Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Cryptosporidiosis wikipedia , lookup
Sexually transmitted infection wikipedia , lookup
West Nile fever wikipedia , lookup
Trichinosis wikipedia , lookup
Brucellosis wikipedia , lookup
Chagas disease wikipedia , lookup
Neonatal infection wikipedia , lookup
Eradication of infectious diseases wikipedia , lookup
Onchocerciasis wikipedia , lookup
Human cytomegalovirus wikipedia , lookup
Middle East respiratory syndrome wikipedia , lookup
Marburg virus disease wikipedia , lookup
Dirofilaria immitis wikipedia , lookup
Hepatitis C wikipedia , lookup
Leptospirosis wikipedia , lookup
African trypanosomiasis wikipedia , lookup
Hepatitis B wikipedia , lookup
Leishmaniasis wikipedia , lookup
Sarcocystis wikipedia , lookup
Visceral leishmaniasis wikipedia , lookup
Fasciolosis wikipedia , lookup
Coccidioidomycosis wikipedia , lookup
Schistosomiasis wikipedia , lookup
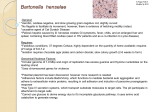
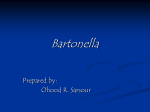
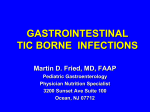
951 Granulomatous Hepatitis and Necrotizing Splenitis Due to Bartonella henselae in a Patient with Cancer: Case Report and Review of Hepatosplenic Manifestations of Bartonella Infection Thomas E. Liston and Jane E. Koehler From the Division of Infectious Disease, Department of Pediatrics, Kaiser Permanente Medical Center, Martinez, California; and the Division of Infectious Disease, Department of Medicine, University of California, San Francisco, California Bartonella (formerly Rochalimaea [1]) infection often appears as skin lesions known as bacillary angiomatosis (BA) but may affect the liver (bacillary peliosis hepatis; BP) and spleen (bacillary splenitis) in both immunocompromised and immunocompetent hosts [2]. Two bacterial agents have been cultured directly from specimens of BA lesions: Bartonella henselae and Bartonella quintana [3]. The occurrence of bartonella infection during chemotherapy for cancer was first reported in 1992; in that pediatric case and in two subsequent cases involving adults, the vascular proliferative manifestation of bartonella infection was described [4-6]. This report details an adult patient receiving chemotherapy for cancer in whom granulomatous visceral disease due to B. henselae developed; we also review hepatosplenic manifestations of bartonella infection. Case Report A 54-year-old woman was admitted to the surgical service of Kaiser Permanente Medical Center (Martinez, CA) in September 1992 after an annual mammogram showed a mass (10 X 4 mm) in the left breast. Excisional biopsy revealed a moderately well-differentiated infiltrating ductal carcinoma. The patient received three courses of chemotherapy with cy- Received 6 September 1995; revised 15 December 1995. Financial support: Dr. Koehler received grant support from the NIH (R29AI36075) and the University wide AIDS Research Program, University of California. Dr. Koehler is a Pew Scholar in the Biomedical Sciences. Reprints or correspondence: Dr. Thomas E. Liston, Department of Pediatrics, Kaiser Permanente Medical Center, 200 Muir Road, Martinez, California 94553-4696. Clinical Infectious Diseases 1996;22:951-7 © 1996 by The University of Chicago. All rights reserved. 1058-4838/96/2206-0007$02.00 toxan, adriamycin, and 5-fluorouracil sequentially with radiation therapy for 6 weeks and then a second cycle of three planned courses of chemotherapy; each course of chemotherapy was 28 days. The patient was again admitted to the hospital in March 1993 because of fever that developed 4 weeks after the fifth course of chemotherapy. Her temperature rose to 105.1 OF (40.6°C) and remained at this level for several days. She had never received a blood transfusion and did not consent to HIV antibody testing. The patient was treated empirically with ceftriaxone and gentamicin. Skin tests for tuberculosis and coccidioidomycosis were negative, as were five blood cultures. The average complete leukocyte count was 5,000/mm3 (5 X 109/1), with 70%80% polymorphonuclear cells. A gallium scan 10 days after admission showed increased uptake in the spleen. A CT. scan done on day 14 showed multiple hypodense lesions in the spleen and a few similar lesions in the liver (figure 1). A bone marrow biopsy showed only hypocellularity. The patient had been raised in Louisiana and recalled drinking fresh milk from cows there. She had traveled extensively throughout the world but had not traveled recently and had never visited South America or the Andes Mountains. She disliked cats and denied any recent contact with a cat or dog but visited people with pets and could have been bitten by fleas. Disseminated Mycobacterium tuberculosis infection was considered the most likely diagnosis, and brucellosis was considered less likely. The antibiotics prescribed earlier were withdrawn; the patient was treated with isoniazid for 13 days and pyrazinamide for 5 days, and administration of rifampin was continued. Splenectomy was recommended for definitive diagnosis. At laparotomy no lesions were noted on the surface of the liver, but a biopsy was performed, along with biopsy of a lymph node. The spleen was removed. Downloaded from http://cid.oxfordjournals.org/ by guest on September 9, 2014 Bacillary angiomatosis and the related disorders of bacillary peliosis hepatis and bacillary splenitis are manifestations of infection with Bartonella henselae and Bartonella quintana in immunocompromised persons. B. henselae infection, but not B. quintana infection, is linked to contact with cats and is presumed to cause visceral cat-scratch disease. We report a case of visceral infection by B. henselae in an adult patient with cancer who was receiving chemotherapy and had had no contact with a cat or dog. The patient-whose illness was eventually diagnosed on the basis of findings of histologic, polymerase chain reaction, and serological studies-was treated with doxycycline and rifampin, and the infection resolved. In addition, 41 cases of documented or suspected bartonella infection of the liver, spleen, or both in immunocompetent or immunocompromised hosts are reviewed. 952 Liston and Koehler em 1996;22 (June) Figure 1. An abdominal CT scan with oral and intravenous contrast showing multiple small, hypodense, round lesions in the spleen (arrows) and liver of a patient with cancer. Figure 2. A photograph of the gross anatomy of the spleen shows heterogeneously sized white nodules. infection [7], the diagnosis of bartonella infection was considered. However, Warthin-Starry silver stains performed at the pathology department at Kaiser Permanente Medical Center and the department of dermatology at the University of California (San Francisco) did not initially reveal the presence of bacteria. Microbiology. A special blood culture specimen was drawn with use of the Isostat Isolator tube (Wampole Laboratories, Cranbury, NJ). Cultures were negative, although antibiotic treatment had been discontinued several days before the culture specimens were drawn. Cultures of the spleen were negative for fungi, Brucella species, and acid-fast bacilli. Serology and peR. A CF test for Brucella was negative (< 1:4). Although the initial test for B. henselae was negative, a second specimen drawn 99 days later revealed IgO antibodies to B. henselae (> 120 EIA units; normal reference value, < 12) as well as IgM antibodies (79 EIA units), as determined at Specialty Laboratories (Santa Monica, CA). Serology samples were collected and sent to the Centers for Disease Control and Prevention (CDC). Immunofluorescent antibody assays [8] (performed at the CDC's Rickettsial Disease Laboratory) of samples collected on day 21 showed antibodies to B. henselae (1 :512) and B. quintana (> 1: 1,024); assays of sera collected during the patient's convalescence (day 35) showed antibody titers of > I: I,024 for B. henselae and > I: I,024 for B. quintana. Ultimately, Warthin-Starry staining of splenic tissue at the Armed Forces Institute of Pathology (Washington, D.C.) revealed a "few clumps ofsilvered bacilli in one granuloma. . . characteristic of cat scratch disease" (figure 3). Splenic tissue obtained at Downloaded from http://cid.oxfordjournals.org/ by guest on September 9, 2014 Pathology. The spleen surface was covered with grayishwhite nodules that were 2-5 mm in size (figure 2). Histopathologic examination showed numerous necrotizing and caseating granulomas, which stained negative for acid-fast bacilli and did not produce a periodic acid-Schiff reaction; examination of a nearby abdominal lymph node and one of several small nodules obtained by liver biopsy revealed the same histopathologic characteristics. Because similar nodules had been found in the spleen of a patient with AIDS-related complex and presumed bartonella em 1996;22 (June) Hepatosplenic Bartonella Infections 953 Figure 3. A Warthin-Starry silver stain of the spleen showing darkly staining bacilli (arrows) consistent with Bartonella (original magnification, X 400). Discussion Human bartonella infections have only recently been reported in the United States and were initially described as vascular proliferative lesions (now known as BA) in HIVinfected patients [10). Other syndromes reported in the past several years that have been caused by Bartonella species include relapsing fever and bacteremia (in both immunocompromised and immunocompetent hosts [11, 12]) and endocarditis [13, 14). Recently, an infection first described many years ago, cat-scratch disease (CSD), has been attributed to B. henselae. This disease is usually self-limiting, develops as a complication of a cat scratch, and manifests as a local, necrotizing lymphadenitis in the immunocompetent host [15, 16]. B. henselae has been cultured directly from specimens of vascular proliferative BA lesions [3] and necrotizing granulomatous CSD lymph nodes [16]. Thus, the histopathologic manifestations of infection with B. henselae can be strikingly different and are apparently related to the degree of immunocompromise in the host. Some patients whose immune systems are not severely compromised appear to have disseminated granulomatous lesions, constitutional symptoms, and a longer and more severe disease course than that of CSD. Our patient had disseminated B. henselae disease, but whether the severity of her illness was related to the chemotherapy for breast cancer is unknown. Bartonella species-associated lesions ofthe liver and spleen can be categorized as one of two distinct types on the basis of histopathologic findings: vascular proliferative lesions or necrotizing granulomatous lesions. Vascular proliferative disease, or BP, differs histopathologically from BA and is characterized by multiple, cystic, blood-filled spaces in addition to foci of necrosis [17]. A fibromyxoid stroma is often present and contains clumps of Bartonella bacilli and a mixed inflammatory infiltrate [17]. As with BA lesions, BP lesions are more common in HIV-infected patients. Downloaded from http://cid.oxfordjournals.org/ by guest on September 9, 2014 splenectomy was sent to the CDC, where it was evaluated further. Bacterial DNA was extracted from the splenic tissue; the template DNA was amplified and then hybridized by dot blotting with use of primers and probes, as previously described by Anderson et al. (9). The probes are specific for differentiation of B. quintana from B. henselae, and the species infecting this patient was determined to be B. henselae. Treatment and outcome. Treatment with erythromycin for suspected bartonella infection was begun on day 22. The patient was unable to tolerate the drug because of gastrointestinal disturbance, and it was replaced with doxycycline (100 mg twice daily) and rifampin (600 mg daily) on day 27. The patient became afebrile the next day and was discharged 30 days after admission. Cultures for M. tuberculosis were negative. The patient continued to do well after completing 4 months of treatment with oral doxycycline (100 mg b.i.d.) and rifampin (600 mg daily). A follow-up CT scan done on day 54, ~ 1 month after splenectomy, showed resolution ofthe liver lesions. Eighteen months following completion of chemotherapy for breast cancer, no sign of recurrence of cancer was evident. The patient declined a sixth course of chemotherapy, and there was no evidence of bartonella infection during nearly 3 years of follow-up. 954 Liston and Koehler 1996;22 (June) hybridization probes, permitted rapid differentiation of the two species. The source of bartonella infections has been intensively investigated recently. A large case-control study [24] of 48 patients (5 immunocompetent patients, 1 transplant recipient, and 42 HIV-infected patients) revealed that BA and BP were significantly linked to owning a cat or being bitten or scratched by a cat. Another study [25] showed a statistically significant association between CSD and owning a kitten or being scratched by a kitten. Further study [26] identified the domestic cat as a major reservoir of B. henselae infection: all seven cats of four patients with BA due to B. henselae had B. henselae bacteremia. In addition, 41 % of pet cats and cats at animal shelters in the San Francisco Bay area whose blood specimens were cultured had B. henselae bacteremia. Viable B. henselae was isolated from fleas combed from one of the cats with bacteremia [26], which indicates that fleas might serve as a vector of B. henselae. Our patient had B. henselae infection yet disliked cats and denied contact with them. Thus, the source of her infection remains unknown. Bartonella infections in patients with BA or BP respond dramatically to treatment with erythromycin or doxycycline [2]. Treatment of bartonella infection in immunocompetent people with CSD and local lymphadenitis has not been studied systematically, and because this infection is self-limiting, treatment may not be warranted for such patients. However, treatment is appropriate for patients with severe, disseminated, granulomatous disease, and for adults it should include administration of erythromycin or doxycycline. Gentamicin or rifampin has also been used successfully to treat both BA and CSD [2, 15], but neither is recommended as single-agent therapy for seriously ill patients [2]. Our patient responded rapidly to treatment with doxycycline and rifampin, and the hepatic lesions and systemic symptoms resolved completely. For immunocompromised patients with disseminated disease, including BP, treatment should last at least 3 months; an adequate duration of treatment for immunocompetent patients is unknown, but treatment probably should last at least I month. Review of Previous Cases Twenty-two articles that described patients with presumed hepatic or splenic disease due to bartonella infection were reviewed [7, 17, 23, 27-45]. These reports contained sufficient clinical data to confirm the diagnosis for 41 patients on the basis of at least three ofthe following 10 criteria: consistent radiographic evidence on CT scan films, ultrasonographic scan films, or both; compatible gross pathology of multiple nodules; compatible histologic findings of granulomas or BP, with or without necrosis; positive Warthin-Starry silver stains; positive PCR for Bartonella species; successful culture of B. henselae; serological increase in titers of antibody to Bartonella species; electron microscopic findings compatible with Bartonella species; positive CSD skin test results; Downloaded from http://cid.oxfordjournals.org/ by guest on September 9, 2014 The second type of hepatic pathological abnormality associated with bartonella infection resembles that found in the lymph nodes of patients with CSD: necrotizing granulomas with leukocytic infiltration, palisading histiocytes, giant cells, and sometimes stellate abscesses [18]. These histopathologic features are seen most commonly in immunocompetent hosts. The hepatic and splenic lesions of both histopathologic types are often multiple and can appear as hypoechoic or low-attenuation lesions scattered throughout the hepatic or splenic parenchyma on ultrasonographic or CT scans [19]. However, numerous other infectious and noninfectious conditions in either immunocompetent or immunocompromised individuals may appear identical, including abscesses due to fungi, protozoa, and bacteria other than Bartonella species. In addition, the CT appearance ofcancers such as lymphoma and Kaposi's sarcoma can be indistinguishable from BP in HIV-infected patients. The diagnosis of bartonella infection must be established by one or more means: histopathologic examination of biopsy specimens, serological evaluation, microbiological culture, and/or use of PCR to detect Bartonella DNA in clinical specimens. The most accessible diagnostic technique for a patient with multiple hypodense lesions of the liver is biopsy. The risk of hemorrhage from percutaneous liver biopsy for a patient with BP remains theoretical, but viewing the liver directly during biopsy may reduce this risk. The biopsied tissue should be examined with hematoxylin-eosin staining, which demonstrates either granulomatous hepatitis or peliosis hepatis. WarthinStarry staining reveals silver-staining bacilli in most cases of BP because the number of bacteria present in lesions is much greater in immunocompromised patients. However, in granulomatous hepatic lesions the bacilli are much more difficult to find, and in our case the difficulty in visualizing organisms may have been related to administration of antibiotic agents in the 2 weeks before splenectomy. Serological tests based on immunofluorescence [8] or EIA [20] are now available. Testing of paired sera confirmed our patient's bartonella infection, but the Bartonella species that caused the infection could not be determined serologically; in fact, the titer of antibodies to B. quintana was higher than that to B. henselae, even though PCR showed B. henselae infection. Culture of Bartonella organisms from tissue or blood is difficult but can be done with use of chocolate agar or heart infusion agar with 5% rabbit blood [3, 11]. Isolates can be identified by means of the Microscan Rapid Anaerobe panel (Baxter Diagnostics, Deerfield, IL), which will distinguish between B. henselae and B. quintana [21]. Definitive identification of Bartonella species requires molecular characterization with citrate synthase PCR- restriction fragment length polymorphism analysis of isolates [22] or 16S rRNA gene amplification and sequencing [3, 23]. In a study described by Anderson et al. [9], a PCR assay (utilized on our patient's tissue) using degenerate primers to allow amplification of a 414-bp fragment of DNA from B. henselae and B. quintana was developed. Internal oligonucleotides, used as em Downloaded from http://cid.oxfordjournals.org/ by guest on September 9, 2014 956 Liston and Koehler Summary This report summarizes the case of a cancer patient with a severe febrile illness and visceral B. henselae disease and reviews the literature on hepatosplenic disease related to presumed bartonella infection. For our patient, the histopathologic appearance was that of necrotizing granulomatous disease of the spleen without angiomatous changes. Bartonella infection must be considered as a cause of fever in patients with cancer who are receiving chemotherapy as well as in patients who are immunocompromised because of HIV infection or organ transplantation. Acknowledgments At the Viral and Rickettsial Zoonoses Branch of the CDC, Mary Jane Schmidt, M.D., arranged for serological and PCR testing of spleen tissue obtained through biopsy; Judy Cooper, P.A., performed the serological testing; and Burt Anderson, Ph.D., performed the PCR studies. Investigators at the Armed Forces Institute of Pathology (Washington, DC) performed the Warthin-Starry silver staining, and the Medical Editing Department of Kaiser Foundation Research Institute (Oakland, CA) provided editorial assistance. References 1. Brenner DJ, O'Connor SP, Winkler HR, Steigervvalt AG. Proposals to unify the genera Bartonella and Rochalimaea, with descriptions of Bartonella quintana comb. nov., Bartonella vinsonii comb. nov., Bartonella henselae comb. nov., and Bartonella elizabethaecomb. nov.; and to remove the family Bartonellaceae from the order Rickettsiales. Int J Syst BacterioI1993;43:777-86. 1996;22 (June) 2. Koehler JE, Tappero JW. Bacillary angiomatosis and bacillary peliosis in patients infected with human immunodeficiency virus. Clin Infect Dis 1993; 17:612-24. 3. Koehler JE, Quinn FD, Berger TG, LeBoit PE, Tappero JW. Isolation of Rochalimaea species from cutaneous and osseous lesions of bacillary angiomatosis. N Engl J Med 1992;326:1625-31. 4. Myers SA, Prose NS, Garcia JA, Wilson KH, Dunsmore KP, Kamino H. Bacillary angiomatosis in a child undergoing chemotherapy. J Pediatr 1992; 121:574-8. 5. Torok L, Viragh SZ, Borka I, Tapai M. Bacillary angiomatosis in a patient with lymphocytic leukaemia. Br J DermatoI1994; 130:665-8. 6. Mulvany NJ, Billson VR. Bacillary angiomatosis of the spleen. Pathology 1993;25:398-401. 7. Delahoussaye PM, Osborne BM. Cat-scratch disease presenting as abdominal visceral granulomas. J Infect Dis 1990; 161 :71-8. 8. Regnery RL, Olson JG, Perkins BA, Bibb W. Serological response to "Rochalimaea henselae" antigen in suspected cat-scratch disease. Lancet 1992;339:1443-5. 9. Anderson B, Sims K, Regnery R, et a!. Detection of Rochalimaea henselae DNA in specimens from cat scratch disease patients by PCR. J Clin Microbiol 1994; 32:942-8. 10. Stoler MH, Bonfiglio TA, Steigbigel RT, Pereira M. An atypical subcutaneous infection associated with acquired immune deficiency syndrome. Am J Clin PathoI1983;80:714-8. 11. Slater LN, Welch DF, Hensel D, Coody DW. A newly recognized fastidious gram-negative pathogen as a cause of fever and bacteremia. N Engl J Med 1990;323:1587-93. 12. Lucey D, Dolan MJ, Moss CW, et a!. Relapsing illness due to Rochalimaea henselae in immunocompetent hosts: implication for therapy and new epidemiological associations. Clin Infect Dis 1992; 14:683-8. 13. Spach DH, Callis KP, Paauw DS, et al. Endocarditis caused by Rochalimaea quintana in a patient infected with human immunodeficiency virus. J Clin Microbiol 1993; 31 :692-4. .14. Daly JS, Worthington MG, Brenner DJ, et al. Rochalimaea elizabethae sp. nov. isolated from a patient with endocarditis. J Clin Microbio1 1993; 31 :872-81. 15. Margileth AM. Antibiotic therapy for cat-scratch disease: clinical study of therapeutic outcome in 268 patients and a review of the literature. Pediatr Infect Dis J 1992; 11 :474-8. 16. Dolan MJ, Wong MT, Regnery RL, et a1. Syndrome of Rochalimaea henselae adenitis suggesting cat-scratch disease. Ann Intern Med 1993; 118:331-6. 17. Perkocha LA, Geaghan SM, Yen TSB, et a1. Clinical and pathological features ofbacillary peliosis hepatis in association with human immunodeficiency virus infection. N Eng1 J Med 1990;323:1581-6. 18. Schwartzman WA. Infections due to Rochalimaea: the expanding clinical spectrum. Clin Infect Dis 1992; 15:893-902. 19. Wyatt SH, Fishman EK. Hepatic bacillary angiomatosis in a patient with AIDS. Abdom Imaging 1993; 18:336-8. 20. Barka NE, Hadfield T, Patnaik M, Schwartzman WA, Peter JB. EIA for detection of Rochalimaea henselae-reactive IgG, IgM, and IgA antibodies in patients with suspected cat-scratch disease [letter]. J Infect Dis 1993; 167:1503-4. 21. Welch DF, Hensel DM, Pickett DA, San Joaquin VH, Robinson A, Slater LN. Bacteremia due to Rochalimaea henselae in a child: practical identification of isolates in the clinical laboratory. J Clin MicrobioI1993;31: 2381-6. 22. Regnery RL, Anderson BE, Clarridge JE III, Rodriguez-Barradas MC, Jones DC, Carr JR. Characterization of a novel Rochalimaea species, R. henselae sp. nov., isolated from blood of a febrile, human immunodeficiency virus-positive patient. J Clin Microbiol 1992:30:265-74. 23. Reiman DA, Loutit JS, Schmidt TM, Falkow S, Tompkins LS. The agent ofbacillary angiomatosis: an approach to the identification of uncultured pathogens. N Engl J Med 1990;323:1573-80. 24. Tappero JW, Mohle-Boetani J, Koehler JE, et a1. The epidemiology of bacillary angiomatosis and bacillary peliosis. JAMA.·1993;269:770-5. Downloaded from http://cid.oxfordjournals.org/ by guest on September 9, 2014 (25 cases). In addition, results were abnormal for liver-spleen scanning and CT scanning in 1 case, for a gallium study and ultrasonographic studies in another case, and for MRI and CT in a third case. Including our case, gross pathological findings in 21 cases of granulomatous bartonella infection included the typical small, gray-white nodules or larger nodules. In cases of the peliotic form of infection, numerous cystic blood-filled spaces were evident. Histologic findings included granulomas (occasionally caseating) in 21 cases, 15 of which involved immunocompetent hosts; BP (vascular proliferative abnormalities) in 12 cases, all of which involved immunocompromised hosts (two had granulomas and BP); and inflammation, necrotizing lesions, or abscess in 6 cases. The affected organs were the liver and spleen in 22 cases, the liver only in 16, and the spleen only in 4. Warthin-Starry silver stains were positive in 27 cases, and electron microscopy was positive in 13. PCR was positive in six cases, and cultures were positive for Bartonella species in one case. Serological studies were positive for Bartonella species in six cases. CSD skin tests were positive in 13 cases, but exposure to kittens or cats was reported in only 25 cases. em cm 1996;22 (June) Hepatosplenic Bartonella Infections 36. Golden SE. Hepatosplenic cat-scratch disease associated with elevated anti-Rochalimaea antibody titers. Pediatr Infect Dis J 1993; 12: 868-71. 37. Slater LN, PithaJV, Herrera L, HughsonMD, MinK-W, ReedJA. Rochalimaea henselae infection in acquired immunodeficiency syndrome causing inflammatory disease without angiomatosis or peliosis: demonstration by immunocytochemistry and corroboration by DNA amplification. Arch Pathol Lab Med 1994; 118:33-8. 38. Malatack JJ, Jaffe R. Granulomatous hepatitis in three children due to catscratch disease without peripheral adenopathy: an unrecognized cause of fever of unknown origin. Am J Dis Child 1993; 147:949-53. 39. Doyle D, Eppes SC, Klein JD. Atypical cat-scratch disease: diagnosis by a serologic test for Rochalimaea species. South Med J 1994; 87: 485-7. 40. Rappaport DC, Cumming WA, Ros PRo Disseminated hepatic and splenic lesions in cat-scratch disease: imaging features. AJR Am J Roentgenol 1991; 156:1227-8. 41. Port J, Leonidas JC. Granulomatous hepatitis in cat-scratch disease: ultrasound and CT observations. Pediatr RadioI1991;21:598-9. 42. Cohen-Abbo A, Cheatham S, Edwards K. Disseminated cat-scratch disease simulating neuroblastoma. Pediatr Infect Dis J 1992; 11:1058-60. 43. Weintrub P. Your diagnosis, please: fever of unknown origin in a fiveyear-old boy. Pediatr Infect Dis J 1991; 10:80-1, 83. 44. Reed JA, Brigati DJ, Flynn SD, et al. Immunocytochemical identification of Rochalimaea henselae in bacillary (epithelioid) angiomatosis, parenchymal bacillary peliosis, and persistent fever with bacteremia. Am J Surg PathoI1992; 16:650-7. 45. Dangman BC, Albanese BA, Kacica MA, Lepow ML, Wallach MT. Cat scratch disease in two children presenting with fever of unknown origin: imaging features and association with a new causative agent, Rochalimaea henselae. Pediatrics 1995;95:767-71. Downloaded from http://cid.oxfordjournals.org/ by guest on September 9, 2014 25. Zangwill KM, Hamilton DH, Perkins BA, et al. Cat scratch disease in Connecticut: epidemiology, risk factors, and evaluation of a new diagnostic test. N Engl J Med 1993; 329:8-13. 26. Koehler JE, Glaser CA, Tappero JW. Rochalimaea henselae infection: a new zoonosis with the domestic cat as reservoir. JAMA 1994;271: 531-5. 27. Rocco VK, Roman RJ, Eigenbrodt EH. Cat scratch disease: report ofa case with hepatic lesions and a briefreview ofthe literature. Gastroenterology 1985;89:1400-6. 28. Rizkallah MF, Meyer L, Ayoub EM. Hepatic and splenic abscesses in catscratch disease. Pediatr Infect Dis J 1988; 7: 191-5. 29. Lenoir AA, Storch GA, DeSchryver-Kecskemeti K, et al. Granulomatosis hepatitis associated with cat scratch disease. Lancet 1988; 1: 1132-6. 30. Ma1atack JJ, Altman HA, Nard JA, Wiener ES, Urbach AH, McGregor RS. Cat-scratch disease without adenopathy. J Pediatr 1988; 114: 101-4. 31. Kemper CA, Lombard CM, Deresinski SC, Tompkins LS. Visceral bacillary epithelioid angiomatosis: possible manifestations of disseminated cat scratch disease in the immunocompromised host: a report of two cases. Am J Med 1990;89:216-22. 32. Slater LN, Welch DF, Min K-W. Rochalimaea henselae causes bacillary angiomatosis and pe1iosis hepatis. Arch Intern Med 1992; 152:602-6. 33. Steeper TA, Rosenstein H, Weiser J, Inampudi S, Snover DC. Bacillary epithelioid angiomatosis involving the liver, spleen, and skin in an AIDS patient with concurrent Kaposi's sarcoma. Am J Clin Pathol 1992;97: 713-8. 34. Tappero JW, Koehler JE, Berger TG, et al. Bacillary angiomatosis and bacillary splenitis in immunocompetent adults. Ann Intern Med 1993; 118:363-5. 35. Apalsch AM, Nour B, Jaffe R. Systemic cat-scratch disease in a pediatric liver transplant recipient and review of the literature. Pediatr Infect Dis J 1993; 12:769-74. 957