Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
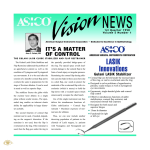
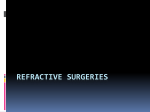
Table 3. CNV Lesion Size and Last FA Results Total Area of CNV, mm2 Patient Baseline Last Last FA 1 2 3 4 5 0.99 0.26 0.82 0.19 0.88 0.99 0.21 0.68 0.16 0.87 Min No Min No Min Abbreviations: CNV, choroidal neovascularization; FA, fluorescein angiography; Min, leakage size less than 50% of the area found at baseline; No, no leakage. corrected VA (BCVA) at baseline ranged from 10/160 to 10/16. Baseline BCVA in patient 1 was 10/50 and reached a value of 10/16 3 months later. At the beginning of the study, patients 2 and 5 (treated with PDT) had BCVAs of 10/160 and 10/100, respectively. One week after IVB injection, their BCVAs increased to 10/ 100 and 10/25, respectively, and this result was stable up to the end of follow-up. One week after the injection, the BCVA of patient 3 increased from 10/32 to 10/22; at the end of the follow-up (6 months), his BCVA further improved to 10/16. The BCVA of patient 4 quickly improved from 10/16 to 10/10. This patient was monitored for 9 months, and at the last follow-up check, his BCVA was 10/12.5 (Table 2). Angiographic examinations showed a decreased CNV leakage in all patients, whereas the CNV size did not show significant variation over the follow-up period (Table 3). Lastly, neither systemic nor local adverse effects were reported following IVB injection. Comment. Current available laser treatments for CNV secondary to AS have a poor outcome. This might be because of the high angiogenic activity present in CNV, which could be worsened by the VEGF stimulation and up-regulation induced by the treatment itself.5 These data support IVB use in the management of CNV due to AS. In our experience, IVB injection did not modify the CNV size, whereas an increase in final lesion size in CNV due to AS has been reported after PDT.2 In our small series of patients, FA leakage diminished in patients 1, 3, and 5 and was completely absent in patients 2 and 4. A reduction of CRT was recorded in all subjects. This change of retinal morphology is likely to be the result of a combined antiexudative effect due to the decrease of vessel permeability and the antiproliferative effect due to the inhibition of further CNV growth following the VEGF blockage.5 The smallest reduction was recorded in the 2 patients who had previously undergone PDT. These anatomical improvements were associated with concomitant increases in VA (a mean of 3-4 lines). The mechanism of this outcome remains uncertain. A previous case report of CNV due to AS treated with IVB by Teixeira and coworkers4 shows an improvement of the patient’s BCVA. Posttreatment optical coherence tomography and FA imaging showed no presence of subsensory fluid or leakage, respectively. Our data seem to confirm the efficacy and safety of anti-VEGF therapy in eyes with CNV secondary to AS, although we realize that the present study has some limitations, including the limited number of patients and the short period of follow-up. Nevertheless, considering the relative rarity of the disease, it would be difficult to conduct randomized controlled trials, which require a higher number of patients with CNV secondary to AS. Michele Rinaldi, MD Roberto dell’Omo, MD Mario R. Romano, MD Flavia Chiosi, MD Ugo Cipollone, MD Ciro Costagliola, MD Correspondence: Dr Costagliola, Dipartimento di Scienze per la Salute, Università degli Studi del Molise, Via Francesco De Sanctis s.n.c., 86100 Campobasso, Italy (ciro.costagliola @unimol.it). Financial Disclosure: None reported. 1. Gass JDM. Angioid Streaks: Stereoscopic Atlas of Macular Diseases. St Louis, MO: Mosby; 1997: 118-123. 2. Menchini U, Virgili G, Varano M, et al. Outcome of choroidal neovascularization in angioid streaks after photodynamic therapy. Retina. 2004;24(5):763-771. 3. Rich RM, Rosenfeld PJ, Puliafito CA, et al. Shortterm safety and efficacy of intravitreal bevaci- (REPRINTED) ARCH OPHTHALMOL / VOL 125 (NO. 10), OCT 2007 1423 zumab (Avastin) for neovascular age-related macular degeneration. Retina. 2006;26(5): 495-511. 4. Teixeira A, Moraes N, Farah ME, Bonomo PP. Choroidal neovascularization treated with intravitreal bevacizumab (Avastin) in angioid streaks. Acta Ophthalmol Scand. 2006;84(6): 835-836. 5. Gomi F, Nishida K, Oshima Y, et al. Intravitreal bevacizumab for idiopathic choroidal neovascularization after previous injection with posterior subtenon triamcinolone. Am J Ophthalmol. 2007;143(3):507-509. Laser In Situ Keratomileusis Flap Necrosis After Trigeminal Nerve Palsy Laser in situ keratomileusis (LASIK) surgery can induce changes in the corneal epithelium owing to a neurotrophic phenomenon as a consequence of the sectioning of nerves during flap cutting. 1 More profound alterations have been reported with a superior hinge, compared with a nasal hinge, and the associated effects tend to normalize over approximately 6 months,2 although it is possible that complete reinnervation and recovery of the basal state may not occur.3 Epithelial damage has also been associated with a reduced blinking rate, which favors corneal exposition.4 To date, various cases of postLASIK neurotrophic epitheliopathy have been reported, characterized by symptoms and signs of dry eye and a spotted distribution of rose bengal dye. Recommended treatments include artificial tears, tear plug, and autologous serum,5 among others. Herein, we report a case of severe corneal flap necrosis that occurred after formation of a trigeminal nerve lesion of vascular origin. The patient was successfully treated with autologous plasma rich in growth factors (PRGF).6 Report of a Case. A male patient, 48 years old and a smoker, underwent LASIK surgery of both eyes in 2000 for myopia (−5.00 OD and −6.00 OS). A microkeratome (Hansatome; Bausch & Lomb, Rochester, New York) was used to produce a cut with a diameter of 8.5 mm and a depth of 160 µm. Postoperative evolution was without incident, and the patient demonstrated satisfactory visual and clinical recuperation. WWW.ARCHOPHTHALMOL.COM ©2007 American Medical Association. All rights reserved. Downloaded From: http://archneur.jamanetwork.com/ on 10/21/2014 In December 2003, the patient arrived at the accident and emergency service of a local general hospital with what appeared to be a leftsided cerebrovascular injury, which was confirmed on brain computed tomographic scan. The same scan revealed several areas of small lacu- nar infarctions, one of them affecting the deep area of the right medial cerebral artery, for which the patient was asymptomatic. He was hospitalized for 5 days. In May 2004, as a result of visual loss in his left eye in the absence of pain, the patient consulted Figure 1. Flap necrosis at the inferior edge of the laser in situ keratomileusis flap. his ophthalmologist, who observed flap necrosis at the inferior edge (Figure 1). Lubricant treatment was initiated, and because of poor evolution, the patient was referred to our center for further treatment. At that stage, he had necrosis of the temporal half of the flap associated with anesthesia of the left trigeminal region. The patient was treated successively during the following weeks with artificial tears without preservatives, tear plug, autologous plasma, cyanoacrylate adhesive, amniotic membrane patch, and a bandage contact lens. Two months later, epithelialization was achieved, leaving as a consequence an anterior stromal opacity and notable topographic irregularity (Figure 2), which only permitted a bestcorrected visual acuity of less than 20/200, as measured with eyeglasses. To improve corneal irregularity, we proceeded in October 2005 to extirpate the flap remnant and apply temporal tarsorrhaphy together with 3 layers of amniotic membrane to increase the permanence period, together with temporal tarsorrhaphy. Despite this procedure, an exten- Figure 2. Orbscan (Bausch & Lomb, Rochester, New York) showing the corneal irregularity after partial flap necrosis. (REPRINTED) ARCH OPHTHALMOL / VOL 125 (NO. 10), OCT 2007 1424 WWW.ARCHOPHTHALMOL.COM ©2007 American Medical Association. All rights reserved. Downloaded From: http://archneur.jamanetwork.com/ on 10/21/2014 eye to respond to certain situations that involve aggression to the ocular surface. Without ruling out the possibility that the trigeminal lesion may have caused a corneal ulcer, this patient demonstrated flap necrosis with minimum repercussion in the deep corneal layers. On removal of the flap remains and despite measures to favor reepithelialization, signs of wound healing were not apparent. In light of this poor response and the risk of corneal melting, treatment with PRGF was initiated. This treatment has been used previously in maxillofacial and orthopedic surgery. Treatment with PRGF involves obtaining platelet and plasma proteins from the patient. The extract contains a high concentration of growth factors that can enhance the mechanisms of repair and regeneration in distinct tissues.6 It is prepared by centrifuging a sample of the patient’s blood and obtaining a plasma fraction enriched in platelets from which growth factors are released with the addition of calcium chloride. This treatment is being used in other patients with different forms of neurotrophic keratitis and is being subjected to further evaluation to characterize its efficacy. Figure 3. Epithelial defect after the amniotic membrane dissolution (lissamine green). Germa´n A. Rocha, MD Arantxa Acera, DSc Juan A. Dura´n, MD Correspondence: Dr Dura´n, Instituto Clı´nico-Quiru´rgico de Oftalmologı´a, Virgen de Begon˜a 34, 48006 Bilbao, Spain ([email protected]). Financial Disclosure: None reported. Figure 4. Improvement of the epithelial defect after treatment with autologous plasma rich in growth factors. sive epithelial defect in the resected zone persisted 1 month later (Figure 3). Consequently, in December 2005 and with the informed consent of the patient, we decided to commence treatment with PRGF (GAC Medical, Vitoria, Spain). Initially, approximately 20 µL (1 drop) was administered every 2 hours, progressively reducing the frequency of administration in accord with the observed improvement. During the following 6 weeks, progressive epithelial closure was observed (Figure 4), although long- term irregularity of the epithelium and opacity of the underlying stroma persisted. The final best-corrected visual acuity was 20/200. Comment. This case presents 2 particularly salient aspects. First, we report flap necrosis due to a trigeminal nerve lesion more than 3 years after LASIK surgery. Second, we describe a novel method for the successful treatment of neurotrophic ulcers. The first aspect raises doubts about the capacity of a LASIK-operated on (REPRINTED) ARCH OPHTHALMOL / VOL 125 (NO. 10), OCT 2007 1425 1. Wilson SE, Ambro´sio R. Laser in situ keratomileusis–induced neurotrophic epitheliopathy. Am J Ophthalmol. 2001;132(3):405-406. 2. Donnenfeld ED, Solomon K, Perry HD, et al. The effect of hinge position on corneal sensation and dry eye after LASIK. Ophthalmology. 2003;110(5):1023-1029. 3. Calvillo MP, McLaren JW, Hodge DO, Bourne WM. Corneal reinnervation after LASIK: prospective 3-year longitudinal study. Invest Ophthalmol Vis Sci. 2004;45(11):3991-3996. 4. Savini G, Barboni P, Zanini M, Tseng SCG. Ocular surface changes in laser in situ keratomileusis–induced neurotrophic epitheliopathy [published correction appears in J Refract Surg. 2005;21(1):10]. J Refract Surg. 2004;20(6): 803-809. 5. Fuchsluger TA, Steuhl K, Meller D. Neurotrophic keratopathy: a post-LASIK case report [in German]. Klin Monatsbl Augenheilkd. 2005; 222(11):901-904. 6. Anitua E, Andia I, Ardanza B, Nurden P, Nurden AT. Autologous platelets as a source of protein for healing and tissue regeneration. Thromb Haemost. 2004;91(1):4-15. WWW.ARCHOPHTHALMOL.COM ©2007 American Medical Association. All rights reserved. Downloaded From: http://archneur.jamanetwork.com/ on 10/21/2014