Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
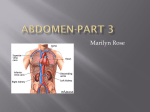
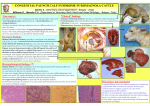
CAS CLINIQUE / CASE REPORT IDIOPATHIC RETROPERITONEAL FIBROSIS PRESENTING AS RECURRENT SCROTAL EDEMA Report of a Case and Review of the Literature http://www.lebanesemedicaljournal.org/articles/62-1/case1.pdf 1 2 1 1,2 2 Rawan SAAB , Mansour KHOURY , Claude AFIF , Roula BOU KHALIL , Chadi BECHARA , Albert GHAOUI 2 2 2 1,2 Maroun GHABACH , Wajih RIAKOS, Sleiman OBEID , Jean OBEID , Georges AFTIMOS, Said FARHAT 2 Saab R, Khoury M, Afif C, Bou Khalil R, Bechara C, Ghaoui A, Ghabach M, Riakos W, Obeid S, Obeid J, Aftimos G, Farhat S. Idiopathic retroperitoneal fibrosis presenting as recurrent scrotal edema : Report of a case and review of the literature. J Med Liban 2014 : 62 (1) : 48-53. Saab R, Khoury M, Afif C, Bou Khalil R, Bechara C, Ghaoui A, Ghabach M, Riakos W, Obeid S, Obeid J, Aftimos G, Farhat S. Fibrose rétropéritonéale idiopathique manifestée par un œdème scrotal récurrent : Cas clinique et revue de la littérature. J Med Liban 2014 : 62 (1) : 48-53. ABSTRACT : Primary or idiopathic retroperitoneal fibrosis, first described by Ormond in 1948, is a rare and elusive diagnosis, requiring a high level of suspicion. Patients usually present with entrapment of retroperitoneal organs, the most common being the ureters, causing hydronephrosis and acute kidney injury. Here, we present the case of a 56-year-old male presenting for recurrent and intermittent scrotal edema. Upon routine laboratory workup, he was found to have an elevated creatinine level. Imaging showed encasement of bilateral ureters. Bilateral ureteral stents were placed with relief of his obstructive uropathy, followed by normalization of creatinine. The patient later underwent laparoscopic release of retroperitoneal adhesions. Biopsies taken from the operative site showed fibroblast proliferation and elements of acute and chronic inflammation. With further workup of etiologies being negative, he was diagnosed with idiopathic retroperitoneal fibrosis. RÉSUMÉ : La fibrose rétropéritonéale idiopathique, d’abord décrite par Ormond en 1948, est un diagnostic rare et difficile, nécessitant un haut niveau de suspicion. Les patients se présentent habituellement avec une compression des organes rétropéritonéaux, les plus communs étant les uretères, résultant en une hydronéphrose, et une insuffisance rénale aiguë. Nous décrivons ici le cas d’un patient de 56 ans qui s’est présenté pour un œdème scrotal récurrent et intermittent. Le bilan de routine révéla une insuffisance rénale aiguë. Un CT scan abdominal a montré l’obstruction des deux uretères. L’uropathie obstructive disparut après l’insertion de deux sondes double J entraînant la normalisation de la créatinine. Le patient a subi plus tard une urétérolyse laparoscopique. Les biopsies prélevées ont montré une prolifération de fibroblastes et d’éléments résultant d’une inflammation aiguë et chronique. Un bilan plus approfondi pour exclure d’autres étiologies s’étant révélé négatif, le diagnostic fut celui d’une fibrose rétropéritonéale idiopathique. Keywords : acute renal failure, scrotal edema, inflammatory syndrome, ureterolysis Mots-clés : insuffisance rénale aiguë, œdème scrotal, syndrome inflammatoire, urétérolyse INTRODUCTION retroperitoneal fibroplasias, it affects one patient per 200,000 to 500,000 individuals, with no racial predilection, but males being twice to three times more affected than females [2-3]. Retroperitoneal fibrosis may be primary (Ormond’s disease) or secondary to malignancy [4-5], medications [3] or contiguity to inflammation (Table I). It has been described in 5% of abdominal aortic aneurysm cases as well, and called “inflammatory aortic aneurysm” [6]. The etiology of the disease is unknown, though it has been suggested to be immunologically-mediated, due to association with autoimmune diseases, and the response to corticosteroids as well as immunosuppressive therapy [7]. In addition, up to 15% of patients have extra-retroperitoneal fibrotic processes including sclerosing cholangitis, mediastinal fibrosis, fibrosing thyroiditis (Riedl’s thyroiditis), and fibrotic orbital pseudotumors [8-9]. Here we describe a case of a patient that presented for Retroperitoneal fibrosis, also known as Ormond’s disease, was described as a clinical entity in 1948 [1]. It is a rare collagen vascular disease, characterized by the formation of plaque-like fibrosis in the retroperitoneal tissue, mainly on the anterior surface of the fourth and fifth lumbar vertebrae. As a result, the structures are entrapped retroperitoneally, namely the ureters; other involved organs may be compromised, such as the small bowel, colon and spinal cord. Also known as retroperitoneal fasciitis or chronic 1 Saint George University Medical Hospital, Balamand University, Beirut, Lebanon. 2 Rosary Sisters Hospital, Ashrafieh, Beirut, Lebanon. Corresponding author: Said Farhat, MD. Saint George University Medical Hospital. Ashrafieh-Beirut. Lebanon. e-mail: [email protected] 48 Lebanese Medical Journal 2014 • Volume 62 (1) TABLE I ACQUIRED ETIOLOGIES OF RETROPERITONEAL FIBROSIS ACQUIRED ETIOLOGIES Malignancy Irradiation Trauma Inflammation Medication NOTES Metastatic colon and breast cancer, lymphomas, sarcomas, carcinomas of the lung, cervix, prostate and bladder. Malignant retroperitoneal fibrosis is distinguished radiologically from retroperitoneal lymph nodes metastasis by medial displacement of the ureters. Treatment of pelvic tumors Peritoneal injury Chronic retroperitoneal inflammation, mainly due to aortitis (a result of severe atherosclerosis and plaque necrosis) Beta-blockers, methylsergide and methyldopa recurrent scrotal edema that was misdiagnosed as inguinal hernia and was found to have retroperitoneal fibrosis. CASE REPORT A 56-year-old male patient presented to our hospital for a hernia repair. He had been complaining of intermittent scrotal edema, without erythema or pain. He presented to his general practitioner who found no palpable masses upon examination, and was diagnosed with an inguinal hernia, for which a non steroidal anti-inflammatory drug was prescribed, without improvement. He presented for a preoperative examination. Upon evaluation, a hernia could not be found. A general workup was ordered. Laboratory results showed renal failure with creatinine of 3.11 mg/dl (0.50-1.20), urea: 61 mg/dl (10-50), phophorus: 5.9 mg/dl (2.6-5), magnesium: 2.8 (1.6-2.6), hemoglobin: 10.8 g/dl (13-18), hematocrit: 33.5% (38-50%) and C-reastive protein: 77 mg/l (negative at < 5 mg/l). An abdomen-pelvis ultrasound was done, showing bilateral increase in kidney size of 13 cm on the right, and 13.4 cm on the left with no parenchymal disease; a bilateral pelvicalyceal dilatation was noted, without nephrolithiasis. Doppler ultrasound of the renal vessels was normal. A CT scan followed (Fig. 1a), revealing the same bilateral moderate hydronephrosis, with diffuse infiltration of the retroperitoneal fat surrounding the aorta and inferior vena cava. There was thickening of the peritoneal reflections at the level of the renal arteries, reaching the bifurcation; this infiltration could be responsible for the bilateral renal dilatation. There were no perivascular adenopathies. Urgent bilateral double J ureteral stents were inserted with subsequent normalization of the creatinine within six days. Retroperitoneal fibrosis was suspected. A tuberculin skin test was positive at 15 mm. HIV, hepatitis B and hepatitis C studies were negative. ANA profile was found negative, with C3 and C4 levels being normal. RA test for rheumatoid arthritis was also done, with negative results (< 8 IU/ml). Erythroid sedimentation rate (ESR) was elevated, at 117 mm (1-13), in addition to a B2 microglobulin level elevated at 3.96 mg/l (0.8-1.2). Protein electrophoresis b FIGURE 1. Abdomen and pelvis CT scan. (a) Patient scan upon presentation, with diffuse infiltration of the retroperitoneal fat surrounding the aorta and inferior vena cava. (b) CT scan six months later, following steroid therapy. R. SAAB et al. – Idiopathic retroperitoneal fibrosis Lebanese Medical Journal 2014 • Volume 62 (1) 49 FIGURE 2 Histopathology of retroperitoneal fibrosis biopsy Focal adipose tissue invasion by dense hyaline fibrosis and immune-electrophoresis followed, showing absence of monoclonality. Further workup with urinary 5-hydroxyindoleacetic acid was also negative. Upper endoscopy followed, showing mild active gastritis, and biopsy revealing the presence of Helicobater pylori. Colonoscopy revealed no abnormalities. Following improvement in clinical and laboratory findings, a laparoscopic bilateral release of retroperitoneal adhesions was performed, with biopsy of the retroperitoneal adipose tissue, which was sent to pathology. A Mycobacterium tuberculosis polymerase chain reaction (PCR) was done, with negative results. Histology revealed focal adipose tissue invasion by dense hyaline fibrosis, with inflammatory exudates composed of plasma cells and few neutrophils (Fig. 2). The conclusion was compatible with idiopathic retroperitoneal fibrosis. The patient was treated with steroids (1 mg/kg) for six months. A repeat abdomen-pelvis CT scan done six months later showed significant improvements, with decreased retroperitoneal fat infiltration, and decreased peritoneal thickening (Fig. 1b). Three months later, the double JJ stents were successfully removed, with creatinine remaining persistently normal for up to four months post removal. A repeat CT scan was normal as well. The scrotal edema progressively resolved over a period of two months after initiation of steroid therapy. He was kept on low dose steroids for two years with a maintained response. PATHOLOGY Examination reveals dense retroperitoneal plaques, on the anterior aspect, beginning at the aortic bifurcation, extending caudally to envelop the aorta and inferior vena cava, as well as the ureters, bilaterally in 2/3 of cases [10]. The aortic branches may also be involved, namely the gonadal, renal, celiac and superior mesenteric arteries. Association with other vasculitic and connective tissue disease has been described, such as ankylosing spondylitis, polyarteritis nodosa, systemic lupus erythe50 Lebanese Medical Journal 2014 • Volume 62 (1) matosus and others [9-11]. In the early disease stages, the plaque consists of a highly vascularized tissue, with collagen deposition and leukocyte infiltrates (macrophages, polyclonal B cells, CD4 + T cells). Rarely, vasculitic lesions may be found in that inflammatory magma [9, 12]. Gradually, the tissue is replaced by fibrosis. The periaortic infiltrate in Ormond’s disease is comparable to that of inflammatory abdominal aortic aneurysm. Severe aortic atherosclerosis and damage to the aortic media is usually, however not uniformly, present. The breaching of the media has raised the suggestion that retroperitoneal fibrosis develops as an autoimmune response to antigens within the severely atherosclerotic aorta [13]. In some cases, the immune reaction is triggered by an external agent, and some drugs are implicated, namely methlysergide, methyldopa and ß-blockers [3]. These agents act as haptens, triggering a hypersensitivity or autoimmune reaction. Methylsergide is a strong serotonin antagonist, causing a rebound serotonin release following prolonged intake. In patients with carcinoid tumors, again, serotonin or its metabolites has been found to trigger the immune response. The association of the disease with familial, as well as connective tissue diseases suggests a role for genetic factors [14]. As an example, the human leukocyte antigen (HLA) B27, present in ankylosing spondilitis, has also been demonstrated in several patients with retro-peritoneal fibrosis [15]. Further investigation also showed an association with the abundant presence of plasma cells. These cells are rich in immunoglobulins, specifically the IgG class 4 (IgG4). The findings led investigators to implement the term “hyperimmunoglobulin G4 syndrome” [16]. PATHOGENESIS Sixty to 70% of retroperitoneal fibrosis cases are idiopathic [4, 17-18]. Associated etiologic factors comprise the rest of the conditions leading to secondary disease, Table I. R. SAAB et al. – Idiopathic retroperitoneal fibrosis Some connective tissue diseases have been associated with retroperitoneal fibrosis [9, 11, 13, 19] (Table II). CLINICAL FEATURES Symptoms are vague and nonspecific, leading to a late diagnosis (6-12 months following the onset of physical complaints) [9-10]. The peak incidence in adults is around 40-60 years of age [6]. Presentation in childhood is extremely rare, with around 33 cases in patients younger than 18 years of age being reported [19-20]. In around 90% of the cases, the most common symptoms are colicky poorly localized pains in the lower abdomen, flanks, back or scrotum [21]. Fever, thrombophlebitis and lower limb edema are also reported. Uncommon nonspecific symptoms include anorexia, nausea, vomiting and weight loss. Review of the literature reveals reports of Raynaud’s phenomenon, limb claudication and urinary symptoms, such ureteral colics, hematuria and frequency. Another rare and confusing manifestation of idiopathic retroperitoneal fibrosis is scrotal involvement and edema, resulting from the extrinsic compression of the gonadal venous and lymphatic systems [22-23], making the presentation of our patient unique. Patients with autoimmune conditions such as inflammatory bowel disease and sclerosing cholangitis may have associated retroperitoneal fibrosis. As such, diagnosis requires a high degree of suspicion. The disease progresses through two clinical stages: an early stage, related to the onset of the inflammatory process, and a late stage, due to compression and entrapment of the retroperitoneal organs [21]. Symptoms can be grouped as early and late, as in table III. DIAGNOSIS As previously stated, diagnosis of retroperitoneal fibrosis requires a high index of suspicion. Confirmatory laboratory results include: elevated inflammatory markers (such as ESR, CRP and alkaline TABLE III EARLY AND LATE SYMPTOMS Early Symptoms Dull pain (poorly localized, back, flank, scrotum or lower abdomen) Ureteral obstruction, hydronephrosis & renal insufficiency Venous thromboembolism (up to 25%) Lower extremity edema Late Symptoms Nausea, vomiting, anorexia, malaise Hypertension Weight loss Small bowel obstruction / Pseudo-obstruction R. SAAB et al. – Idiopathic retroperitoneal fibrosis TABLE II CONNECTIVE TISSUE DISEASES AND VASCULITIDES Associated Connective Tissue Diseases Ankylosing spondylitis Scleroderma Systemic vasculitides (Wegener’s granulomatosis, polyarteritis nodosa) Systemic lupus erythematosus Rheumatoid arthritis Riedl’s thyroiditis phosphatase), normocytic normochromic anemia (compatible with chronic inflammatory disease), raised urea and creatinine levels (in 50 to 75% of cases due to ureteral entrapment), and polyclonal hypergammaglobulinemia (and hyper IgG4 [16]). Imaging may include intravenous pyelography (IVP), showing medially deviated and narrowed ureters, with proximal dilatation and various degrees of hydronephrosis. The middle third portion is the most involved. These findings, however, are not specific for retroperitoneal fibrosis [10]. Ultrasound is used as well, revealing clearly marginated and markedly hypoechoic retroperitoneal infiltrative masses. As for the CT scan, it shows a sharply marginated homogeneous soft tissue mass encasing the ureters and abdominal aorta, enhancing with contrast. The inferior vena cava may be encased between the renal hila and the sacral promontory [10]: Magnetic resonance imaging (MRI) is the diagnostic method of choice, revealing the chronic retroperitoneal mass with intermediate T1 signal intensity, and low T2 intensity. High T2 signal intensity may be due to more acute active disease or secondary retroperitoneal fibrosis due to malignancy. Despite the advances in imaging techniques, a biopsy is required for histological confirmation, and differentiation of idiopathic retroperitoneal fibrosis from secondary retroperitoneal fibrosis due to other causes. MANAGEMENT Goals of management are to preserve renal function, prevent organ involvement and relieve symptoms, which require integration of both surgical and nonsurgical therapies. Empirical treatment regimen includes corticosteroids and immunosuppressive therapies. Corticosteroids offer beneficial effects through antiinflammatory actions, and inhibition of fibrotic tissue maturation. In 2002, Van Bommel [24] reported a satisfactory outcome with corticosteroids, however, despite their successes, the use of these agents as first-line therapy is still controversial. A standard protocol is prednisolone 40-60 mg/day, tapered to 10 mg/day within two to three months, and discontinued within one to two years. Combining corticosteroids with azathioprine or peniLebanese Medical Journal 2014 • Volume 62 (1) 51 cilliamine may be useful in patients displaying signs of inflammation, as witness by raised levels of ESR and CRP, positive ANA results and positive positron emission tomography (PET) findings [25]. Combination with ureteral surgery showed decrease in restenosis, however the response may vary, and very high levels of corticosteroids may be required, and side effects outweigh the benefits of treatment [26]. Tamoxifen, a nonsteroidal antiestrogen, was used in 1991 by Clarke et al. [27] in the treatment of retroperitoneal fibrosis. Though the mechanism is not entirely clear, tamoxifen increases the synthesis of the inhibitory growth factor transforming growth factor-ß (TGF-ß), which may decrease the size of the fibrotic mass [28]. In a randomized, open-label, controlled trial, Vaglio et al. [29] compared the efficacy of prednisone with that of tamoxifen with a variable protocol. Compared with steroids, tamoxifen has lower adverse effects, however, the increased risk of thromboembolism and ovarian cancer should be carefully considered [30]. Mycophenolate mofetil was also studied, acting by blocking the proliferation of T and B lymphocytes. In 2008, Swartz et al. [31] conducted a trial using highdose prednisone and mycophenolate mofetil (1000 mg bid) as steroid-sparing therapy, discontinued within 6 to 12 months. Recent studies show radiologic regression of the mass, with improvement in outcome. When steroid therapy has failed to be tapered, azathioprine has been used as a steroid-sparing treatment. Cogan and Fastrez [32] used 150 mg/day of azathioprine for six weeks in a patient who recurred following discontinuation of steroid therapy, with a significant response. Experimental therapies with immunosuppressive agents such as methotrexate, cyclosporine and cyclophosphamide have showed promising results. Future steroid-sparing options could include biologic disease modifying agents such as tumor necrosis alpha (TNF α) inhibitors, and anti-CD20 drugs [33]. Surgical management confirms the diagnosis. It is required in severe organ encasement, mainly in ureteral involvement. Release of retroperitoneal adhesions is the procedure of choice, but is reserved for moderate to severe manifestations, due to the occurrence of post surgical adhesions [34-37]. CONCLUSION Retroperitoneal fibrosis is a rare disease, occurring as primary Ormond’s disease, or secondary to many etiological factors. Diagnosis is based on a high index of suspicion, as symptoms are vague, and the disease is insidious. Treatment is a combination of medical and surgical therapy, and future immune modulators and disease-modifying agents are promising. Because of asymptomatic recurrences of retroperitoneal fibrosis, patients require close follow-up. SOURCES OF SUPPORT (Funds, grants, drugs): none. 52 Lebanese Medical Journal 2014 • Volume 62 (1) REFERENCES 1. Ormond JK. Bilateral ureteral obstruction due to envelopment and compression by an inflammatory retroperitoneal process. J Urol 1948; 59: 1072-9. 2. Kottra JJ, Dunnick NR. Retroperitoneal fibrosis. Radiol Clin North Am Nov 1996; 34 (6): 1259-75. 3. Higgins PM, Aber GM. Idiopathic retroperitoneal fibrosis – an update. Dig Dis 1990; 8 (4): 206-22. 4. Lepor H, Walsh PC. Idiopathic retroperitoneal fibrosis. J Urol Jul 1979; 122 (1): 1-6. 5. Thomas MH, Chisholm GD. Retroperitoneal fibrosis associated with malignant disease. Br J Cancer Nov 1973; 28 (5): 453-8. 6. Von Fritschen U, Maltzfeld E, Clasen A, Kortmann H. Inflammatory abdominal aortic aneurysm: a postoperative course of retroperitoneal fibrosis. J Vasc Surg 1999; 30: 1090-8. 7. Carton RW, Wong R. Multifocal fibrosclerosis manifested by vena caval obstructions and associated with vasculitis. Ann Intern Med Jan 1969; 70 (1): 81-6. 8. Izzedine H, Servais A, Launay-Vacher V, Deray G. Retroperitoneal fibrosis due to Wegener’s granulomatosis: a misdiagnosis as tuberculosis. Am J Med Aug 1 2002; 113 (2): 164-6. 9. Zabetakis PM, Novich RK, Matarese RA, Michelis MF. Idiopathic retroperitoneal fibrosis: a systemic connective tissue disease? J Urol Jul 1979; 122 (1): 100-2. 10. Monev S. Idiopathic retroperitoneal fibrosis: Prompt diagnosis preserves organ function. Cleveland Clinic Journal of Medicine 2002; 69 (2): 160-6. 11. Littlejohn JO, Keystone EC. The association of retroperitoneal fibrosis with systemic vasculitis and HLA-B27: a case report and review of the literature. J Rheumatol 1981; 8: 665-9. 12. Parums DV, Choudhury RP, Shields SA, Davies AH. Characterisation of inflammatory cells associated with “idiopathic retroperitoneal fibrosis”. Br J Urol Jun 1991; 67 (6): 564-8. 13. Ramshaw AL, Roskell DE, Parums DV. Cytokine expression in aortic adventitial inflammation associated with advanced atherosclerosis (chronic periaortitis). J Clin Pathol 1994; 47: 721-7. 14. Hatsiopoulou O, Irving S, Sharma SD. Retroperitoneal fibrosis in 2 brothers. J Urol Jan 2001; 165 (1): 182. 15. Astudillo L, Alric L, Jamard B, Laroche M. [Retroperitoneal fibrosis in an HLA-B27-positive patient]. Rev Med Interne Dec 1999; 20 (12): 1149-50. 16. Neild GH, Rodriguez-Justo M, Wall C, Connolly JO. Hyper-IgG4 disease: report and characterisation of a new disease. BMC Med Oct 6 2006; 4: 23. 17. van Bommel EF, van Spengler J, van der Hoven B, Kramer P. Retroperitoneal fibrosis: report of 12 cases and a review of the literature. Neth J Med Dec 1991; 39 (5-6): 338-45. 18. Buff DD, Bogin MB, Faltz LL. Retroperitoneal fibrosis. A report of selected cases and a review of the literature. N Y State J Med Sep 1989; 89 (9): 511-16. 19. Gilkeson GS, Allen NB. Retroperitoneal fibrosis. A true connective tissue disease. Rheum Dis Clin North Am Feb 1996; 22 (1): 23-38. 20. Buff DD, Bogin MB, Faltz LL. Retroperitoneal fibrosis. A report of selected cases and a review of the literature. N Y State J Med Sep 1989; 89 (9): 511-16. R. SAAB et al. – Idiopathic retroperitoneal fibrosis 21. 22. 23. 24. 25. 26. 27. 28. 29. Koep L, Zuidema GD. The clinical significance of retroperitoneal fibrosis. Surgery Mar 1977; 81 (3): 250-7. Ward CS, Dundas DD, Dow J, Dormandy JA, Shearer RJ. Scrotal swelling due to perianeurysmal fibrosis. Br J Urol 1988 Jun; 61 (6): 536-8. Schulte-Baukloh H, Knispel HH, Dallenbach F, Miller K. Scrotal involvement with idiopathic retroperitoneal fibrosis. J Urol 1999 Nov; 162 (5): 1692-3. van Bommel EF. Retroperitoneal fibrosis. Neth J Med Jul 2002; 60 (6): 231-42. Harreby M, Bilde T, Helin P. Retroperitoneal fibrosis treated with methylprednisolone pulse and disease-modifying antirheumatic drugs. Scand J Urol Nephrol Sep 1994; 28 (3): 237-42. Wagenknecht LV, Hardy JC. Value of various treatments for retroperitoneal fibrosis. Eur Urol 1981; 7 (4): 193200. Clark CP, Vanderpool D, Preskitt JT. The response of retroperitoneal fibrosis to tamoxifen. Surgery. Apr 1991; 109 (4): 502-6. Frankart L, Lorge F, Donkier J. Tamoxifen for retroperitoneal fibrosis. Postgrad Med J 1997; 73: 653-4. Vaglio A, Palmisano A, Alberici F et al. Prednisone versus tamoxifen in patients with idiopathic retroperitoneal fibrosis: an open-label randomised controlled trial. Lancet Jul 23 2011; 378 (9788): 338-46. R. SAAB et al. – Idiopathic retroperitoneal fibrosis 30. 31. 32. 33. 34. 35. 36. 37. Monev S, Remer E, Calabrese L. Effect of tamoxifen in patients with idiopathic retroperitoneal fibrosis. Arthritis Rheum 1998; 41 (suppl): 419. Swartz RD, Lake AM, Roberts WW, Faerber GJ, Wolf JS Jr. Idiopathic retroperitoneal fibrosis: a role for mycophenolate mofetil. Clin Nephrol Apr 2008; 69 (4): 260-8. Cogan E, Fastrez R. Azathioprine. An alternative treatment for recurrent idiopathic retroperitoneal fibrosis. Arch Intern Med Apr 1985; 145 (4): 753-5. McDougal WS, MacDonell RC. Treatment of idiopathic retroperitoneal fibrosis by immunosuppression. J Urol 1991; 145: 112-14. Kerr WS, Suby HI, Vickery A, Fraley E. Idiopathic retroperitoneal fibrosis: clinical experiences with 15 cases, 1956-1967. J Urol May 1968; 99 (5): 575-84. Kavoussi LR, Clayman RV, Brunt LM, Soper NJ. Laparoscopic ureterolysis. J Urol Feb 1992; 147 (2): 426-9. Fugita OE, Jarrett TW, Kavoussi P, Kavoussi LR. Laparoscopic treatment of retroperitoneal fibrosis. J Endourol Oct 2002; 16 (8): 571-4. Styn NR, Frauman S, Faerber GJ, Wolf JS Jr. University of Michigan surgical experience with ureterolysis for retroperitoneal fibrosis: a comparison of laparoscopic and open surgical approaches. Urology Feb 2011; 77 (2): 339-43. Lebanese Medical Journal 2014 • Volume 62 (1) 53