Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
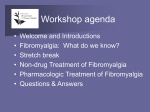
PROCEEDINGS OVERCOMING OBSTACLES: BARRIERS TO CARE IN FIBROMYALGIA TREATMENT* — M Steven P. Cohen, MD† ABSTRACT Many patients with fibromyalgia syndrome (FMS) receive inadequate or ineffective treatment, often because of multifactorial barriers that stand in the way of appropriate care. These barriers include the high prevalence of medical and psychiatric comorbidities in patients with FMS, the challenges inherent in diagnosing FMS, and the perception among many that FMS is not a “real” disease. Another major obstacle is that there is often little or no coverage for patients with FMS who do have health insurance, and restricted access to healthcare for those who do not. This article reviews these and other patient-, physician-, and process-related barriers and explains how they interfere with treatment. The article also suggests several common-sense strategies aimed at overcoming these obstacles and improving care for patients with FMS. any patients with fibromyalgia syndrome (FMS) receive inadequate or ineffective treatment. In part, this is a direct reflection of the lack of consensus among clinicians with respect to diagnosis, causes, and effective treatments. In large measure, however, inappropriate care can be attributed to numerous multifactorial barriers that need to be overcome. These barriers fall into 4 broad but interrelated categories: patient-related factors; physician-related factors; work and social impairment; and factors involving “process,” such as delayed diagnosis and inadequate healthcare coverage. The categories overlap to some extent, just as FMS frequently overlaps with several other pain syndromes and psychiatric conditions. Factors in each of the categories are reviewed in detail in this article, as well as strategies to overcome these obstacles. PATIENT-RELATED FACTORS (Adv Stud Med. 2009;9(4):115-121) *Based on a presentation developed by Dr Cohen for a national symposium series held in October and November 2009. †Associate Professor of Anesthesiology, Director of Medical Education for Pain Management Division, Johns Hopkins University School of Medicine, Baltimore, Maryland; Director of Chronic Pain Research, Walter Reed Army Medical Center, Washington, DC. Address correspondence to: Steven P. Cohen, MD, Associate Professor of Anesthesiology, Director of Medical Education for Pain Management Division, The Johns Hopkins Pain Management Division, 550 North Broadway, Suite 301, Baltimore, MD 21205. E-mail: [email protected]. Johns Hopkins Advanced Studies in Medicine n Patient-related barriers to appropriate care include the often desperate attempts of many patients to find a “cure,” which can undermine relationships and the ability to function at work. Patients with FMS have a higher prevalence of coexisting psychopathology, which may predate the physical symptoms of FMS. Depression, anxiety disorders, and post-traumatic stress disorder are the most common psychiatric diagnoses, but some studies have found a higher incidence of Axis II disorders as well. Studies conducted in patients with FMS with and without comorbid psychopathology strongly support the usefulness of cognitive-behavioral therapy. Other patient-related barriers include cognitive impairment, a host of sleep disturbances, and the high degree of overlap between FMS and several other con- 115 PROCEEDINGS 116 these other syndromes. Patients complaining of chronic widespread pain should therefore be evaluated not only for FMS, but also for chronic fatigue syndrome, multiple chemical sensitivities, irritable bowel syndrome, temporomandibular joint disorder, and other somatoform pain disorders that commonly coexist (Table 1).9,10 Figure. Proportion of Patients with FMS Reporting Worsening of Pain After Sleep by Alpha Intrusion Subtype 100 100 75 Patients, % ditions that share similar clinical features. The cognitive impairment associated with FMS, sometimes referred to as “fibrofog,” involves all aspects of memory, attention span, and task-switching. Pain and psychological, sleep, endocrine, and social problems can all exacerbate cognitive deficits. Sleep disturbances—particularly nonrestorative sleep, insomnia, early morning awakenings, poorquality sleep, delayed sleep latency, daytime fatigue, increased nocturnal physical activity, and easy arousability—are common in patients with FMS.1-3 In a recent study, up to 99% of patients reported having sleep problems; patients with FMS get an average of 5 hours of sleep per night compared with 7 to 8 hours per night for controls.3 Polysomnographic studies in patients with FMS suggest abnormalities in sleep continuity as well as sleep architecture.1,2 Rapid eye movement (REM) sleep, slow-wave sleep, and total sleep time are decreased. Sleep efficiency is further compromised because of an increased number of awakenings. In addition, there is abnormal alpha-wave intrusion in non-REM sleep. Alpha-wave intrusion—particularly of the phasic, tonic, and low alpha subtypes—is a common but nonspecific electroencephalographic finding in patients with FMS that may interfere with sleep function and contribute to worsening of pain.1,2 As demonstrated in a polysomnographic study of patients with FMS, phasic alpha sleep activity correlates strongly with worsening pain after sleep (Figure).1 Patients with phasic alpha activity also report longer duration of pain after sleep than patients with tonic alpha or low alpha activity. The history of the relationship between sleep and FMS is a long one, with early findings suggesting that FMS-like symptoms could be induced by stage 4 sleep deprivation, and that the “fibrositis” symptom complex should perhaps be considered a “nonrestorative sleep syndrome.”4 More recent findings have demonstrated inspiratory airflow dysfunction,5 a cyclic alternating pattern strongly correlated with the severity of FMS symptoms,6 sympathetic overdrive,7 and restless leg syndrome during sleep.8 Although treating these sleep-related problems is likely to benefit the patient, it clearly will not eradicate all FMS symptoms. Diagnosing FMS is a challenge because it is only one of several overlapping systemic and regional pain syndromes with shared clinical features.9 It is not unusual for patients with FMS to have 1 or more of P <.001 58 50 25 25 0 Phasic Alpha Tonic Alpha Low Alpha Reprinted with permission from Roizenblatt et al. Arthritis Rheum. 2001;44:222-230.1 Table 1. Prevalence of Selected Comorbid Conditions in Patients with FMS Comorbid Conditions Prevalence, % Chronic fatigue syndrome 21–80 Irritable bowel syndrome 32–80 Temporomandibular joint disorder 75 Headache (tension-type and migraine) 10–80 Multiple chemical sensitivities 33–55 Interstitial cystitis 13–21 Chronic pelvic pain 18 FMS = fibromyalgia syndrome. Data from Aaron and Buchwald.10 Vol. 9, No. 4 n December 2009 PROCEEDINGS Further complicating the diagnostic challenge is the frequent overlap between FMS and several psychiatric diagnoses, including major depression, obsessive compulsive disorder, bipolar disorder, post-traumatic stress disorder, generalized anxiety disorder, and panic attacks. PHYSICIAN-RELATED FACTORS Physician-related factors that can lead to ineffective care reflect how challenging it is to diagnose FMS and deal with patients who are often considered “difficult.” Even in patients who are not considered difficult, diagnosing and managing FMS is a time- and labor-intensive endeavor because of multiple physical comorbidities and a high incidence of coexisting psychopathology. Moreover, treatment success rates are low, often leading to disappointment, frustration, and even anger for patients and physicians alike. Difficult patients exhibit several distinguishing characteristics. They bring out a clinician’s negative feelings, fail to respond to multiple treatments, and do not comply with clinician recommendations. They are more likely to be “doctor shoppers,” with unrealistic expectations and low satisfaction rates. In addition to poor functional status and a high incidence of Axis I and Axis II disorders, they utilize a disproportionate share of healthcare resources and require a considerable amount of labor-intensive paperwork to support claims for disability benefits. Difficult patients can be labeled as dependent clingers, entitled demanders, manipulative help-rejectors, or self-destructive deniers.11 The identifying features of each of these patient “labels,” along with recommended treatment approaches, are summarized in Table 2. The diagnosis of FMS relies on a careful review of the patient’s medical, family, and social history, along with a thorough physical examination. The medical and family histories should focus on the presence of other pain syndromes, particularly regional somatic and visceral pain syndromes, and the social history should determine whether (and which) symptoms are triggered or exacerbated by “stressors” such as cold weather or exertion, and if there is any substance abuse. Physical examination findings are often normal except for diffuse pain and tenderness. It is important to note, however, that tenderness is not necessarily confined to the joints or the tender points identified in the American College of Rheumatology diagnostic criteria.12 In addition, weakness and sensory disturbances have been found to affect a majority of FMS sufferers.13 Another physician-related factor is the lingering question about the precise categorization of FMS (ie, is it a syndrome or is it a disease?). By definition, a syndrome lacks unequivocal diagnostic criteria, has no readily identifiable etiologic agent or well-defined pathophysiologic mechanisms, lacks characteristic physical signs, is associated with other poorly explained syndromes, is considered a “diagnosis of exclusion,” Table 2. Identifying Features and Treatment Strategies by Patient “Label” Patient “Label” Identifying Features Treatment Strategies Dependent clingers Escalating need for re-assurance and become increasingly helpless Set appropriate limits with realistic expectations Entitled demanders Initially present as “needy,” but then exhibit aggressive and intimidating behavior Control “anger,” acknowledge situation, and discuss expectations Manipulative help-rejectors Ungrateful and pessimistic about treatment Paradoxically advocate skeptical attitude to therapy and schedule regular appointments Self-destructive deniers Engage in behaviors that thwart attempts to improve their condition (eg, drinking) Avoid vengeful feelings and focus on underlying depression Reprinted with permission from Wasan et al. Reg Anesth Pain Med. 2005;30:184-192.11 Johns Hopkins Advanced Studies in Medicine n 117 PROCEEDINGS and generally carries a poor prognosis. By these standards, FMS is clearly a syndrome and not a disease. WORK AND SOCIAL FACTORS Work-related factors are important drivers of the economic burden of FMS. As shown in numerous studies, FMS is associated with increased utilization of healthcare resources and high job- and productivityrelated costs. Among patients with rheumatologic problems, one study found that FMS, osteoarthritis, and rheumatoid arthritis (RA) were associated with the highest likelihood of long-term disability.14 A comparative analysis of the economic burden of FMS and RA found that costs associated with disability and missed work days were similar for both, but that patients with FMS accounted for more emergency department and physician visits.15 Several studies examining the impact of FMS in the workplace found that annual indirect costs due to lost productivity ranged from $535 to $3411 among employees with FMS compared with $221 to $1699 among employees without FMS.16-19 Lost productivity was variously defined in these studies as work loss, workplace payments, lost wages, disability, or absenteeism. Two of these studies also examined the impact of FMS alone, depression alone, and coexisting FMS and depression on direct and indirect costs in the workplace.16,17 Both studies found that annual costs in patients with coexisting FMS and depression were higher than the sum of the individual costs of each condition. In one study, for example, the individual costs of FMS alone and depression alone totaled $10 262, but the costs of coexisting FMS and depression were $10 611.16 The corresponding costs in the other study were $8264 and $9413.17 Fibromyalgia syndrome is associated with comparatively high levels of healthcare utilization and expenditures. One study demonstrated that 1-year total healthcare costs were 3 times higher in patients with FMS than in age- and gender-matched patients who did not have FMS.20 Another study found that patients with FMS accounted for substantially more visits and prescriptions per year (25 visits and 11 prescriptions) than matched controls (12 visits and 4.5 prescriptions).21 Patients with FMS in this study also underwent more testing for a period of at least 10 years prior to diagnosis. In yet another study, 61% of patients 118 with FMS reported spending $100 to $500 per month on prescription medications.22 Although patients often report that FMS has had an adverse effect on their relationships and social functioning, social factors per se have been poorly studied. Several studies show a possible link between FMS and obesity, smoking, and divorce,23-25 whereas studies of patients with chronic pain or illness due to any cause indicate a divorce rate of approximately 75%.26 Chronic pain may also play a role in suicide. FACTORS INVOLVING “PROCESS” Factors involving “process,” which can be summarized as navigating through the healthcare system from diagnosis to treatment and follow-up, are major barriers to appropriate care. First, many physicians do not recognize FMS as a “real illness,” a circumstance that usually results in inadequate or ineffective treatment, or even no treatment at all. Second, many interventional pain clinics will not see patients with FMS because of lack of insight and/or financial reasons. And third, many insurance companies will not pay for the extended physical therapy, cognitive-behavioral therapy, or other expensive treatments that FMS often requires. Failure to recognize FMS as a real illness may also play a role in its delayed diagnosis, which averages 4 to 5 years after symptom onset,27 and in prompting multiple patient visits to multiple providers. In a study by Dobkin et al, 178 women with primary FMS saw an average of 7.2 physicians and 11.3 complementary/ alternative medicine providers during a 6-month period.28 More auspiciously, another study found that the initial diagnosis of FMS—made by family physicians who referred patients to a rheumatology clinic—was confirmed in 71% of referrals.29 Reduced access to healthcare is another major barrier to effective treatment. Of the 47 million Americans who do not have medical insurance, more than 17 million are women over the age of 18 years, the population most likely to be affected by FMS.30 Uninsured patients, regardless of gender, are more likely to suffer serious health problems. However, having health insurance is no guarantee of receiving adequate treatment because many policies exclude, or provide only partial coverage for, certain conditions, including FMS. In fact, among women who do have health insurance, over 50% have either failed to fill a pre- Vol. 9, No. 4 n December 2009 PROCEEDINGS scription or postponed or went without medical care because of cost concerns.31 A disproportionate number of uninsured people in the United States have low educational levels and socioeconomic status. Studies in the United States, Spain, Sweden, Israel, and Finland confirm that patients with FMS, regardless of their insurance status, are more likely to have low education levels and socioeconomic status.32-36 These studies also confirm that there is an inverse correlation between educational and socioeconomic levels and the severity of disability related to FMS. OVERCOMING OBSTACLES Several strategies have been suggested to overcome barriers to care in patients with FMS. These include patient and physician education, better communication between patients and healthcare professionals, medication counseling, and improved access to healthcare. Several common-sense treatment strategies that can be implemented in primary care practice are summarized below: • Establish realistic expectations and an approach to treatment that is acceptable to the patient. • Address sleep abnormalities if present. • Use a multidisciplinary approach to treat coexisting physical conditions. • Identify underlying psychological/psychiatric issues and treat/refer accordingly. • Incorporate a structured exercise program, if indicated, into the treatment regimen as early as possible. • Recognize and develop treatment strategies for “difficult” patients (Table 2). • Educate and involve patients and family members, particularly spouses, about FMS. • Utilize social work services and networks to maximize available resources for uninsured and underinsured patients. CONCLUSIONS Barriers to appropriate care for patients with FMS are multifactorial. These barriers can be broadly categorized as patient-related, physician-related, workrelated, and/or process-related. Early interventions and a multidisciplinary Johns Hopkins Advanced Studies in Medicine n approach to treatment may minimize, but not eradicate, these obstacles and ultimately result in improved patient care. CASE STUDY PRESENTATION AND H ISTO RY A 51-year-old woman with a 5-year history of diffuse body pain and a diagnosis of FMS presents with worsening pain that she attributes to “overexertion and watching the kids,” weakness, and occasional numbness. She describes her pain as “sharp, burning, tingly, gnawing, achy, stinging, and crushing,” and she notes that it is exacerbated by cold weather, activity, and stress. She has a medical history significant for low back pain, abdominal pain secondary to irritable bowel syndrome, and headaches. Her surgical history is remarkable for cholecystectomy and appendectomy. A detailed review of systems notes a long history of insomnia and symptoms consistent with depression. A former gymnast and tennis player, she is currently unemployed and recently separated, with custody of 2 teenagers. She is a recent smoker and has a family history of depression, but no history of substance abuse. She is not currently involved in a relationship and reports having no libido. At presentation, she was taking sertraline 50 mg once daily, clonazepam 1 mg 3 times a day, extended-release oxycodone 80 mg 3 times a day, immediate-release oxycodone 10 mg every 4 hours as needed, topiramate 200 mg/day, a multivitamin, and a bisphosphonate. PHYSICAL EXAMINATION AND D IAGNOSTIC EVALUATION Physical examination reveals a slightly overweight, agitated woman in obvious distress. She is diffusely tender to very light palpation with less than 2 kg/cm2 of pressure applied bilaterally, above and below the waist, and has several positive Waddell’s signs for low back pain, which indicate nonorganic pathology and a poor treatment prognosis.37 She also exhibits overreaction and patchy, nondermatomal areas of numbness, but no focal neurological signs. The diagnostic workup includes magnetic resonance imaging of the spine, which reveals mild-tomoderate spondylotic changes in the lumbar and cervical regions, and the brain, which is normal. The white blood count is normal as well. 119 PROCEEDINGS The differential diagnosis includes FMS, central pain disorder, somatoform disorder, opioid-induced hyperalgesia, and malingering/secondary gain. The latter is unlikely because she is not on or seeking disability, and she is receiving financial support from her husband. The absence of any preceding neurological event, focal neurological signs or symptoms, and spasticity eliminates central pain disorder. Her pain pattern was not consistent with a somatoform disorder. Although the distribution of her pain is consistent with a clinical diagnosis of FMS, she did have some evidence of opioid-induced hyperalgesia. Specifically, pain to extremely light touch is a hallmark of neuropathic pain or some other type of nociceptor sensitization, not FMS. The extremely high doses of opioids she was taking therefore likely signify a combination of clinical tolerance and opioid-induced hyperalgesia. N ONPHARMACOLOGIC TREATMENT The patient was referred to a sleep clinic, where she was given sleep counseling. After giving informed consent, she signed a 3-way contract (patient, pain clinic, and primary care physician) which made the pain clinic the sole prescriber of all controlled substances. By signing, she explicitly agreed to an opioid taper over 2 months and a benzodiazepine transition to cyclobenzaprine, a muscle relaxant with demonstrated benefit in FMS. She was also referred to a pain psychologist, who initiated cognitive-behavioral therapy and taught her how to utilize relaxation techniques and develop coping skills. At the same time, she agreed to restart a daily exercise regimen, which included flexibility and strength training along with an emphasis on aerobic training, and to keep an exercise diary. Because many patients do not respond adequately to exercise treatment because of poor compliance secondary to pain, she began her aerobic training with simple walking. PHARMACOLOGIC TREATMENT Pregabalin was started, with the dose initially titrated to 225 mg twice a day, and then increased to 300 mg twice a day. The attempted switch to cyclobenzaprine 5 mg twice a day was changed to 8 mg twice a day, and eventually increased to 10 mg 3 times per day. The patient was able to discontinue most of her benzodiazepine, but continued to take clonazepam 0.5 mg at bedtime. On a similar note, she was also unable to 120 taper off opioids completely, but did manage an approximately 90% decrease in her total dosage to fentanyl patch 12.5 µg per hour plus a single hydrocodone/acetaminophen tablet per day as needed. Over the next 3 months, she reported a 25% reduction in symptoms, with resolution of allodynia and redevelopment of the classic FMS pain pattern. However, insomnia recurred with the tapering of opioids and benzodiazepines. At this point, after “buy in” from her psychologist and primary care physician, she was switched from sertraline to duloxetine 60 mg orally at bedtime because the latter has shown benefit in alleviating pain and improving sleep in FMS. As her depression resolved, she began working part-time for a medical billing company. Protriptyline, a tricyclic antidepressant that can reduce drowsiness, was added when she noted that daytime fatigue and lethargy were interfering with her productivity at work. Dextromethorphan, an oral N-methyl-D-aspartate receptor antagonist, was also added after a positive intravenous ketamine infusion test.38 C URRENT STATUS She reports a 60% reduction in pain and appears to be doing well. She received a promotion to assistant manager, lost 10 pounds, and has started dating again. REFERENCES 1. Roizenblatt S, Moldofsky H, Benedito-Silva AA, Tufik S. Alpha sleep characteristics in fibromyalgia. Arthritis Rheum. 2001;44:222-230. 2. Harding SM. Sleep in fibromyalgia patients: subjective and objective findings. Am J Med Sci. 1998;315:367-376. 3. Theadom A, Cropley M. Dysfunctional beliefs, stress and sleep disturbance in fibromyalgia. Sleep Med. 2008;9:376-381. 4. Moldofsky H, Scarisbrick P, England R, Smythe H. Musculoskeletal symptoms and non-REM sleep disturbance in patients with “fibrositis syndrome’ and healthy subjects. Psychosom Med. 1975;37:341-351. 5. Gold AR, Dipalo F, Gold MS, Broderick J. Inspiratory airflow dynamics during sleep in women with fibromyalgia. Sleep. 2004;27:459-466. 6. Rizzi M, Sarzi-Puttini P, Atzeni F, et al. Cyclic alternating pattern: a new marker of sleep alteration in patients with fibromyalgia? J Rheumatol. 2004;31:1193-1199. 7. Martínez-Lavín M, Hermosillo AG, Rosas M, Soto ME. Circadian studies of autonomic nervous balance in patients with fibromyalgia: a heart rate variability analysis. Arthritis Rheum. 1998;41:1966-1971. 8. Shah MA, Feinberg S, Krishnan E. Sleep-disordered breath- Vol. 9, No. 4 n December 2009 PROCEEDINGS ing among women with fibromyalgia syndrome. J Clin Rheumatol. 2006;12:277-281. 9. Clauw DJ, Crofford LJ. Chronic widespread pain and fibromyalgia: what we know, and what we need to know. Best Pract Res Clin Rheumatol. 2003;17:685-701. 10. Aaron LA, Buchwald D. Chronic diffuse musculoskeletal pain, fibromyalgia and co-morbid unexplained clinical conditions. Best Pract Res Clin Rheumatol. 2003;17:563-574. 11. Wasan AD, Wooton J, Jamison RN. Dealing with difficult patients in your pain practice. Reg Anesth Pain Med. 2005:30:184-192. 12. Wolfe F, Smythe HA, Yunus MB, et al. The American College of Rheumatology 1990 Criteria for the Classification of Fibromyalgia. Report of the Multicenter Criteria Committee. Arthritis Rheum. 1990;33:160-172. 13. Watson NF, Buchwald D, Goldberg J, et al. Neurologic signs and symptoms in fibromyalgia. Arthritis Rheum. 2009;60:2839-2844. 14. Gjesdal S, Haug K, Ringdal P, et al. Sickness absence with musculoskeletal or mental diagnoses, transition into disability pension and all-cause mortality: a 9-year prospective cohort study. Scand J Public Health. 2009;37:387-394. 15. Silverman S, Dukes EM, Johnston SS, et al. The economic burden of fibromyalgia: comparative analysis with rheumatoid arthritis. Curr Med Res Opin. 2009;25:829-840. 16. Greenberg PE, Leong SA, Birnbaum HG, Robinson RL. The economic burden of depression with painful symptoms. J Clin Psychiatry. 2003;64(suppl 7):17-23. 17. Robinson RL, Birnbaum HG, Morley MA, et al. Depression and fibromyalgia: treatment and cost when diagnosed separately or concurrently. J Rheumatol. 2004;31:1621-1629. 18. Wassem R, Hendrix TJ. Direct and indirect costs of fibromyalgia to patients and their families. J Orthoped Nurs. 2003;7:26-31. 19. Robinson RL, Birnbaum HG, Morley MA, et al. Economic cost and epidemiological characteristics of patients with fibromyalgia claims. J Rheumatol. 2003;30:1318-1325. 20. Berger A, Dukes E, Martin S, et al. Characteristics and healthcare costs of patients with fibromyalgia syndrome. Int J Clin Pract. 2007;16:1498-1508. 21. Hughes G, Martinez C, Myon E, et al. The impact of a diagnosis of fibromyalgia on health care resource use by primary care patients in the UK: an observational study based on clinical practice. Arthritis Rheum. 2006;54:177-183. 22. Bennett RM, Jones J, Turk DC, et al. An internet survey of 2,596 people with fibromyalgia. BMC Musculoskelet Disord. 2007;8:27. 23. Okifuji A, Bradshaw DH, Olson C. Evaluating obesity in fibromyalgia: neuroendocrine biomarkers, symptoms, and functions. Clin Rheumotol. 2009;28:475-478. Johns Hopkins Advanced Studies in Medicine n 24. Pamuk ON, Dönmez S, Cakir N. The frequency of smoking in fibromyalgia patients and its association with symptoms. Rheumatol Int. 2009;29:1311-1314. 25. Wolfe F, Hawley DJ. Psychosocial factors and the fibromyalgia syndrome. Z Rheumatol. 1998;57(suppl 2):88-91. 26. National Invisible Chronic Illness Awareness Week. Fact Sheet and Statistics About Chronic Illness. Available at: http://www.restministries.org/invisibleillness/statistics.htm. Accessed November 29, 2009. 27. Dell DD. Getting the point about fibromyalgia. Nursing. 2007;37:61-64. 28. Dobkin PL, De Civita M, Bernatsky S, et al. Does psychological vulnerability determine health-care utilization in fibromyalgia? Rheumatology (Oxford). 2003;42:1324-1331. 29. Shleyfer E, Jotkowitz A, Karmon A, et al. Accuracy of the diagnosis of fibromyalgia by family physicians: is the pendulum shifting? J Rheumatol. 2009;36:170-173. 30. US Department of Health and Human Services. Office of Women’s Health. Health Insurance and Women. Available at: http://www.womenshealth.gov/faq/health-insurancewomen.cfm. Accessed November 21, 2009. 31. Doty MM, Collins SR, Rustgi SD, Nicholson JL. Out of options: why so many workers in small businesses lack affordable health insurance, and how health care reform can help. Findings from Commonwealth Fund Biennial Health Insurance Survey, 2007. Issue Brief (Commonw Fund). 2009;67:1-22. 32. Callahan LF, Smith WJ, Pincus T. Self-report questionnaires in five rheumatic diseases: comparisons of health status constructs and associations with formal education level. Arthritis Care Res. 1989;2:122-131. 33. Mas AJ, Carmona L, Valverde M, et al. Prevalence and impact of fibromyalgia on function and quality of life in individuals from the general population: results from a nationwide study in Spain. Clin Exp Rheumatol. 2008;26:519-526. 34. Bergman S. Psychosocial aspects of chronic widespread pain and fibromyalgia. Disabil Rehabil. 2005;27:675-683. 35. Neumann L, Buskila D. Ethnocultural and educational differences in Israeli women correlate with pain perception in fibromyalgia. J Rheumatol. 1998;25:1369-1373. 36. Mäkelä M, Heliövaara M. Prevalence of primary fibromyalgia in the Finnish population. BMJ. 1991;303:216-219. 37. Waddell G, McCulloch JA, Kummel E, Venner RM. Nonorganic physical signs in low-back pain. Spine. 1980;5:117-125. 38. Cohen SP, Verdolin MH, Chang AS, et al. The intravenous ketamine test predicts subsequent response to an oral dextromethorphan treatment regimen in fibromyalgia patients. J Pain. 2006;7:391-398. 121