Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Human cytomegalovirus wikipedia , lookup
Urinary tract infection wikipedia , lookup
Marburg virus disease wikipedia , lookup
Sociality and disease transmission wikipedia , lookup
Neonatal infection wikipedia , lookup
Multiple sclerosis signs and symptoms wikipedia , lookup
Carbapenem-resistant enterobacteriaceae wikipedia , lookup
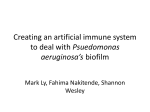
Journal of Hospital Infection (2005) 61, 20–26 www.elsevierhealth.com/journals/jhin Unusual implication of biopsy forceps in outbreaks of Pseudomonas aeruginosa infections and pseudo-infections related to bronchoscopy P. Cornea,*, S. Godreuilb, H. Jean-Pierreb, O. Jonqueta, J. Camposb, E. Jumas-Bilakc, Sylvie Parerd, H. Marchandinb a Service de Réanimation Médicale Assistance Respiratoire, Hôpital Gui de Chauliac, 80 avenue Augustin Fliche, 34295 Montpellier, France b Laboratoire de Bactériologie, Hôpital Arnaud de Villeneuve, Montpellier, France c Laboratoire de Bactériologie, Faculté de Pharmacie, Montpellier, France d Unité d’Hygiène Hospitalière et de Prévention, Hôpital Saint-Eloi, Montpellier, France Received 7 May 2004; accepted 27 January 2005 KEYWORDS Bronchoscope; Pseudomonas aeruginosa; Pulsedfield gel electrophoresis; Outbreak; Biopsy forceps Summary Between January and April 2003, a sudden increase in positive respiratory tract specimens for Pseudomonas aeruginosa was observed in an intensive care unit of the University Teaching Hospital of Montpellier, France. Most of the strains were cultured from bronchoalveolar lavage fluid samples, suggesting that bronchoscopic procedures could be implicated. The relationships between isolates were investigated by antibiotyping and pulsed-field gel electrophoresis. Both phenotypic and molecular markers allowed identification of two consecutive nosocomial outbreaks of respiratory infections related to two different bronchoscopes. These two outbreaks implicated nine and seven patients, respectively. Four of these 16 patients had true infections and recovered with antibiotic therapy. Inspection of both bronchoscopes revealed a damaged internal channel caused by defective biopsy forceps. These defects led to improper cleaning and disinfection of the bronchoscopes despite adherence to all current reprocessing procedures. The two outbreaks were controlled after replacing the inner channels of the bronchoscopes and switching from use of re-usable to disposable biopsy forceps. These outbreaks emphasize the need to establish surveillance procedures for detecting contamination of bronchoscopes, and the importance of recording each endoscopic procedure to facilitate further investigations if needed. Q 2005 The Hospital Infection Society. Published by Elsevier Ltd. All rights reserved. * Corresponding author. Tel.: C33 4 67 33 77 36; fax: C33 4 67 33 67 31. E-mail address: [email protected] 0195-6701/$ - see front matter Q 2005 The Hospital Infection Society. Published by Elsevier Ltd. All rights reserved. doi:10.1016/j.jhin.2005.01.024 P. aeruginosa outbreaks and bronchoscopy 21 Introduction Pulsed-field gel electrophoresis (PFGE) Contaminated endoscopes are the most common cause of device-related nosocomial outbreaks.1 In most cases, implicated micro-organisms are environmental bacteria, particularly Pseudomonas aeruginosa2–4 and mycobacteria.5,6 The outcome of bronchoscopy-related infections can be dramatic, particularly in critically ill patients. Moreover, contamination of bronchoscopes can lead to unnecessary diagnostic and therapeutic interventions. Most outbreaks have resulted from inadequate cleaning and disinfection procedures.7 Less frequently, defective bronchoscopes have been incriminated despite adequate reprocessing.3 As infections related to bronchoscopy are uncommon, there are no formal recommendations for any type of surveillance for these procedures.8 The lack of surveillance system can result in delays in the initiation of outbreak investigation.8 Between January and April 2003, an increasing number of P. aeruginosa isolates were recovered from respiratory tract specimens in an intensive care unit (ICU) of the University Teaching Hospital of Montpellier, France. Most of the strains were cultured from samples in patients who underwent bronchoscopy. This report describes the epidemiological investigations undertaken to prove that this increase was associated with the spread of P. aeruginosa clones and to search for the common source of infection. Genomic DNAs were prepared by a method described previously.10 P. aeruginosa DNAs were digested with 40 U of the the restriction enzyme SpeI (New England Biolabs, Hertfordshire, UK) for 6 h at 37 8C. PFGE was performed with a CHEF-DR III apparatus (Bio-Rad, Hercules, CA, USA) in a 1% agarose gel in Tris-borate-EDTA buffer at 8 8C for 40 h. SpeI digests were run at 4.5 V/cm with pulses from 40 to 5 s. PFGE patterns were compared by visual inspection and interpreted according to the criteria of Tenover et al.11 Materials and methods Bacterial strains and antibiotic susceptibility profiles P. aeruginosa strains recovered from sputum and bronchoalveolar lavage (BAL) samples in patients hospitalized in an ICU of the University Teaching Hospital of Montpellier, France between January and April 2003 were collected. The two bronchoscopes, designated A and B, used in this ICU during the same period were investigated for bacterial culture after flushing the biopsy port into a sterile cup with 40 mL of sterile saline that mimicked BAL, swabbing the biopsy port-cap and the suction port of the bronchoscopes, and sampling tap water and cleaning solutions. The isolates were identified by conventional phenotypic methods. Antibiotic susceptibility was tested by disk diffusion assay on Mueller–Hinton agar, and interpreted according to the recommendations of the Antibiogram Committee of the French Microbiology Society.9 Clinical data and outcomes Medical records were reviewed to determine whether patients who had undergone a bronchoscopy had transient colonization or true infection. Patients were considered to be colonized on the basis of clinical and radiological data, and if subsequent sputum analysis did not reveal the same bacteria as BAL samples. In contrast, infection was defined: (i) on the basis of clinical data, particularly signs of respiratory tract infection with fever and purulent sputum; (ii) on radiographic appearance of a new and persistent pulmonary infiltrate; (iii) on isolation of the same bacterial species from sputum with a bacterial count O107 colony forming units/mL; and (iv) if PFGE patterns of strains from BAL and sputum samples were indistinguishable. Respiratory infections were considered to be potentially attributable to bronchoscopy if they occurred within 14 days of bronchoscopic procedures. Bronchoscope cleaning procedures Bronchoscopes were cleaned by trained personnel in accordance with national guidelines.12 Briefly, after leak testing, instruments were soaked twice (10 and 5 min, respectively) in detergent (Aniosyme Pla, Anios, Lille, France) and cleaned manually by wiping the outer surface and brushing the internal channel and suction ports. Bronchoscopes subsequently underwent complete immersion in a solution of peracetic acid (Anioxyde 1000, Anios) for 20 min. Finally, bronchoscopes were rinsed with sterile water, dried with forced air and stored. Results Between January and April 2003, the frequency of isolation of P. aeruginosa from BAL samples 22 increased dramatically (Figure 1). During this period, 61 bronchoscopic procedures were performed in 36 patients with two different bronchoscopes (bronchoscopes A and B). All patients were mechanically ventilated, and evaluation of pneumonia and bronchial aspiration were the main indications for bronchoscopy. Thirty-six BAL specimens were obtained for bacterial culture and 20 samples yielded growth of 22 P. aeruginosa isolates. Six different antibiotypes, named 1 to 6, were detected among these 22 P. aeruginosa strains (Table I), and two main clusters of isolates were detected according to their antibiotype and their date of isolation. Between 4 and 17 January 2003, eight P. aeruginosa strains were isolated from BAL samples collected with bronchoscope A in patients 1–8 (P1–P8). In five of these eight BAL specimens, organisms other than P. aeruginosa were recovered, including Staphylococcus aureus in two patients (P1 and P6) and Streptococcus pneumoniae in two other patients (P5 and P8). These eight P. aeruginosa isolates were only resistant to imipenem (antibiotype 1) and displayed the same pulsotype A (Table I and Figure 2). Investigation of bronchoscope A after flushing with sterile saline yielded the growth of a P. aeruginosa isolate (strain 10) showing antibiotype 1 and pulsotype A. However, the index case and the mechanism of contamination of bronchoscope A remained unknown. Two patients (P6 and P10) were con- Figure 1 Number of Pseudomonas aeruginosa isolates recovered monthly from bronchoalveolar lavage samples in the intensive care unit between November 2002 and June 2003. Striped bars, number of strains unrelated to the outbreaks determined by pulsed-field gel electrophoresis analysis; open bars, number of strains from outbreak 1 with pulsotype A; solid bars, number of strains from outbreak 2 with pulsotype D. P. Corne et al. sidered to have been infected during bronchoscopy. Indeed, these two patients presented clinical and radiological signs of pneumonia and had subsequent respiratory tract culture (strains 7 and 14) that grew P. aeruginosa with antibiotype 1 and pulsotype A. Between 1 February and 1 April 2003, 14 clinical isolates were recovered in 12 BAL samples from 10 ICU patients (Table I). P. aeruginosa was recovered in pure culture in nine of the 12 BAL specimens, with coagulase-negative staphylococci in two samples and S. aureus in one specimen. Ten of the 14 isolates displayed a similar antibiotype (antibiotype 6) and the same pulsotype (pulsotype D) (Table I and Figure 2). The P. aeruginosa strain recovered from bronchoscope B after flushing with sterile saline (strain 28) showed the same phenotypic and genotypic characteristics. For P12, P. aeruginosa had been isolated from sputum samples before undergoing bronchoscopy, and this patient was considered to be the source of contamination of bronchoscope B. Two patients (P15 and P17) presented with bronchitis after bronchoscopic procedures, and were considered to be infected by the P. aeruginosa strain recovered from bronchoscope B. For three patients (P9, P11 and P18) who underwent bronchoscopy with bronchoscope B, P. aeruginosa strains recovered from BAL samples showed different antibiotypes and unrelated pulsotypes. The four patients infected during bronchoscopic procedures (P6, P10, P15 and P17) recovered under antibiotic therapy. Three patients (P10, P15 and P17) received piperacillin/tazobactam for eight to 14 days. P6 had one recurrence of P. aeruginosa pneumonia and received cefepime and ofloxacin for 14 days and ticarcillin/clavulanate for 21 days with tobramycin for the first seven days. In the ICU, written bronchoscope reprocessing protocols were reviewed, and reprocessing procedures were observed during unannounced visits. No significant breaches in reprocessing procedures were observed and re-usable biopsy forceps were sterilized correctly between patients. Moreover, bronchoscopes A (model BF type P15, Pentax; date of manufacturing: 1999) and B (model BF type 18P, Pentax; date of manufacturing: 2001) had been regularly serviced and maintained, and the last maintenance service was in December 2002 for both bronchoscopes. These two bronchoscopes were removed from the ICU on 21 January and 2 April 2003, respectively. Inspection by the manufacturer revealed large breaches in the internal channel of both bronchoscopes due to defective biopsy forceps. After April 2003, the rate of recovery of P. aeruginosa from BAL specimens returned to baseline level (Figure 1). Straina 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 Patient (P) or bronchoscope Bronchoscope used Date of isolation (day/month) Sample Bacterial count (CFU/mL) Antibiotypeb Infection (I) or contamination (C) Pulsotypec P1 P2 P3 P4 P5 P6 P6 P7 P8 Bronchoscope A P9 P9 P9 P10 P11 P12 P12 P13 P14 P12 P15 P16 P17 P17 P15 P18 P19 Bronchoscope B A A A A A A – A A – B B B – B B B B B B B B B – – B B – 04/01 07/01 08/01 08/01 10/01 12/01 13/01 15/01 17/01 21/01 01/02 01/02 01/02 03/02 14/02 21/02 04/03 14/03 16/03 17/03 18/03 20/3 21/03 24/03 24/03 31/03 01/04 02/04 BAL BAL BAL BAL BAL BAL Sputum BAL BAL – BAL BAL BAL Sputum BAL BAL BAL BAL BAL BAL BAL BAL BAL Sputum Sputum BAL BAL – O106 9!103 2!104 – 3!104 102 O107 O104 104 – – – – 108 O104 104 105 2!104 103 O104 60 3!102 5!103 O107 O107 O106 6!104 – 1 1 1 1 1 1 1 1 1 1 2 3 4 1 5 6 6 6 6 6 6 6 6 6 6 2 6 6 C C C C C I I C C – C C C I C I I C C I I C I I I C C – A A A A A A A A A A B B B1 A C D D D D D D D D D D E D D 23 –, not determined; CFU, colony forming unit; BAL, bronchoalveolar lavage; bold type, strains isolated from bronchoscopes. a Presented by chronological date of isolation. b Determined by pattern of susceptibility to the following antibiotics: ticarcillin; ticarcillin/clavulanate; piperacillin; piperacillin/tazobactam; imipenem; cefotaxime; ceztazidime; cefepime; gentamicin; tobramycin; netilmicin; amikacin; colistin; pefloxacin; and ciprofloxacin. Antibiotype 1, resistance to imipenem only; antibiotype 2, wild-type phenotype; antibiotype 3, resistance to ticarcillin and intermediate susceptibility to ticarcillin/clavulanate, aztreonam, gentamicin and netilmicin; antibiotype 4, multi-resistance; antibiotype 5, intermediate susceptibility to cefepime and resistance to all aminoglycosides tested; antibiotype 6, resistance to ticarcillin, ticarcillin/clavulanate and aztreonam and intermediate susceptibility to cefepime and pefloxacin. c Identical pulsed-field gel electrophoresis (PFGE) patterns were assigned the same annotation, related pulsotypes were noted A, A1, etc. and unrelated PFGE patterns were noted pulsotype A, B, etc. P. aeruginosa outbreaks and bronchoscopy Table I Data for strains of Pseudomonas aeruginosa recovered from bronchoalveolar lavage (BAL) and corresponding sputum samples between January and April 2003 in the intensive care unit 24 P. Corne et al. Figure 2 Pulsed-field gel electrophoresis profiles of selected strains of Pseudomonas aeruginosa. Lane M, concatemer of phage lambda DNA (48.5 kb) as molecular weight marker. Bold type, strains isolated from bronchoscopes. (a) Lanes I and II, strains isolated from bronchoalveolar lavage samples in November 2002 and December 2002, respectively, before first outbreak and showing two unrelated pulsotypes (U); lanes 1, 6, 7, 9 and 10, corresponding strains in Table I with identical pulsotype A. (b) Lanes 16, 18, 19, 21, 23, 24, 26 and 27, corresponding strains in Table I with identical pulsotype D characteristic of the second outbreak; lane 25, strain 25 with unrelated pulsotype E. Discussion The increasing number of P. aeruginosa isolates recovered from BAL specimens in the ICU over a three-month period was investigated by both phenotyping and genotyping methods. Usually, the antibiotype is considered to be an epidemiological marker with low discriminatory power for P. aeruginosa typing due to the capacity of this bacteria to gradually and progressively develop its resistance to antibiotics. However, some outbreaks of P. aeruginosa infections, related or not to bronchoscopy, are still detected on the basis of an unusual antibiotype of the epidemic cluster,13,14 as was the case in the first outbreak reported here. Indeed, eight P. aeruginosa strains isolated from BAL samples during January 2003 only displayed resistance to imipenem, suggesting a mechanism of resistance due to decreased penetration through the outer membrane. Since this pattern of isolated resistance to imipenem is rarely observed in our institution, these strains were suspected to be clonaly related. In contrast, the antibiotype of P. aeruginosa strains involved in the second outbreak was more usual in our institution, and the increasing number of P. aeruginosa isolates recovered from BAL specimens was the warning to activate investigations. Further investigations were conducted by macrorestriction analysis of SpeI-digested DNA, which is considered to be the most discriminatory molecular method for P. aeruginosa typing.15 Finally, two successive P. aeruginosa outbreaks implicating nine and seven patients, respectively, were identified after PFGE analysis and each epidemic cluster could be linked to a contaminated bronchoscope. Previously reported outbreaks of P. aeruginosa infections related to bronchoscopy have been attributed to inappropriate handling methods for disinfection,7,16,17 and to contamination13,18 or improper connection to an automated washerdisinfector.2 More recently, two large outbreaks of P. aeruginosa infections and contamination implicated manufacturing defects in bronchoscopes for the first time. Both outbreaks were attributed to a loose biopsy-port cap in the bronchoscopes, P. aeruginosa outbreaks and bronchoscopy resulting in inadequate disinfection of the bronchoscopes.3,4 In our institution, an automated endoscope washer is not used for bronchoscopes. Cleaning and disinfection procedures are manual and are performed in accordance with national guidelines.12 Although reprocessing procedures were shown to be performed correctly in the ICU, bacteriological investigations of the bronchoscopes yielded a pure culture of P. aeruginosa after saline flushes. In contrast, no bacterial growth was obtained from the biopsy port-cap and the port of the bronchoscopes, tap water or cleaning solutions, suggesting that they were not implicated in the spread of P. aeruginosa. This observation contrasted with previous studies showing that saline flushes are less sensitive than brush cultures of bronchoscope lumens for detection of contamination,19 and demonstrated that saline flushes remain useful to search for bronchoscope contamination. Finally, inspection of both bronchoscopes by the manufacturer revealed a defect in the internal channel caused by defective biopsy forceps. These defects were not detected by leak tests. The biopsy forceps had defective closing that was not visually detectable, probably due to repeated use and decontamination. These damaged inner channels probably sheltered organisms and led to improper cleaning and disinfection of the bronchoscopes despite adherence to all current reprocessing standards. The two outbreaks were controlled after replacing the inner channels of the bronchoscopes. Since these outbreaks, disposable biopsy forceps have been used in the ICU. At present, in France, the use of disposable biopsy forceps is obligatory in gastrointestinal endoscopy because of the risk of prions.20 On the other hand, there are no recommendations for biopsy forceps in bronchoscopy. Based on the outbreaks reported herein, the use of disposable biopsy forceps also seems to be necessary for bronchoscopy. There are no formal recommendations for surveillance of bronchoscopic procedures.21 The two outbreaks reported here emphasize the importance of monitoring microbiology results for all procedures. This type of surveillance can be performed manually or by automated computer system, and identifies an increase in the recovery of organisms in specimens taken during procedures.8 Moreover, the investigation of suspected outbreaks is considerably facilitated by the record of each bronchoscopic procedure, including the patient’s name, the date of the procedure and the serial number of the endoscope used. Another type of surveillance procedure is periodic examination of endoscopic equipment for contamination. This type of surveillance procedure is already performed by 25 30% of bronchoscopists with varied frequencies.22 Although this approach of surveillance is attractive, there are no standard culture methods, no standard for how often the cultures should be performed, and no consensus regarding what threshold of various types of bacteria is considered to be problematic. This area requires more investigation.7,8 Consequently, periodic surveillance cultures of bronchoscopes is not formally recommended.7,23 Reports of outbreaks related to bronchoscopy for which no procedural breaches could be identified are very rare, as are nosocomial infections involving bronchoscopy accessories. We presented here two successive outbreaks of P. aeruginosa infections and pseudo-infections attributed to defective bronchoscopes. For the first time, these defects were attributed to defective re-usable biopsy forceps, and this accessory should be considered as an additional potential source of cross-infection during bronchoscopy. Contamination of the endoscopes was controlled after replacing the inner channels and establishing the use of disposable biopsy forceps despite their cost. These outbreaks emphasize the need for surveillance procedures for detecting contamination of bronchoscopes, and the importance of recording each endoscopic procedure to facilitate epidemiological investigations in case of suspected outbreaks. Acknowledgements The authors are grateful to Pr Philippe Van de Perre for critical reading of the manuscript. References 1. Spach DA, Silverstein FE, Stamm WE. Transmission of infection by gastrointestinal endoscopy and bronchoscopy. Ann Intern Med 1993;118:117—128. 2. Sorin M, Segal-Maurer S, Mariano N, Urban C, Combest A, Rahal JJ. Nosocomial transmission of imipenem-resistant Pseudomonas aeruginosa following bronchoscopy associated with improper connection to the Steris System 1 processor. Infect Control Hosp Epidemiol 2001;22:409—413. 3. Kirschke DL, Jones TF, Craig AS, et al. Pseudomonas aeruginosa and Serratia marcescens contamination associated with a manufacturing defect in bronchoscopes. N Engl J Med 2003;348:214—220. 4. Srinivasan A, Wolfenden LL, Song X, et al. An outbreak of Pseudomonas aeruginosa infections associated with flexible bronchoscopes. N Engl J Med 2003;348:221—227. 5. Kressel AB, Kidd F. Pseudo-outbreak of Mycobacterium chelonae and Methylobacterium mesophilicum caused by contamination of an automated endoscopy washer. Infect Control Hosp Epidemiol 2001;22:414—418. 26 6. Ramsey AH, Oemig TV, Davis JP, Massey JP, Török TJ. An outbreak of bronchoscopy-related Mycobacterium tuberculosis infections due to lack of bronchoscope leak testing. Chest 2002;121:976—981. 7. Culver DA, Gordon SM, Mehta AC. Infection control in the bronchoscopy suite. A review of outbreaks and guidelines for prevention. Am J Respir Crit Care Med 2003;167: 1050—1056. 8. Srinivasan A. Epidemiology and prevention of infections related to endoscopy. Curr Infect Dis Rep 2003;5:467—472. 9. Soussy CJ, Carret G, Cavallo JD, et al. Antibiogram Committee of the French Microbiology Society. Report 2000–2001. Pathol Biol (Paris) 2001;48:832—871. 10. Gouby A, Neuwirth C, Bourg G, et al. Epidemiological study by pulsed-field gel electrophoresis of an outbreak of extended-spectrum b-lactamase-producing Klebsiella pneumoniae in a geriatric hospital. J Clin Microbiol 1994;32: 301—305. 11. Tenover FC, Arbeit RD, Goering RV, et al. Interpreting chromosomal DNA restriction patterns produced by pulsedfield gel electrophoresis: criteria for bacterial strain typing. J Clin Microbiol 1995;33:2233—2239. 12. Ministère de la Santé, de la famille et des personnes handicapées. Circulaire DHOS/E 2/DGS/SD 5 C n82003-591 du 17 décembre 2003 relative aux modalités de traitement manuel pour la désinfection des endoscopes non autoclavables dans les lieux de soins Bull Officiel 2004; 1:11. 13. Schelenz S, French G. An outbreak of multidrug-resistant Pseudomonas aeruginosa infection associated with contamination of bronchoscopes and an endoscope washer–disinfector. J Hosp Infect 2000;46:23—30. 14. Denton M, Kerr K, Mooney L, et al. Transmission of colistinresistant Pseudomonas aeruginosa between patients attending a pediatric cystic fibrosis center. Pediatr Pulmonol 2002; 34:257—261. P. Corne et al. 15. Grundmann H, Schneider C, Hartung D, Daschner FD, Pitt TL. Discriminatory power of three DNA-based typing techniques for Pseudomonas aeruginosa. J Clin Microbiol 1995;33: 528—534. 16. Kolmos HJ, Lerche A, Kristoffersen K, Rosdahl VT. Pseudooutbreak of Pseudomonas aeruginosa in HIV-infected patients undergoing fiberoptic bronchoscopy. Scand J Infect Dis 1994;26:653—657. 17. Silva CV, Magalhaes VD, Pereira CR, Kawagoe JY, Ikura C, Ganc AJ. Pseudo-outbreak of Pseudomonas aeruginosa and Serratia marcescens related to bronchoscopes. Infect Control Hosp Epidemiol 2003;24:195—197. 18. Blanc DS, Parret T, Janin B, Raselli P, Francioli P. Nosocomial infections and pseudoinfections from contaminated bronchoscopes: two-year follow up using molecular markers. Infect Control Hosp Epidemiol 1997;18:134—136. 19. Rutala WA, Weber DJ. Disinfection of endoscopes: review of new chemical sterilants used for high-level disinfection. Infect Control Hosp Epidemiol 1999;20:69—76. 20. Ministère de l’emploi et de la solidarité. Décision du 18 juin portant sur l’interdiction de réutilisation des pinces à biopsie endoscopique digestive. J Officiel 2001;150:10403. 21. British Thoracic Society Bronchoscopy Guidelines Committee, a Subcommittee of Standards of Care Committee of British Thoracic Society. British Thoracic Society guidelines on diagnostic flexible bronchoscopy. Thorax 2001;56(Suppl. 1): 1—21. 22. Srinivasan A, Wolfenden LL, Song X, Perl TM, Haponik EF. Bronchoscope reprocessing and infection prevention and control: bronchoscopy-specific guidelines are needed. Chest 2004;125:307—314. 23. Rutala WA, Weber DJ. Reprocessing endoscopes: United States perspective. J Hosp Infect 2004;56(Suppl. 2): S27—S39.