurrent chest pain ACC/AHA Class I A 12-lead ECG should be performed and shown to an Recommendation experienced emergency physician as soon as possible after ED arrival, with a goal of within 10 min of ED arrival for all patients with chest discomfort (or anginal equivalent) or other symptoms suggestive of ACS. If the initial ECG is not diagnostic but the patient remains symptomatic and there is high clinical suspicion for ACS, serial ECGs, initially at 15- to 30-min intervals, should be performed to detect the potential for development of ST-segment elevation or depression [Level of Evidence: B]. LABORATORY STUDIES CARDIAC MARKERS _____/_____ Troponin T/Troponin I: NOW AND EVERY _____hrs × ___ times _____/_____ CK-MB: NOW AND EVERY _____ hrs × ___ times ACC/AHA Class I Cardiac biomarkers should be measured in all patients Recommendation who present with chest discomfort consistent with ACS. A cardiac-specific troponin is the preferred marker, and, if available, it should be measured in all patients who present with chest discomfort consistent with ACS. Patients with negative cardiac biomarkers within 6 h of the onset of symptoms consistent with ACS should have biomarkers remeasured in the time frame of 8 to 12 h after symptom onset. (The exact timing of serum marker measurement should take into account the uncertainties often present with the exact timing of onset of pain and the sensitivity, precision, and institutional norms of the assay being utilized as well as the release kinetics of the marker being measured.) [Level of Evidence: B]. CHEMISTRY PANEL _____/_____ CBC, LIPID PROFILE, PTT, Chemistry (7) panel IN AM – FASTING 3 STANDING ORDERS ADMIT – Unstable Angina/Non–ST-Elevation MI (NSTEMI) ACC/AHA Class I Recommendations* in Bold Check/Initial/Date MEDICATIONS _____/_____ ASPIRIN 162-325 (__________ insert dose) mg po chewed (loading dose) now, then 162-325 mg/d po (daily maintenance dose) ACC/AHA Class I Aspirin should be administered to patients as soon as Recommendation possible after hospital presentation and continued indefinitely in patients not known to be intolerant of that medication [Level of Evidence: A]. OR _____/_____ ACC/AHA Class I Recommendation _____/_____ CLOPIDOGREL 300 mg po x 1, then 75 mg/d po if aspirin intolerant Clopidogrel (loading dose followed by daily maintenance dose)† should be administered to patients who are unable to take ASA because of hypersensitivity or major GI intolerance [Level of Evidence: A]. Stop all NSAIDs except aspirin β-BLOCKER (choose one): IV β-BLOCKER _____/_____ Drug: _____________________________ every ____ hrs _______ mg IV ORAL β-BLOCKER _____/_____ METOPROLOL TARTRATE 50-200 mg bid _____/_____ ATENOLOL 50-200 mg/d _____/_____ CARVEDILOL 6.25 mg bid, uptitrated to max. 25 mg bid ACC/AHA Class I Oral β-blocker therapy should be initiated within the first Recommendation 24 h for patients who do not have ≥1 of the following: 1) signs of HF, 2) evidence of a low-output state, 3) increased risk‡ for cardiogenic shock, or 4) other relative contraindications to β-blockade (PR interval >0.24 s, second- or third-degree heart block, active asthma, or reactive airway disease) [Level of Evidence: B]. 4 STANDING ORDERS ADMIT – Unstable Angina/Non–ST-Elevation MI (NSTEMI) ACC/AHA Class I Recommendations* in Bold _____/_____ NITROGLYCERIN PASTE 2% Sliding Scale TP q4h. For SBP <100 mm Hg, remove nitropaste; for SBP 100-120 mm Hg, give 1” nitropaste; for SBP 121-140 mm Hg, give 2” nitropaste; for SBP >140 mm Hg, give 3” nitropaste _____/_____ NITROGLYCERIN 1/150 (0.4 mg) 1 TAB SL q5min x 3 prn chest pain; HOLD IF: SBP <100 mm Hg _____/_____ NITROGLYCERIN 5-200 µg/min IV in D5W continuous IV ACC/AHA Class I Patients with ongoing ischemic discomfort should Recommendation receive sublingual NTG (0.4 mg) every 5 min for a total of 3 doses, after which assessment should be made about the need for IV NTG, if not contraindicated. [Level of Evidence: C]. IV NTG is indicated in the first 48 h after UA/NSTEMI for treatment of persistent ischemia, HF, or hypertension. The decision to administer IV NTG and the dose used should not preclude therapy with other proven mortality-reducing interventions such as βblockers or ACE inhibitors [Level of Evidence: B]. 5 STANDING ORDERS ADMIT – Unstable Angina/Non–ST-Elevation MI (NSTEMI) ACC/AHA Class I Recommendations* in Bold EARLY INVASIVE STRATEGY (High- or Intermediate-Risk Patients) Check/Initial/Date _____/_____ CLOPIDOGREL 300-600 (__________ insert dose) mg po x 1, then 75 mg/d po (Add once decision to proceed with PCI is confirmed. Withhold for 5 days if CABG is planned.) ACC/AHA Class I In patients with a history of GI bleeding, when ASA and Recommendation clopidogrel are administered alone or in combination, drugs to minimize the risk of recurrent GI bleeding (eg, proton-pump inhibitors) should be prescribed concomitantly [Level of Evidence: B]. AND/OR _____/_____ GLYCOPROTEIN IIB/IIIA THERAPY (choose one [can be started upstream or in cardiac catheterization lab]): EPTIFIBATIDE 180 µg/kg IV bolus x 2, 10 min apart, followed by IV infusion of 2.0 µg/kg/min, reduce to 1.0 µg/kg/min if CrCl <50 mL/min OR _____/_____ TIROFIBAN IV infusion of 0.4 µg/kg/min for 30 min, reduce to 0.2 µg/kg/min for CrCl <30 mL/min, followed by IV infusion of 0.1 µg/kg/min, reduce to 0.05 µg/kg/min if CrCl <30 mL/min OR _____/_____ ABCIXIMAB 0.25 mg/kg IV bolus, followed by IV infusion of 0.125 µg/kg/min [reserve only for patients with planned PCI within 12 hours] ACC/AHA Class I For patients in whom an initial invasive strategy is Recommendation selected, antiplatelet therapy in addition to aspirin should be initiated before diagnostic angiography (upstream) with either clopidogrel (loading dose followed by daily maintenance dose)† or an IV GP IIb/IIIa inhibitor [Level of Evidence: A]. Abciximab as the choice for upstream GP IIb/IIIa therapy is indicated only if there is no appreciable delay to angiography and PCI is likely to be performed; otherwise, IV eptifibatide or tirofiban is the preferred choice of GP IIb/IIIa inhibitor [Level of Evidence: B]. 6 STANDING ORDERS ADMIT – Unstable Angina/Non–ST-Elevation MI (NSTEMI) ACC/AHA Class I Recommendations* in Bold EARLY INVASIVE STRATEGY (High- or Intermediate-Risk Patients) Continued Check/Initial/Date _____/_____ ANTICOAGULANT THERAPY (choose one): ENOXAPARIN 1 mg/kg SC q12h (if CrCl <30 mL/min, give 1 mg/kg every 24 h) [continue for the duration of hospitalization, 8 days, or until PCI or CABG is performed] OR _____/_____ UNFRACTIONATED HEPARIN (for 48 hours) 60 U/kg IV bolus (not to exceed 4000 U), followed by IV infusion of 12 U/kg/h (not to exceed 1000 U/h) to goal aPTT 50-70 sec; check aPTT in 6 h and adjust as indicated OR _____/_____ FONDAPARINUX 2.5 mg SC once daily (avoid if CrCl <30 mL/min [continue for the duration of hospitalization, 8 days, or until PCI or CABG is performed]). UFH, per institutional practice, should be administered for any PCI procedure OR _____/_____ BIVALIRUDIN 0.1 mg/kg IV bolus, then IV infusion of 0.25 mg/kg/h [continue for the duration of hospitalization, 8 days, or until PCI or CABG is performed] ACC/AHA Class I Anticoagulant therapy should be added to antiplatelet Recommendation therapy as soon as possible after presentation. For patients in whom an invasive strategy is selected, regimens with established efficacy at a Level of Evidence: A include enoxaparin and UFH, and those with established efficacy at a Level of Evidence: B include bivalirudin and fondaparinux. 7 STANDING ORDERS ADMIT – Unstable Angina/Non–ST-Elevation MI (NSTEMI) ACC/AHA Class I Recommendations* in Bold EARLY CONSERVATIVE STRATEGY (Low- or Intermediate-Risk Patients) Check/Initial/Date _____/_____ CLOPIDOGREL 300-600 (__________ insert dose) mg po x 1, then 75 mg/d po ACC/AHA Class I For patients in whom an initial conservative (ie, Recommendation noninvasive) strategy is selected, clopidogrel (loading dose followed by daily maintenance dose)† should be added to ASA and anticoagulant therapy as soon as possible after admission and administered for at least 1 month [Level of Evidence: A] and ideally up to 1 year [Level of Evidence: B]. In patients with a history of GI bleeding, when ASA and clopidogrel are administered alone or in combination, drugs to minimize the risk of recurrent GI bleeding (eg, proton-pump inhibitors) should be prescribed concomitantly [Level of Evidence: B]. ANTICOAGULANT THERAPY (choose one): _____/_____ ENOXAPARIN 1 mg/kg SC q12h (if CrCl <30 mL/min, give 1 mg/kg every 24 h) [continue for the duration of hospitalization, 8 days, or until PCI] OR _____/_____ UNFRACTIONATED HEPARIN (for 48 hours) 60 U/kg IV bolus (not to exceed 4000 U), followed by IV infusion of 12 U/kg/h (not to exceed 1000 U/h) to goal aPTT 50-70 sec; check aPTT in 6 h and adjust as indicated OR _____/_____ FONDAPARINUX 2.5 mg SC once daily (avoid if CrCl <30 mL/min [continue for the duration of hospitalization, 8 days, or until PCI]). UFH, per institutional practice, should be administered for any PCI procedure ACC/AHA Class I Anticoagulant therapy should be added to antiplatelet Recommendation therapy as soon as possible after presentation. For patients in whom a conservative strategy is selected, regimens using either enoxaparin§ or UFH [Level of Evidence: A] or fondaparinux [Level of Evidence: B] have established efficacy. In patients in whom a conservative strategy is selected and who have an increased risk of bleeding, fondaparinux is preferable [Level of Evidence: B]. 8 STANDING ORDERS ADMIT – Unstable Angina/Non–ST-Elevation MI (NSTEMI) ACC/AHA Class I Recommendations* in Bold EARLY CONSERVATIVE STRATEGY (Low- or Intermediate-Risk Patients) Continued Check/Initial/Date _____/_____ Schedule assessment of LVEF _____/_____ Schedule stress test ACC/AHA Class I For patients in whom an initial conservative strategy is Recommendation selected and no subsequent features appear that would necessitate diagnostic angiography (recurrent symptoms/ischemia, HF, or serious arrhythmias), a stress test should be performed [Level of Evidence: B]. _____/_____ _____/_____ Start early invasive strategy if patient has recurrent symptoms/ischemia, HF, arrhythmias, or positive cardiac biomarkers GLYCOPROTEIN IIB/IIIA THERAPY EPTIFIBATIDE 180 µg/kg IV bolus x 2, 10 min apart, followed by IV infusion of 2.0 µg/kg/min, reduce to 1.0 µg/kg/min if CrCl <50 mL/min OR _____/_____ TIROFIBAN IV infusion of 0.4 µg/kg/min for 30 min, reduce to 0.2 µg/kg/min for CrCl <30 mL/min, followed by IV infusion of 0.1 µg/kg/min, reduce to 0.05 µg/kg/min if CrCl <30 mL/min ACC/AHA Class I For patients in whom an initial conservative strategy is Recommendation selected, if recurrent symptoms/ischemia, HF, or serious arrhythmias subsequently appear, then diagnostic angiography should be performed. Either an IV GP IIb/IIIa inhibitor (eptifibatide or tirofiban) or clopidogrel (loading dose followed by daily maintenance dose)† [Level of Evidence: A] should be added to ASA and anticoagulant therapy before diagnostic angiography (upstream) [Level of Evidence: C]. 9 STANDING ORDERS ADMIT – Unstable Angina/Non–ST-Elevation MI (NSTEMI) ACC/AHA Class I Recommendations* in Bold Check/Initial/Date AS-NEEDED MEDICATIONS _____/_____ Colace 100 mg po bid _____/_____ MAALOX PLUS EX STR 15 mL po q6h prn indigestion _____/_____ OXAZEPAM 15-30 mg po qhs prn insomnia _____/_____ ACETAMINOPHEN 650 mg po q4h prn headache _____/_____ MAGNESIUM HYDROXIDE 30 mL po qd prn constipation _____/_____ MAGNESIUM SULFATE Sliding Scale IV qd Call house officer if serum Mg <1.2 Hold order for creatinine >1.9 If serum Mg <1.4 give 5 g MgSO4 IV If serum Mg <1.6 give 4 g MgSO4 IV If serum Mg <1.8 give 3 g MgSO4 IV If serum Mg <2.0 give 2 g MgSO4 IV _____/_____ LAB, MG, K qd _____/_____ KCL IMMEDIATE REL Sliding Scale Target K >4.5 po qd Call house officer if K <3.4 If K <3.7 give 60 mEq If K <4.1 give 40 mEq If K <4.6 give 20 mEq _____/_____ CHEST PAIN PROTOCOL _____/_____ ECG x 1 prn chest pain _____/_____ For CP: check VS, call house officer _____/_____ Mark if cardiac cath is planned: Time _________________ _____/_____ NPO except meds _____/_____ LAB, TYPE AND HOLD NEXT AVAILABLE _____/_____ NUTRITION CONSULT Patient admitted to cardiology ischemia pathway with known or suspected CAD. Please facilitate outpatient education in low-cholesterol, low-salt diet _____/_____ SOCIAL SERVICE CONSULT Patient admitted to cardiology ischemia pathway with known or suspected CAD. Please assess and assist in need for outpatient support (including VNA) services 10 Now After midnight STANDING ORDERS ADMIT – Unstable Angina/Non–ST-Elevation MI (NSTEMI) ACC/AHA Class I Recommendations* in Bold Check/Initial/Date DAY 2 or Later: REMINDERS _____/_____ Calcium channel blocker (if β-blocker contraindicated) Drug: _______________________ ___mg ____times/d ACC/AHA Class I In patients with continuing or frequently recurring Recommendation ischemia and in whom β-blockers are contraindicated, a nondihydropyridine calcium channel blocker (eg, verapamil or diltiazem) should be given as initial therapy in the absence of clinically significant LV dysfunction or other contraindications [Level of Evidence: B]. _____/_____ ACE inhibitor or ARB; recommended if diabetic Drug: _______________________ ___mg ____times/d ACC/AHA Class I An ACE inhibitor should be administered orally within Recommendation the first 24 h to patients with pulmonary congestion or LVEF ≤0.40, in the absence of hypotension (SBP <100 mm Hg or <30 mm Hg below baseline) or known contraindications to that class of medications. An ARB should be administered to patients who are intolerant of ACE inhibitors and have either clinical or radiologic signs of HF or LVEF ≤0.40 [Level of Evidence: A]. _____/_____ Lipid-lowering therapy (statins) regardless of LDL; dose target to LDL <100 mg/dL Drug: ____________________________ ___mg once daily ACC/AHA Class I Hydroxymethyl glutaryl-coenzyme A reductase Recommendation inhibitors (statins), in the absence of contraindications, regardless of baseline LDL-C and diet modification, should be given to post-UA/NSTEMI patients, including postrevascularization patients. For patients with elevated LDL-C (≥100 mg/dL), cholesterol-lowering therapy should be initiated or intensified to achieve an LDL-C <100 mg/dL [Level of Evidence: A]. _____/_____ Echocardiography. FIRST 24 HR if evidence of CHF, hemodynamic instability, mechanical complication _____/_____ Warfarin: RECOMMENDED if LV thrombus, extensive wall dyskinesis, LVEF <20%-30% 11 STANDING ORDERS ADMIT – Unstable Angina/Non–ST-Elevation MI (NSTEMI) ACC/AHA Class I Recommendations* in Bold Check/Initial/Date PRIOR TO DISCHARGE _____/_____ _____/_____ Patient had stent implanted OR Patient had medical therapy without stenting MEDICATIONS _____/_____ Aspirin ________ mg/d for _________________________ ________________________________________________ ACC/AHA Class I For patients treated medically without stenting, aspirin Recommendation (75 to 162 mg/d) should be prescribed indefinitely [Level of Evidence: A]. For patients treated with bare-metal stents, aspirin 162 to 325 mg/d should be prescribed for at least 1 month [Level of Evidence: B], then continued indefinitely at a dose of 75 to 162 mg/d [Level of Evidence: A]. For patients treated with DES, aspirin 162 to 325 mg/d should be prescribed for at least 3 months after sirolimus-eluting stent implantation and 6 months after paclitaxel-eluting stent implantation, then continued indefinitely at a dose of 75 to 162 mg/d [Level of Evidence: B] _____/_____ Clopidogrel 75 mg/d for ____________________________ _______________________________________________ ACC/AHA Class I For patients treated medically without stenting, Recommendation clopidogrel (75 mg/d) should be prescribed for at least 1 month [Level of Evidence: A] and ideally for up to 1 year [Level of Evidence: B]. For patients treated with bare-metal stents, clopidogrel should be prescribed at a dose of 75 mg/d for a minimum of 1 month and ideally up to 1 year (unless the patient is at increased risk of bleeding; then it should be given for a minimum of 2 weeks [Level of Evidence: B]. For patients treated with DES, clopidogrel 75 mg/d should be given for at least 12 months to all post-PCI patients receiving DES [Level of Evidence: B]. 12 STANDING ORDERS ADMIT – Unstable Angina/Non–ST-Elevation MI (NSTEMI) ACC/AHA Class I Recommendations* in Bold Check/Initial/Date PRIOR TO DISCHARGE (Continued) MEDICATIONS (Continued) _____/_____ β-blocker Drug: _______________________________________ Dosage: _____________________________________ ACC/AHA Class I β-blockers are indicated for all patients recovering from Recommendation UA/NSTEMI unless contraindicated. Treatment should begin within a few days of the event, if not initiated acutely, and should be continued indefinitely [Level of Evidence: B]. _____/_____ ACE inhibitor or ARB Drug: _______________________________________ Dosage: _____________________________________ _____/_____ Aldosterone receptor blocker Drug: _______________________________________ Dosage: _____________________________________ ACC/AHA Class I Angiotensin-converting enzyme inhibitors should be Recommendation given and continued indefinitely for patients recovering from UA/NSTEMI with HF, LV dysfunction (LVEF <0.40), hypertension, or diabetes mellitus, unless contraindicated [Level of Evidence: A]. An angiotensin receptor blocker should be prescribed at discharge to those UA/NSTEMI patients who are intolerant of an ACE inhibitor and who have either clinical or radiological signs of HF and LVEF <0.40 [Level of Evidence: A]. Long-term aldosterone receptor blockade should be prescribed for UA/NSTEMI patients without significant renal dysfunction (estimated creatinine clearance should be >30 mL/min) or hyperkalemia (potassium should be ≤5 mEq/L) who are already receiving therapeutic doses of an ACE inhibitor, have an LVEF ≤0.40, and have either symptomatic HF or diabetes mellitus [Level of Evidence: A]. 13 STANDING ORDERS ADMIT – Unstable Angina/Non–ST-Elevation MI (NSTEMI) ACC/AHA Class I Recommendations* in Bold Check/Initial/Date PRIOR TO DISCHARGE (Continued) MEDICATIONS (Continued) _____/_____ Calcium channel blocker Drug: ________________________________________ Dosage: ______________________________________ ACC/AHA Class I Calcium channel blockers are recommended for Recommendation ischemic symptoms when β-blockers are not successful [Level of Evidence: B]. Calcium channel blockers are recommended for ischemic symptoms when β-blockers are contraindicated or cause unacceptable side effects [Level of Evidence: C]. _____/_____ Statin Drug: ________________________________________ Dosage: ______________________________________ ACC/AHA Class I For hospitalized patients, lipid-lowering medications Recommendation should be initiated before discharge [Level of Evidence: A]. _____/_____ Nitroglycerin Drug: ________________________________________ Dosage: ______________________________________ ACC/AHA Class I Nitroglycerin to treat ischemic symptoms is Recommendation recommended [Level of Evidence: C]. 14 STANDING ORDERS ADMIT – Unstable Angina/Non–ST-Elevation MI (NSTEMI) ACC/AHA Class I Recommendations* in Bold Check/Initial/Date PRIOR TO DISCHARGE (Continued) PATIENT/FAMILY EDUCATION AND FOLLOW-UP INSTRUCTIONS _____/_____ Medication instructions/disease education _____/_____ Smoking cessation _____/_____ Diabetes management _____/_____ Nutrition, weight, and blood pressure management _____/_____ Exercise program ACC/AHA Class I Before hospital discharge, patients and/or designated Recommendation responsible caregivers should be provided with supportable, easily understood, and culturally sensitive instructions with respect to medication type, purpose, dose, frequency, and pertinent side effects. If the pattern or severity of anginal symptoms changes, which suggests worsening myocardial ischemia (eg, pain is more frequent or severe or is precipitated by less effort or now occurs at rest), the patient should contact his or her physician without delay to assess the need for additional treatment or testing [Level of Evidence: C]. Specific instruction should be given on the following: smoking cessation and achievement of optimal weight, daily exercise, and diet [Level of Evidence: B]; hypertension control to a blood pressure <140/90 mm Hg or <130/80 mm Hg in patients with diabetes or chronic kidney disease [Level of Evidence: A]; and lifestyle and pharmacotherapy measures in patients with diabetes to achieve a near-normal A1c level of <7% [Level of Evidence: B]. *Anderson JL, Adams CD, Antman EM, et al. ACC/AHA 2007 guidelines for the management of patients with unstable angina/non–ST-elevation myocardial infarction: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the 2002 Guidelines for the Management of Patients With Unstable Angina/Non–ST-Elevation Myocardial Infarction). J Am Coll Cardiol. 2007;50:e1-e157. † Some uncertainty exists about optimum dosing of clopidogrel. Randomized trials establishing its efficacy and providing data on bleeding risks used a loading dose of 300 mg orally followed by a daily oral maintenance dose of 75 mg. Higher oral loading doses such as 600 or 900 mg of clopidogrel more rapidly inhibit platelet aggregation and achieve a higher absolute level of 15 STANDING ORDERS ADMIT – Unstable Angina/Non–ST-Elevation MI (NSTEMI) ACC/AHA Class I Recommendations* in Bold inhibition of platelet aggregation, but the additive clinical efficacy and the safety of higher oral loading doses have not been rigorously established. ‡ Risk factors for cardiogenic shock (the greater the number of risk factors present, the higher the risk of developing cardiogenic shock): age >70 years, SBP <120 mm Hg, sinus tachycardia >110 or heart rate <60, increased time since onset of symptoms of UA/NSTEMI. § Limited data are available for the use of other LMWHs in UA/NSTEMI. 16