Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
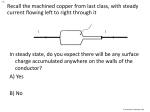
This Week in Microbiology with Vincent Racaniello, Ph.D. Episode #047: Resistance on the surface Aired 19 December 2012 Hosts Vincent Racaniello, Elio Schaechter and Michael Schmidt http://www.microbeworld.org/index.php?option=com_content&view=article&id=1320:twim-‐47-‐ &catid=107:this-‐week-‐in-‐microbiology&Itemid=275 Vincent: This week in Microbiology is sponsored by ASM, the American Society for Microbiology, the world’s largest membership society for microbiologists. To find out how ASM membership can help advance your science, your career, and your network go to ASM.org/Advance. Joining me today from Small Things Considered is Elio Schaechter. Elio: How are you doing? Vincent: I am well. Elio: Nice to be on again. Vincent: Welcome back, hope everything is well with you. Elio: Yeah, we are having some rain in San Diego which is unusual but most welcome. Maybe I’ll get to see some mushrooms popping up. Vincent: I was just going to ask you, will the mushrooms come out now? Elio: They sure will. They are eager to… they don’t wait too long when this happens. Vincent: How soon after the rain will you go look? Elio: Oh, three or four days. Vincent: So on the weekend maybe? Elio: Oh yeah. Vincent: Nice, sounds good. Also joining us today from Medical University of South Carolina is Michael Schmidt. Michael: Hello Vincent, hello Elio. How are things going today up in beautiful New York City? Vincent: It is a beautiful day today. It’s cold but clear and blue skies, about seven degrees Celsius here. We are in winter. Michael: We were supposed to have… the sky was supposed to clear because there is that famous meteor shower that is supposed to occur tonight but it doesn’t look like it’s going to clear so no meteor viewing at the beach tonight. Vincent: You are not going to see it tonight huh? Michael: No, it hasn’t blown out yet. It rained yesterday and it just hasn’t cleared up to see that end-‐of the-‐world meteor shower as we get to the equinox when the Mayans say that the world is going to end. Vincent: Well, speaking of ending, the year is coming to an end very quickly. We are in the last month. It is amazing. I don’t know where it went. Before we start talking about papers I wanted to ask both of you a question. This has to do with hurricane Sandy. As you know a lot of trees fell down during the hurricane. This morning as I was driving to work, it was about freezing early in the morning. I drove past the recycling center where they are piling up all the broken branches and trees and twigs into these huge, huge piles. They clear the streets and they put them on this pile. I have seen this pile grow over the last few weeks. This morning, it was steaming. There was steam, not steam, just condensed vapor coming out of the pile. So I wanted to ask you, what is going on in that pile to make this? Elio: I can tell you the Latin name for it. It is called “eremacausis.” Vincent: Can you spell that? Elio: E-‐R-‐E-‐M-‐A-‐C-‐A-‐U-‐S-‐I-‐S. Vincent: It’s a Latin name for it. Wow. Elio: “Eremacausis” is the Latin name for the phenomenon that makes compost piles so hot that when they are working properly you can’t put your hand in it because it would get burned. This is heat generated by essentially fermentative processes. We don’t think about this in biochemical reactions normally because the reactions are in such dilute conditions that the heat generated dissipates in the buffer. But if you have it in a circumscribed space the heat generated is sufficient that it can even catch on fire. I think that’s been known to happen. What catches on fire is the methane that is often generated. So that maybe what it is. On the other hand, I’m not so sure because the breakdown of lignin is very slow. Obviously there is some cellulose and other stuff in trees and that can be decomposed fairly rapidly but the bulk is lignin and lignin is very recalcitrant. Eventually it gets decomposed by fungi. But I’m not so sure this is the phenomenon that I mentioned. It maybe just simply that they store up the heat or something and under that condition it gives up enough vapors. If the air is cold it looks like steam. Vincent: I see. Hmm, I was wondering if it was some kind of fermentation. Michael: I think it’s just the dew point. I think the pile is warmer and what you saw is the simple dew point because it’s probably simple decomposition and fermentation, as you said, and it’s just raised the heat. Our friends who listen to us and do fermentation for a living in the big-‐scale systems will tell you, their biggest expense in running large scale fermenters is of course not heating them but cooling them because metabolism does generate heat. Vincent: Well, I always try and look at the world around me and see what the microbes are doing. Elio: They are all over. They are all over. Vincent: That is why I pass this. I have to ask my co-‐hosts today about this. There you go a little of the real world. Elio: Good try, good try. [0:05:58] Vincent: Alright, on to our papers. The first one is a paper right up Michael’s alley. It’s in mBio, Horizontal Transfer of Antibiotic Resistance Genes on Abiotic Touch Surfaces: Implications for Public Health. I must say Michael the introduction and parts of the discussion of this paper are frightening. Michael: They truly are. I mean if you don’t read anything, just read the opening paragraph of the conclusion where Dr. Keevil and his colleagues write, “It is estimated that up to 10% of patients admitted to modern hospitals acquire one or more infections and that the proportion rises to 25% in some developing countries.” So that is one in four people admitted to hospitals will actually acquire an infection. In fact that really sets the tone as to why this paper is in mBio and why it is so important to discuss it. It’s about horizontal gene transfer. Over the last few years we had a TWiM where we actually discussed NDM, the New Delhi metallo-‐protease that confers the metallo-‐beta-‐lactamase that confers antibiotic resistance in many gram negatives. It is really rapidly spread around the globe. Elio: Can you spell out what NDM stands for? Michael: New Delhi, the ‘N’ is New, the ‘D’ is Delhi, and the ‘M’ is the metallo-‐beta-‐lactamase. Elio: It is the New Delhi metallo-‐beta-‐lactamase. It is a mouthful but it is easier to remember. I have kind of an allergy to acronyms. Michael: I too am also allergic to acronyms. This is a really good paper for the entering student because it begins to re-‐teach some basic principles like conjugation and determining such simple concepts as the conjugation frequency, which I think is often times forgotten by many modern molecular biologists since we don’t do that much conjugation type research any longer. The conjugation frequency and how conjugation frequency is actually calculated and the methods are really interesting in how you go through it. I am going to take you through this paper telling you this remarkable story. Elio: Before you do, I think you made a very good point that in the lab you don’t see conjugation going on very often. But in nature it actually happens a great deal which is the point of this paper. So there is a disconnect between what we do in experiments and what happens in the real world. [0:09:012] Michael: Yes, absolutely, in fact I’ll just jump to Figure 2 where if you just simply look at the title of Figure 2, it’s the comparison of the frequencies of conjugation of donor E. coli that has a particular phenotype and Klebsiella pneumoniae that contains either the beta-‐lactamase resistance gene and the NDM or the beta-‐lactamase plasmid. The way they setup this experiment is they ask a simple question. They ask if we mix the donor and the recipient—here’s a little digression about how to do conjugation experiments—you have to kill off the donor and the recipient in your ultimate selection, when you get the final colony. Typically you have ten times as many donor cells to the recipient cells. The recipient in this case is they are moving the marker genes which contain the antibiotics. So you are going to score for transfer of the antibiotic resistance determinant from the donor to the recipient. The recipient doesn’t have the antibiotic trait but it has another trait that allows it to grow. This particular trait that this recipient has is its ability to grow in the presence of sodium azide. Any biochemist out there will tell you what the first thing you put in buffers. Of course, Vincent, it is what? Azide, you put it in buffers so bacteria don’t eat your proteins. Vincent: Yes, that would be true. Yeah. Michael: Consequently if the recipient acquires the plasmid that has the resistance marker—in this case it is beta-‐lactamase or NDM—the recipient that has acquired the new information, and if it is stably integrated, it will be able to grow on a plate containing azide and the drug of choice. If the recipient does not have the gene of choice it will of course not live because the antibiotic is there and it won’t be able to grow. Vincent: All this is done just so that you can measure conjugation. Michael: Yes. Elio: The score for the guys who made it. Vincent: Yes. Elio: A successful date. Vincent: The transfer is by conjugation. Is that what is going on? Michael: Conjugation, you are having sex, garden-‐variety sex. The DNA goes through the sex pilus. You have E. coli transferring DNA down its sex pilus into E. coli. You have intra-‐species transfer, which isn’t really that remarkable. But when you have Klebsiella which is not only a different species but it is also a different genus, its moving the beta-‐lactamase or the NDM from it to the E. coli. Now you can begin to understand how antibiotic resistance moves so easily amongst bacteria. Bacteria can have productive sex where the phenotype is transferred amongst different genera. This is really pretty interesting. Figure 2 really goes through this in very eloquent detail. They have a donor and they have a suspension. They mix the Klebsiella and they ask the question, how many Klebsiella beta-‐lactamase genes transfer to the azide resistant E. coli? They get a conjugation frequency down in the 10-‐7 range, which is arguing that it is not very efficient. But if you think about the concentration of bacteria that are resident on normal hospital equipment, it is pretty substantial because the infectious dose for some of these KPCs (Klebsiella Pneumonia Carbapenemase resistance strains) that have some of these determinants or NDM—so I guess that would be KPNDM—can be pretty substantial in the environment and it only takes one to ten of those to affectively cause an infection in a patient because they are so good at infecting the vulnerable in a hospital. [0:14:09] The first thing that these authors did is they asked a very… they are setting up the story is: is conjugation relevant in the dry environment of hospital equipment? Whether it is the rail of the patient’s bed, whether it would be the over-‐bed tray table that you eat your lunch from or whether it would be the IV pole you carry as you walk up and down the hall to re-‐ambulate yourself. What they show in the first figure, and if you look at our modern hospital a lot of the stuff is made out of stainless steel, what you find is that E. coli survives for a long period of time on stainless steel. In Figure 1 you start out with 10,000,000 (ten million) bacteria and you ask the simple question, how many die each day? As you dehydrate, some of the gram-‐negatives die very quickly. E. coli is no exception. You drop two logs in ten days. They start with ten million and in two days you have 100,000 (one hundred thousand). Then over a month you only drop three to four more logs. You can begin to see that way out at 100 days you still almost have a 1,000 E. coli on this solid stainless steel coupon or you still have at least one Klebsiella Pneumonia sitting on this stainless steel coupon. Elio: What is a coupon? They use the term coupon. I didn’t understand it when I read it. What’s a coupon here? A coupon is when you go to the grocery store. Michael: It is literally that metaphor, where you clip something out. A coupon is about the size of a coupon you clip from the grocery store that is made out of the metal. Elio: Oh, I see, just a piece of metal. Michael: It is a piece of metal. You can well imagine you can toss this piece of metal into our standard sterilization oven at 180 degrees C for three hours and it’ll kill everything on it. Pull it out and you can inoculate bacteria. They typically put ten million bacteria in a twenty microliter aliquot. The other thing that you need to appreciate is what the microbe is suspended in. They took great pains to suspend the microbe in phosphate buffered saline [PBS], trypticase soy broth, and brain-‐heart infusion agar. Elio: You don’t mean agar. Michael: Excuse me, I mean broth [brain and heart infusion broth], I’m sorry. Thank you for catching that. Trypticase soy broth is very different than Luria broth. Trypticase soy broth has tryptone yeast extract and a phosphate buffer in it, as well as glucose. That is effectively going to give the micro-‐organism a nice growth medium. As you put 20 microliters on to this coupon it will dry down. Those proteins will effectively stabilize the dehydration effect that can happen to this. When you grow the microbe in brain-‐ heart infusion broth, brain and heart are very high in lipid content, so you have a lot more fat. The reason they work with these three different suspensions, and this goes to their Figure 3, where panel A is phosphate buffered saline, panel B is trypticase soy broth, and panel C is brain-‐heart infusion broth. This then teaches you that what the microbe is in can actually determine how long it will remain viable on these various hospital surfaces. You can make the leap to thinking about what’s going on in the hospital. Typically you think about fugitive emissions just when you sneeze and it hits your monitor. Most of the stuff in our sneeze, unless you have an active cold, is mostly water which is very similar to PBS versus when you have a productive runny nose where there is more, to use the impolite term, snot, which is more like brain-‐heart infusion broth. Vincent: What did you call it, a fugitive emission? Michael: A fugitive emission. Vincent: I never heard that. That’s great. Elio: I don’t quite know why they used artificial media when they could have used fugitive emissions or blood or something that is in the environment. Why not look at the real situation? How peculiar. I think there are habits we have of using laboratory media but it seems a little inappropriate almost? Michael: Well this is I think an issue of reproducibility. Vincent: Everybody’s snot is different. Michael: Pretty much so. Elio: Yeah but you can make a preparation and use it for the life of the experiment. It can be the same preparation. Start up with a lot of snot. Michael: That’s true. You can use saliva and have people chew on wax. Vincent: I can just see people getting hell for that kind of experiment. You know, use Elio’s snot and someone says, “No, it’s Elio’s. This is different from everyone else in the world.” Elio: You bet. That’s why they call me snotty. Michael: This is the fundamental issue of bacteria in the environment and it really drives home the importance of the data associated with this paper. They are actually measuring conjugation between a multi-‐drug resistant group like Klebsiella and they are asking: can it move amongst a different species? They are setting us up to think about antibiotic transference on fomites. A fomite is this inanimate object that health care workers or visitors coincidentally touch and exchange data on. Elio: A fomite could be a towel or a cup or anything that is inanimate that the patient comes in contact with, right? Michael: Correct. It is where the recipient is going to acquire the new knowledge. If we look at the epidemiology of how New Delhi Metallo-‐Beta-‐Lactamase moved throughout the globe, it’s really pretty remarkable at how quickly it spread. I think the conjugation story is really part of that. The second piece of their story is they looked at a continuously active antimicrobial material. The material that they selected was copper. Solid copper and its alloys, containing at least 60% copper, are bactericidal to every micro-‐organism that has been checked. Everything from E. coli to MRSA to C. diff to spores of C. diff, anything that contains greater than 60% copper will inactivate it. [0:21:52] Elio: Can I interrupt you with a little memory? Michael: Sure. Elio: When I setup my lab at the beginning I was growing E. coli, Salmonella in a minimal medium and not unusually it wouldn’t grow at all. I traced it back, and other people had the same experience, that if you use regular distilled water, it comes in contact with copper pipes someplace. If you don’t deionize it, E. coli just is not going to grow. This is with very tiny amounts of copper. So it is exquisitely sensitive to that in the absence of other junk like a nutrient broth. So it brings back memories of how I had to fight copper in liquid medium not only on solid surfaces. Michael: If you look at their methods for Figure 5 and Figure 6 where they are looking at how copper destroys DNA, and we’ll get to that near the end, it really speaks volumes to the point Elio brought up because they found if you had a chelator like EDTA. EDTA will chelate the copper ion. It’s no longer going to breakdown the DNA. They really had a very nice, elegant control. They just used the ladder that they purchased that came in glycerol and EDTA that immediately bound up the copper. It was pretty neat. The remainder of the story of the paper is they ask simple questions about conjugation and whether or not conjugation occurs on stainless steel, on a solid piece of stainless steel versus a piece of metallic copper. The copper that they used in the conjugation experiment I believe was a copper-‐nickel that contained 89% copper, 10% nickel, and 1% iron. It is called “copper nickel.” It is a shiny copper-‐colored stuff that the US dollar, the dollar coin is made out of. If you get your hands on a new dollar coin that is effectively copper-‐nickel and that’s what it looks like. The dollar nickel is exquisitely antimicrobial. [0:24:17] Elio: That by the way goes back a long way. It used to be called the oligometallic effect or some fancy name. When I was a student, they talked about how coins are safe, especially copper coins because bugs aren’t going to live very long on them. That’s a good thing. It just happened to be a coincidence that the US mint decided on a copper-‐containing coin. Vincent: It was not done on purpose then? Michael: No. In fact our quarters are actually mostly copper. They and their table will give you the list of the—I think the quarter is nickel silver, which is 65% copper and 17% zinc, and that’s why it looks like it’s a silver coin when in reality…. Elio: Not a bit of silver in it right? Michael: Not a bit of silver in it. It is just to describe the color. They did the take-‐home conclusion of this paper and ask a simple question: can the plasmid move from the donor to the recipient in the presence of stainless steel? This is Figure 2. The answer was yes. It went between E. coli equally well—from E. coli to E. coli and it had a conjugation frequency at about 3x10-‐5. So it is a relatively high conjugation frequency on solid copper at t0. So it is having sex wicked fast. Vincent: That is amazing to me. It is immediate. Michael: Oh yeah. Vincent: Basically these guys have pili. As soon as they touch another bacterium they start pushing DNA through it or is the DNA always coming out? Michael: Well, you know conjugation you have to be competent to have that sex and so you have to have the right receptor in order to move it across. On the solid surface it’s…if you look at the stainless steel number at t0 what you see is that Klebsiella pneumoniae moved it to the recipient E. coli pretty damn good. Vincent: Amazing. Michael: Then they ask the question: did it breed true? Now this may confuse folks because if you get a colony on a plate obviously it is just not the product of that one sexual encounter. The colony had to multiply upward. So it has obviously bred true. So then why did they then pick and streak on the next, you know, pick and streak? The only thing I can rationally explain is that growing on a solid surface often induces damage in the cell. So you may get the F0 generation to come up on the plate but subsequently that cell may be so damaged and it may not survive. This is why you see a difference between the immediate and then the actual result where they actually look at the subsequent event. When you ask the question, does it move on copper? Well the Klebsiella pneumoniae was able to move it at t0. T0 is effectively…you literally put the bacteria on the coupon, you allow it to dry and then you pull them off. As you see, it was pretty damn fast even on copper. But at two hours you have no conjugation left. That is principally because all the bacteria have died. That takes us to Figure 3 where they actually illustrate for us how quickly copper kills on solid surfaces. They take us through. You can see it is a concentration-‐dependent kill across the board. I’m just going to talk, for the sake of time, about panel A where it is phosphate buffered saline. Up at the top you have stainless steel. What you are seeing out at two hours where there is some killing of stainless steel as you’re probably measuring the dehydration effect, where the bacteria are dying from dehydration. Whereas in panel B you really don’t see any perceived death from stainless steel because the proteins are protecting the bacteria from the dehydration. This is especially apparent when you look at the brain-‐heart infusion broth. As you go down these curves look at the kill curves, we are just going to go look as the rate goes from slow to fast. We are moving from right to left. The first curve is something called “Muntz metal” which is the lowest concentration of copper. Then you have this silver nickel which is 65% copper. Then you have good old cartridge brass which is, as its name implies, the copper jacket of bullets, that’s 70-‐30. Then you have the phosphor bronze which is 95% copper, 5% silicon and a little bit of phosphorous. Then the last one is copper nickel which is 89% copper and the remainder, for all intents and purposes, is nickel. You see how quickly copper kills. Again it really drives home the story that a continuously active antimicrobial material like copper can actually snuff out this movement of multi-‐drug resistance amongst populations in the built environment. The remainder of their paper then gets into the subtleties of the wet killing copper versus the dry killing copper. Wet versus dry is again where you are measuring copper ion versus the ability of what Elio was introducing us to is the oligo-‐sensitivity of copper coins or coins and how they kill. That is specifically explained in their supplemental figure where exposure to dry copper inhibits respiration. They teach you how to measure respiration. I encourage you to look at the supplemental figure because it is really pretty neat that they have both cartridge brass and pure metallic copper. In panels C and D you see no respiration of the bacteria on these copper surfaces. On stainless steel you see actively respiring cells going to town. This again drives home the fact that what the metallic copper is doing is effectively scrounging electrons. It is this scrounging of electrons that effectively results in the rapid death of the micro-‐organism because you effectively are collapsing the membrane potential and it is all about the membrane potential. Elio: Michael since you were very visual here for a while listeners may not have the paper in front of them. The way they measure respiration is on a single-‐cell level using a dye called tetrazolium which turns red upon reduction. So you can look at the respiration in terms of percent cells which are respiring and not respiring under the microscope. Michael: It is really pretty dramatic. On the copper coupon there is no red light and on the stainless steel coupon there is plenty of red light. They have a control on the other side. In panels A, C, and E they use SYTO 9 which is green. You can literally count the number and that’s how you are able to determine the percentage. The interesting thing about all of this is you have to ask yourself the question, how does copper do all these remarkable things? It goes back to the Fenton reaction that we all learned in freshman chemistry where iron-‐2 or copper-‐1, the donator accepts free electrons during the process of metabolism. Since bacteria do all their metabolism inside their cell you have the ability to have these hydroxyl ions that are generated and the net consequence is you get a cycling of copper-‐1 and copper-‐2. It is just a self-‐ fulfilling prophecy that this copper cycles back and forth very quickly and you are generating a lot of free radicals that then results in the cleavage of DNA which are their final set of figures in Figure 5 and in Figure 6 where they actually measure the breakage of DNA as a consequence of copper. It drives home the theme as to conjugation because not only will copper prevent the conjugation that they’ve shown but in transformation. This occurs quite often in gram-‐positives as well as in gram-‐ negatives where you will have the lysis of the bacterium and the bacterium will spill its guts so the DNA is just sitting out there on the surface. Remember bacteria have a means to bring in DNA. That is of course the first major experiment that we all learned about, that DNA was the molecule of life with the rough pneumococci and the smooth pneumococci. They then go in Figure 6 and show how copper is able to break DNA. They just have a really simple way of illustrating this with an agarose gel. They go from having a distinct banding pattern to having a gigantic smear that goes into nothingness as time progresses. They are able to measure how the killing is dependent upon copper and time is essential and of course temperature is important because as we well know the DNA is of course a temperature active molecule. So the warmer it is the more active the copper can get in line with the DNA in concert with the free radical generation and of course cleave and break the DNA down. This group—Warnes, Keevil, and Highmore—have actually done this in an exquisite set of papers that were in AEM where they looked at this in enterococci and staphylococci and E. coli. I think looking at this from truly translational medicine, what they have shown is that this is a good way of controlling the spread of DNA within the environment if you can just short circuit the ability to transfer this material. Vincent: Michael, how much does conjugation on the built environment contribute to the spread of antibiotic resistance, do we have any sense of that versus within the patient for example? Michael: I don’t think we have a good sense of it in the sense that we do know that the built environment does contribute to the rate of hospital associated infections. Elio: And resistance. Michael: And resistance. So I guess now that they have demonstrated this we can probably begin to do a survey of copper in the built environment and ask the question about antibiotic frequency in that population. Elio: Michael, if you were designing a hospital would you put copper surfaces wherever you can or is that premature? Are we at that point yet? Michael: We are at that point. We know that copper…I have a paper in the process of being finally finishing its peer-‐review process that has shown that limited and strategic placement of this material can control the rate at which HAIs are acquired. I think this group has demonstrated that it can control the spread of antibiotic resistance markers, at least from conjugation and maybe, potentially, from transformation. Infection in the hospital is a stochastic process because health care is still individualized, not everybody is treated the same. One of the comments that was made in our review was they asked me did I track how often the health care team moved in and out of the patients room. Of course, if you think about it, that is a really hard thing to do in a multi-‐center trial. How do you begin to analyze that data since I was trained to do binary experiments and ask yes and no questions? This is why I think this paper is a good primer for the entering graduate student because it begins to teach them about conjugation, something that was forgotten, but it is so important in this era of emerging antibiotic resistance to really understand this frequency pattern. Now we are getting much better with our epidemiological tracking because we have such tremendous molecular tools. We can finger print these microbes with MLST or we can even sequence them. But the scary thing is that Stephanie Dancer of the United Kingdom postulates that to acquire an infection in the hospital typically takes a dose of one pathogen whether it be MRSA, whether it be VRE, whether it be C. diff. Vincent: What is VRE? Michael: Vancomycin-‐resistant enterococci, VRE. Elio: How about C. difficile, same thing? Michael: Clostridium difficile is a really challenging organism to cultivate from the environment because you are effectively trying to find spores and you need to transport them back to the lab in pre-‐reduced medium in an anaerobic chamber so that when the spore germinates…. Elio: Why do you have to do that with spores? Are spores sensitive to oxygen? Michael: Typically the way you swab in the environment is you wet them. Elio: I see, so they could germinate. Michael: From our discussion of last time we know what triggers germination. Elio: Moisture for one thing. Michael: Moisture is the trigger. If there is oxygen present, you’re dead. Vincent: Wow. Elio: Maybe they can figure out sampling techniques which don’t involve water, they just involve scraping or something. Anyhow, that is a side point, but Michael I think this is really a beautiful presentation you made because this is maybe a relatively low-‐tech solution to a gigantic problem, or at least a partial solution. I don’t know if copper is that much more expensive to install, maybe it is but the cost is probably within reason. This could revolutionize or might revolutionize the whole problem of hospital acquired infections. I applaud this. It is good stuff. Michael: If you look at the Center for Medicare Services data. I think their most recent data is from 2004, they estimate that a hospital-‐associated infection costs on average $43,000 and it adds 19 days to your stay in the hospital. Elio: You are in the hospital because you are sick and you’re going to get sicker. That is really a horrible thing. Vincent: The last sentence of this paper, “The evolution of potentially untreatable infectious diseases will eventually and inevitably affect us all.” It’s pretty serious. Elio: Cheerful thoughts for the season. Vincent: Really, really nice. Michael thank you, that was really nice. Michael: You are welcome. It was a fun one to do because I think anytime you can…it took me back to my roots of doing the conjugation lab with the undergraduates when I was a TA at Indiana. Vincent: We are happy to be able to do that for you. Our next paper is Applied and Environmental Microbiology. It’s called “Reversing Bacterial Resistance to Antibiotics by Phage-‐Mediated Delivery of Dominant Sensitive Genes.” So we have a little theme here today. [0:43:27] Elio: We sure do. This is more of the same only it has a different flavor. Same category of phenomena being studied, again, having to do with living on the hospital surfaces. Vincent: Right. Hospital surfaces and antibiotic resistance, right? Elio: Right. So we’re still there. So I’m going to present this paper I guess. Vincent: Yes, please, Elio. Elio: The title of the paper is “Reversing Bacterial Resistance to Antibiotics by Phage-‐Mediated Delivery of Dominant Sensitive Genes.” It’s by a group in Tel Aviv. The senior author is Udi Qimron. I don’t know any this people. This is an exercise in [exquisite] cleverness. This is not your regular sort of let’s-‐go-‐after-‐ a-‐phenomenon paper. This is one that requires, I would say, leaps of faith and leaps of technical and genetic savviness. So the title—“Reversing Bacterial Resistance to Antibiotics”—think what that means. It means that if you could take bacteria which are resistant to antibiotics and talk them out of it and persuade them to become sensitive, you solve the problem. Not bad. How do you do that? We’re going to go into that in a minute. It is by phage-‐mediated. Phage-‐mediated, so we already know how they’re going to try. They’re going to try to do this by phage-‐mediated delivery of dominant sensitive genes. Now here’s the story. By the way, before I do that, let me tell you that in the paper they say: Our overall goal in this study is to provide a proof of principle for a genetic system that is able to restore drug sensitivity to drug-resistant pathogens residing on hospital surfaces. Now, if you have copper there, you may not need any of this, right? Michael: Yes, it’s true. Elio: The first paper may be obviating the second one. But this is an exercise in how to think as much as it is in translation or medicine or public health. So it’s well worth going into. It was published in AEM, which is Applied and Environmental Microbiology, and this came out in February of this year. Alright, so it all starts with the finding by Joshua Lederberg, the discoverer of bacterial conjugation, in 1951. It’s not long after he discovered conjugation in 1946, I think, is when they published the paper. He was only 28 years old. Anyhow, he found in this 1951 paper that if you look at heterozygous diploids, that’s the word in use then—today, we will call them “a bacterium that carries a plasmid”—“bacterium that carries a plasmid,” there’s a sensitive gene on one—let’s say, on a chromosome—or a resistance gene on the plasmid or vice-‐versa, just making the difference. Guess who wins? The sensitive gene. Now this is kind of surprising because you think, “Gee, what difference does it make if there is a sensitive gene there? Resistance is resistance.” So you’ll think—streptomycin, which is the drug that they studied—if you have streptomycin in the medium and you have those two genes, the resistance gene is going to dominate and take over, right? This would be logical. Not so. It turns out that, in this case and in some other cases, the sensitive gene is dominant. I guess, to this date, I’m not so sure we know how this works. Mike, are you up on the latest on the mechanism of this? Because I can say something about what was thought about in the old days. Michael: I would go with the old days because I don’t know. Elio: Okay. Now let’s assume that not much has happened in the last 40 years. I’m not sure. Maybe it has. Let’s assume that it has. So in the old days you would say that what happens is the resistant part of the element, which in this case is ribosome, because streptomycin is a drug that inhibits protein synthesis by hitting the ribosomes. So you have now resistance ribosomes and they should be able to go ahead. The sensitive ribosomes, mark up the cell. In other words, having sensitivity does not just stop protein synthesis, it does other things to the cell. What it is to this date, I really don’t know. As of today, I think activating a toxin/endotoxin system which should work fine in this case. Whatever it is, let’s presume we know and go on, whatever it is, sensitivity is epistatic. Now, Michael, that’s a term you haven’t heard since graduate school, right? Michael: No, actually, I heard it last week from the former head of the Nuclear Regulatory Commission who asked an individual what that meant. Vincent: What does that mean, Elio? Elio: Well, it means that one gene has dibs over the other. One is dominant over the other. Vincent: Another word for “dominant”? Michael: No, it’s not dominant. It’s… Elio: Yes, it is. It’s epistatic. It means one is dominant over the other. Yes. Geneticists like their own language and so it is. Anyhow, never mind that. So now they say, “How are we going to do that? How are we going to render a resistant bacterium sensitive by swapping the genes, by swapping the gene for resistance for the gene for sensitivity?” Well, the fact is that they don’t have to actually do any swapping. All you have to do is to introduce the gene for sensitivity. The gene for resistance isn’t going to do anything. So it’s a great situation. So they looked at mutations and they found the mutations of streptomycin in E. coli and they got all kinds. The resistance typically will work at the level of increasing the MIC, that’s the “minimum inhibitory concentration” by about 100-‐fold. So it’ll go from—typically, a regular-‐sensitive E. coli, to start with, is sensitive to about 1½ µg/mL; the resistant will be resistant to about 100 to 200 µg. Okay. So they know that they have such resistant mutants and now they want to reduce the problem by introducing the sensitive gene. So they start out by doing this with plasmids, which is the logical thing to do, and plasmids indeed increase the resistance by considerable fold. I forgot how much it is but it’s quite a bit. So they do that. Imagine now, using this on a surface. They are thinking the same way that people on the first paper think: the surface is a hostile environment, highly contaminated and should be de-‐contaminated. So they say, “How are we going to do this? Are we going to spray a plasmid all over the place?” That doesn’t work because a plasmid by itself isn’t going to get incorporated. So you have to do a conjugation experiment. Just add to the surface a donor bacterium which can carry the plasmid into a recipient but they don’t want to do that. They said they don’t want to spread another E. coli or another [bacteria] into the environment which is already contaminated. There’s also reasons why this is not such a great idea. So they thought and thought and said, “Why not, instead of using a plasmid, use a phage?” Now think about it, a phage is something you can spray on a surface. And it doesn’t have to do anything. It just have to wait for the bacterium to come and pick it up, right, so it’s not a situation with conjugation. We need two cells, two kinds of cells that can mate with each other. Here you just need to add the phage. This leads us vaguely generally into the subject of what can you do with phages and people. The whole subject of phage therapy, we talked about this. Vincent: We did way back. Michael: Yes, and we have this company based out of Maryland called “Intralytix” that makes phage that they actually incorporate into cold cuts. It’s the FDA-‐licensed phage product to control Listeria and they’re also developing one that control Salmonella and E. coli in processed meats and in ground beef. So it’s not too farfetched to think about spraying phage within a hospital environment because the FDA has already letting them do it in food that we consume. Elio: That’s right. Vincent: Yes. TWiM number six, we talked about antibacterial therapy with phage. Yes. Elio: And we will be talking about it again. Phage therapy has this wave function. It comes and goes. Since d’Herelle and Twort discovered phages in 1910/1920, phage therapy has come and gone, come and gone, come and gone. It seems to be a little bit on the ascendancy now. In Eastern Europe it has been used considerably especially in Bulgaria and, I believe, in Estonia. I think also in Russia. So we’ll be hearing more about it. Anyhow, that is not the subject of this paper. It’s not phage therapy. It’s not injecting phages into people. It’s simply spraying it on surfaces. By the way, they have one really neat trick. When you do something like this and you want to figure out if you have in fact succeeded, having in fact introduced the gene you want, what you do is you have a marker gene that goes along with it, typically a resistance gene. But what resistance are you going to use? Because if you’re going to use a gene for resistance to streptomycin, you’re doing exactly what you shouldn’t be doing. You’re adding genes of resistance into the environment. So they figured that there is a compound, namely, potassium tellurite (K2TeO3), a salt, which is quite toxic to bacteria. It’s been known that since, I think, Alexander Fleming. It’s actually been used in syphilis therapy, obviously, unsuccessfully. The beauty of tellurite is that if you become resistant—the gene for tellurite resistance is very small and it is not related to resistance to anything else—so becoming resistant to tellurite is something you can do environmentally because it’s of no effect. You’re not using that for selection. Tellurite is not found in the environment. It’s a very rare metal. It’s okay to do that. It’s very clever to have come up with something like that and they were lucky that they did. Michael: Do they turn black? Elio: Yes. The bacteria growing on tellurite—that’s right, they make intracellular crystals of black tellurite. By the way, the reason why tellurite is toxic—this is total digression, folks, don’t listen if you don’t want to—the tellurite is toxic because it substitutes for sulphur. It’s in the same chemical group as sulphur so the cells take up tellurite [instead of the] sulphur, in this way, they mark up the cellular metabolism completely. It’s quite rare. It’s 75th in abundance on the earth’s crust. Yet, bacteria and some eukaryotes carry genes which are resistant to tellurite. So tellurite is a great substance to use for detecting that you have been successful. They do this. They now play around with the phage and they found that the phage they used does not increase resistance. They take a phage that has the sensitivity gene. They added to bacteria which are resistant and now they ask, “Does the sensitivity go up?” The answer is: not by much, maybe four-‐fold. Not by much. At this point, I’d quit. It didn’t. They say, “Hey, if one gene is good. Two genes are better. So let’s put two genes, two copies of the same gene into the phage”—and, by the way, there’s enough room in the phage to do this, there’s no problem—now they get the sensitivity up considerably. Now it’s okay. It’s fine. Now they have what they want. They have transferred sensitivity to a resistant bacterium by using a phage that transferred the sensitivity genes. Now pretty good so far, right? So another question is, that’s good for the genes they looked at, namely, streptomycin resistance. How often is this true that sensitivity is dominant over resistance? Obviously, if this is a one-‐of-‐a-‐kind phenomenon, only true for streptomycin, we’re not going to get very far. So the answer is, well, it works for nalidixic acid, an inhibitor of gyrase, and they think that it will work for the whole other antibiotics. I don’t know the answer because obviously something is known about this and I don’t know it. Certainly, we have a lot of trimethoprim resistance and stuff like that. So it’s possible that the situation which we have here of sensitivity being dominant to resistance can be used for a lot of other antibiotics. In terms of this being of practical use it matters a great deal because streptomycin is not used. In practice, nalidixic acid is probably isn’t used that much. So it really depends. Is this a phenomenon that is characteristic of resistance and sensitivity for a lot of other antibiotics? And if it were, it may work. Now, in truth, when you look at the whole thing, killing the bacteria is a hell of a lot better than keeping and making them sensitive but it’s very clever. This, I think, is, as I say, it’s an exercise in exquisite elegance. How’s that? Vincent: Well, Michael, if you put copper everywhere, it would probably kill the phages, right? Elio: You might. Michael: It does indeed kill eukaryotic viruses. I don’t know whether or not Bill has tried to inactivate phage. But it’s an issue of you have to marshal your resources. Infection control is a systems-‐based engineering system. You put copper on surfaces closest to the patient and then you may want to put the phage in the mop water to take out the microorganisms, make the microorganisms that are on the floor sensitive to the antibiotics. Vincent: I see. Yes. Right. How about for this New Delhi metallo-‐beta-‐lactamases? Would the target of that be dominant sensitive, do you think? Michael: Well, it’s a plasmid. A lot of these microbes are building these mega-‐plasmids because some of these plasmids can be 100 Kb. It’s almost like the sex plasmid. They become huge. Elio: But wait. That’s not the point. The point is will sensitivity become dominant to resistance? Now I don’t think it would be. Wherever it comes, wherever the origin of the genes is, I don’t think that you can assume in the case of beta-‐lactams that it affects cell wall synthesis. It’s the same story with streptomycin. I doubt. Vincent: Which may be a problem with this approach. Elio: At best, it would be a limited scope. Vincent: Yes. Nonetheless, an interesting exercise, as you say. Elio: Yes. Vincent: By the way, I looked up “epistatic.” A gene whose phenotype—so epistasis is a phenomenon where expression of one gene depends on the presence of one or more modifiers. Elio: That’s what it means? Vincent: Yes. A gene whose phenotype is expressed is called “epistatic” while one whose phenotype is altered or suppressed is called “hypostatic.” Epistasis, it can be contrasted with dominance which is an interaction between alleles of the same gene locus. Elio: Okay. I’m close but not quite. Vincent: Yes, it’s okay. Elio: Take a chance with big words. Vincent: That’s all right. Anything else Michael? Any other thoughts before we close here? Michael: No. I think we again had two dissimilar papers that we managed to tie up into a neat Christmas package. Vincent: It is a nice package here. Content on This Week in Microbiology (microbeworld.org/twim) is licensed under a Creative Commons Attribution 3.0 License. Transcribed by Raphael Fernandez and Steve Stokowski