Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
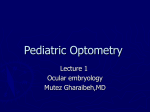
NEURO-OPHTHALMOLOGY Clinical Examination • • • • Visual Acuity Colour Vision Visual Fields Pupils Normal Eye and Optic Disc Cupped disc The swollen optic disc • Papilloedema • Papillitis • Malignant hypertension • Ischaemic optic neuropathy • Diabetic optic neuropathy • CRVO • Intraocular inflammation 25 y.o. female Reduced VA Pain with eye movement Colour desaturation RAPD 65 y.o. male Reduced VA Painless loss of vision Essential hypertension Smoker The pale optic disc • Congenital • Secondary to • raised ICP • vascular retinal disease • optic neuritis • optic nerve compression • trauma • Glaucoma Papilloedema • • • • • Disc swelling secondary to raised ICP Haemorrhages Headache – Worse in the morning – Valsalva manouver Nausea and projectile vomiting Horizontal diplopia (VI palsy) Causes Disc pallor – Space occupying lesion – Intracranial hypertension • Idiopathic • Drugs • Endocrine Vessel attenuation – Severe hypertension Blurred optic disc margin CWS Small optic cup Pupils • First Order – Retina to Pretectal Nucleus in B/S (at level of Superior colliculus) • Second Order – Pretectal nucleus to E/W nucleus (bilateral innervation!) • Third Order – E/W nucleus to Ciliary Ganglion • Fourth Order – Ciliary Ganglion to Sphincter pupillae (via short ciliary nerves) Pupil • Constricted (mioisis) – Sympathetic (pupillodilator) denervation – Drugs • Pilocarpine • Morphine • Dilated (mydriasis) – Parasympathetic (pupilloconstrictor) denervation – Lesion of the third CN – Drugs • Atropine • Cocaine Horner’s • Oculosympathetic paresis – Ptosis – Miosis – Ipsilateral anhidrosis – Does not dilate with cocaine 4% Sympathetic Pathway • First Order – Posterior Hypothalamus to Ciliospinal centre of Budge (C8-T2) (Uncrossed in Brainstem) • Second Order – Ciliospinal centre of Budge to Superior Cervical Ganaglion • Third Order – Superior Cervical Ganglion to dilator pupillae muscle. (Close to ICA and joins V1 intracranially) Internal Carotid Dissection Herpes Zoster Otitis Media Tolosa-Hunt Sy. CVA Tumour Pancoast bronchogenic carcinoma Causes of Horner’s pupil • Central – B/S lesions (tumours, vascular and MS) Syringomyelia, Lat. Med. Syn., S.C. ca. • Preganglionic – Pancoast tumour, Carotid & Aortic aneurysms, Neck lesions/trauma. • Postganglionic – Cluster headaches, Nasopharyngeal tumours, Otitis media, Cavernous sinus mass and ICA disease. • Miscellaneous – Congenital (brachial plexus injury) Idiopathic. Afferent & efferent defects • Argyll-Robertson pupil – Small, irreg – Does not react to light – Reacts to accommodation – Causes • syphilis • diabetes • Miotonic pupil (Adie’s syndrome) – Dilated – Poor response to light and convergence. • Constricts with weak Pilocarpine • Holmes-Adie syndrome – Reduced tendon reflexes (Knee, ankle) - Orthostatic hypotension Ocular motility abnormalities • Third nerve palsy – Double vision – Eye turned down & out – Ptosis – Dilated pupil & headache • Compressive lesion • Sixth nerve palsy – Double vision – Eye turned in Cranial Nerve Palsies Looking straight ahead Posterior communicating artery aneurysm Chiasma Posterior cerebral artery III CN Internuclear Ophthalmoplegia • Defective adduction of the ipsilateral eye • Nystagmus of the contralateral (abducting) eye • NORMAL CONVERGENCE • Causes – Young patients • Bilateral • Demyelination – Older patients • Unilateral • Vascular, tumours Myasthenia Gravis • • • • • Fatigability Double vision Lid twitch Ptosis Normal reflexes & sensation INVESTIGATIONS MG ACh Anti AChR Ab’s AChR • Anti ACh receptor Ab’s • Electromyography • Tensilon test – Edrophonium blocks acetyl-cholinesterase – Beware of cholinergic cardiac effects. Use with Atropine 0.6mg • Thoracic CT and MRI to rule out thymoma Localising the lesion • Monocular visual field defects indicate lesions anterior to the optic chiasm • Bitemporal defects are the hallmark of chiasmal lesions • Binocular homonymous hemianopia result from lesions in the contralateral postchiasmal region • Binocular quadrantanopias reflect optic tract lesions