Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
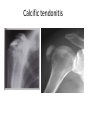
Pattern recognition of the shoulder By Florence Davidson SORSA-RSSA 2013 Contents • A method and terminology used for pattern recognition of the appendicular skeleton • Overview normal anatomy: shoulder • Common projections for trauma • Interactive clicker session: shoulder & cervical spine Cardinal rules • Correct patient (identity and anatomy) • Sufficient diagnostic quality (anatomy demonstrated, exposure, whether repeat or supplementary views needed) • Radiographer comments must only be made on visible radiographic appearances- if the medial end of the clavicle is omitted from an AP shoulder projection, it is impossible to comment on the normality of the SC joint. • All images relating to the examination must be viewed (Snaith: 2005) Pattern recognition of the skeleton: 1. Bones Trace around the cortex (edge) of every bone The bony outline should be smooth (any breaks in the presence of trauma= a fracture) Check the trabecular pattern which should have a smooth and regular appearance- look for any black (lucent) or white (sclerotic) lines which may indicate separation or overlapping of bone fragments. Pattern recognition of the skeleton: 2. Joints • Look carefully at all the components of a joint for alignment of the articular surfaces, in particular the edge of joints. Pattern recognition of the skeleton: 3. Soft tissues • Check for any evidence of soft tissue swelling, disruption of fat planes or presence of any foreign material. Sometimes soft tissue changes may be the only clue to subtle injury. (Snaith: 2005) Review approach Review approach Features Anatomy and laterality Identify abnormality Describe fracture type Intra/extra-articular Position Displacement/angulation-direction Once you have the elements above, assemble in a succinct way (Snaith: 2005) Paediatric fractures • Many variations • Differ from adults due to elasticity of children’s bones • Radius and ulna most commonly injured with buckle (Torus #) • When # involves epiphyseal plate, Salter Harris classification is used • Sufficient for radiographers to ID # as metaphyseal or epiphyseal Some “terms”: • • • • • • • • Cortical bone (cortex) Periosteum Trabeculae Mineralisation Intra, extra and periarticular Fat pad Lucent Sclerotic Anatomy of the shoulder • The glenohumearal joint has a great range of motion. • The glenoid fossa is small and the joint capsule is lax making it prone to subluxation and dislocation. Robin Smithuis and Henk Jan van der Woude Anterior view Posterior view Normal appearance • AP • Humeral head not symmetrical • Looks like the head of a walking stick • The articular surfaces of the humerus and the glenoid parallel to each other. Raby et al: 1995 Normal AC JOINT: 3-5mm (up to 7mm) Normal shoulder: internal rotation Normal shoulder: external rotation Figure 4.3. The Y view. The humeral head overlies the centre of the glenoid (G). The Y is formed by the j junction of the scapular \ blade, coracoid (C) and acromion (A). Raby et al: 1995 Raby et al: 1995 http://www.wikiradiography.com/page/I maging+Shoulder+Dislocations?t=anon Shoulder pathologies • Dislocations: Anterior most common • Subluxations: AC joint • Fractures: Clavicle # most common in children, scapula # are rare, elderly commonly # proximal humerus • Soft tissue: calcification of tendons Dislocations: Anterior (most common) http://www.wikiradiography.com http://www.wikiradiography.com Dislocations: Posterior (only 5%) Raby et al:1995 Figure 4.19. Posterior dislocation. Y view. The! humeral head lies behind the glenoid (the centra of the Y). http://www.wikiradiography.com/photo/8178 625/poaterior+shoulder+dislocation http://image.wikifoundry.com/image/1/KikuxU 0zw9CTWoMCXU5HIg241164 Calcific tendonitis Pattern recognition of the cervical spine Contents: • • • • • • • Normal anatomy & radiographic anatomy Fracture prevalence Projections & pattern recognition Soft tissue structures Pathomechanics Stability Classification of trauma Fracture prevalence • # C5/C6 common (most injuries due to hyper flexion) • # infrequent in children <8yrs (likely to involve C1/C2) • Neurological damage occurs in about 40% of cases (due to burst # or facet joint dislocations) (Nunn) • One third of injuries occur at the level of C2, and one half of injuries occur at the level of C6 or C7. (http://www.radiologyassistant.nl/en/p4902153514 6c5/spine-cervical-injury.html#i49021535369a6 Ligaments: Although not demonstrated radiographically, disruptions are evidenced by alignment and location of the osseous structures supported by the ligaments (Nunn) McConnell et al: 2005 McConnell et al: 2005 An injury is considered unstable if 2 of the 3 columns are disrupted A patient with a suspected C/Spine injury can be cleared: http://www.radiologyassistant.nl/en/p490215 35146c5/spine-cervicalinjury.html#i49134bdbb8298 Projection: Lateral Projections: Lateral • Most detectable abnormalities will be visible on lateral view. • Trace 3 anatomical lines: Projection: “Swimmers” • To assess alignment of C7 with T1: “Is there subluxation?” Soft tissue signs • The retropharyngeal/preveretebral soft tissues can provide signs of cervical spine injury. • This image demonstrates normal preveretebral soft tissues: C2 (Black arrows): The prevertebral soft tissues at C2 should measure less than 7mm or less than 50% of the width of the adjacent vertebral body C6 (White arrows): The prevertebral soft tissues at C6 should measure less than 22mm. Or not be greater than the width of the adjacent vertebral body. These are guides only and must be interpreted in the context of bony appearances, mechanism of injury and clinical signs. http://www.wikiradiography.com/page/Soft+Tissue+ Signs-+Cervical+Spine Lateral: • Vertebral bodies and intervertebral discs should be of uniform height at both the anterior and posterior parts (3mm difference can indicate wedge compression fracture) Lateral: The normal relationship between the anterior arch of C1 and the odontoid peg: not >3mm in the adult Raby et al Projections: AP • Assess superior & inferior end plates, spinous processes, lateral masses SP in straight line (?bifid) Raby AP Malalignment of SP?Facet joint dislocation Raby AP: • Distance between SP should be equal Anterior cervical dislocation Raby et al: 1995: http://www.radiologyassistant.nl/en/p49021535146c5/spinecervical-injury.html#i49021535369a6 Projection: AP open mouth (C1/C2) • Lateral masses of C1 should not overhang lateral masses of C2 (Burst #?) • Symmetric space between odontoid peg & lateral masses of C1 (? Rotation) • Artefacts mimicking #? Jefferson fracture (burst fracture of C1) http://www.scientificspine.com/spinal-diseases/atlas-fracture.html Axis (C2) • Odontoid peg • Hangman’s fracture http://www.radiologyassistant.nl/en/p49021535146 c5/spine-cervical-injury.html#i49021535369a6 McConnell et al: 2005 Teardrop extension fracture Wedge compression fracture www.mdguidelines.com Fracture spinous process Raby et al: 1995: 106 References: • • • • • • • • • • • Bontrager, K & Lampignano. 2005. Textbook of Radiographic Positioning and Related Anatomy. St Louis: Elsevier Mosby Mc Connell, J; Eyres, R & Nightingale, J. 2005. Interpreting Trauma Radiographs. Oxford: Blackwell publishing Moeller, T. 1999. Normal findings in Radiography. New York: Thieme Stuttgart Raby, N; Berman, L 7 De Lacey, G. 1995. Accident & Emergency Radiology, A survival guide. London: WB Saunders Snaith, B. 2005. Radiographer comments in practice: Describing injuries. Synergy: December www.ceessentials.net www.imageinterpretation.co.uk http://www.radiologyassistant.nl/ www.radiopaedia.org www.wikiradiography.com www.xray2000.co.uk