Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
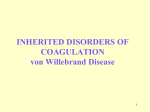
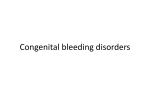
von Willebrand factor Pocket card Issue number 4 2012 von Willebrand factor (vWF): Overview 1 •A multimeric glycoprotein that promotes platelet adherence and aggregation and is a carrier for FVIII in plasma •Protein assembled from identical subunits into linear strings, referred to as multimers, varying in size from ~2–20 million Da •Multimers are subjected to physiologic degradation by the metalloprotein ADAMTS13 (A Disintegrin-like And Metalloprotease domain [reprolysin type] with Thrombospondin type I motifs) •The FVIII-vWF complex circulates as a loosely coiled protein complex •When vascular injury occurs: •vWF (particularly the large multimers) becomes tethered to the exposed subendothelium (collagen, etc.) •High fluid shear rates in the microcirculation induce a conformational change (‘unrolling’ or ‘uncoiling’) in multimeric vWF •This then binds to the platelet membrane receptor glycoprotein (GP) Ib complex, leading to platelet adherence, activation and aggregation, and facilitating clotting •vWF acts as a specific carrier protein for Factor VIII in the plasma •Protects Factor VIII from proteolytic degradation •Factor VIII is released from vWF by the action of thrombin •vWF therefore helps target Factor VIII to sites of vascular injury •vWF therefore plays a major role in blood coagulation and vWF deficiency or dysfunction (von Willebrand disease) leads to a bleeding tendency Role of von Willebrand factor in normal hemostasis Platelet adhesion Platelet activation Platelet aggregation FVIII Thrombin GPIIb/IIIa receptor Platelet GPIa vWF Platelet activators vWF binds to exposed subendothelial collagen receptors at site of injury and interacts with platelet GPIb FVIII Fibrinogen Coagulation cascade Thrombin generation Activated platelets express GPIIb/IIIa receptor GPIIb/IIIa receptor binds to circulating fibrinogen and vWF to cross-link platelets vWF = von Willebrand factor; GP = glycoprotein Fig. 1 Inheritance of von Willebrand disease Autosomal dominant: Type I and Type II vWD Affected male Unaffected female Autosomal recessive: Type III (some Type II) vWD Carrier male Carrier female Affected Unaffected Unaffected Affected Affected Unaffected Carrier child son daughter son daughter child child 1:4 chance Fig. 2 1:4 chance Carrier child 1:2 chance Classification of von Willebrand disease1 Type Description Inheritance Prevalence Bleeding propensity 1 Partial quantitative vWF deficiency Qualitative vWF defect Decreased vWFdependent platelet adhesion with selective deficiency of high-molecularweight multimers Increased affinity for platelet GPIb Decreased vWFdependent platelet adhesion without selective deficiency of high-molecularweight multimers Markedly decreased binding affinity for FVIII Virtually complete deficiency of vWF Defect in platelet GPIb AD Up to 1% Mild-moderate AD (R) Uncommon Variable – usually moderate AD Uncommon AD (R) Uncommon Variable – usually moderate Variable – usually moderate AR Uncommon Variable – usually moderate AR Rare (1:250,000 to 1:1,000,000) Very rare; may be misdiagnosed as type 2B High – severe bleeding Variable – usually moderate 2 2A 2B 2M 2N 3 Platelettype AD Table 1 AD autosomal dominant; AR autosomal recessive; AD (R) autosomal dominant (may be recessive) Summary of von Willebrand disease assays Test Function Assay von Willebrand factor ristocetin cofactor assay (vWF RCo)* Assesses binding activity of vWF to platelets von Willebrand factor antigen (vWF Ag)** vWF protein as measured by protein assays; does not imply functional ability Reflection of vWF activity to antigen concentration and aids differentiation between quantitative and qualitative differences in vWF Measures the cofactor function of FVIII in plasma, and therefore indicates the ability of vWF to bind and maintain the level of FVIII in the circulation Qualitative assessment of size of vWF multimers Ristocetin cofactor activity: quantitates platelet agglutination after addition of vWF and ristocetin Immunoassays such as ELISA, LIA, RIA vWF RCo: vWF Ag Factor VIII (FVIII) von Willebrand factor multimers Ristocetin-induced platelet aggregation (RIPA) Ratio of vWF RCo to vWF Ag FVIII activity: plasma clotting test based on PTT assay using FVIII-deficient substrate; quantitates activity Electrophoresis in agarose gel and visualisation with monospecific anti-vWF Measures the ability of vWF Measures aggregation to bind to platelets in the of platelet-rich plasma to presence of various concent- various concentrations of rations of ristocetin ristocetin RIPA is similar to vWF RCo, but ristocetin is added directly to the plasma without serial dilution Table 2 * Platelet-based assays preferred **ABO blood types have a significant effect on plasma vWF (and FVIII) concentrations. Individuals who have blood type O have concentrations approximately 25% lower compared to persons who have other ABO blood types. Laboratory evaluation1 Positive Initial evaluation (history and physical examination) Laboratory evaluation Initial hemostasis tests • CBC and platelet count • PTT • PT • Fibrinogen or TT (optional) No further evaluation Isolated prolonged PTT that corrects on 1:1 mixing study** or no abnormalities 1 or more tests abnormal IF bleeding history is strong, consider performing initial VWD assays Other cause identified, e.g., platelets*, isolated abnormal PT, low fibrinogen, abnormal TT Possible referral for other appropriate evaluation Negative Initial VWD assays • vWE:Ag • vWF:RCo • FVIII No test abnormal Referral for selected specialized vWD studies • Repeat initial vWD assays if necessary • Ratio of vWF:RCo to vWF:Ag • Multimer distribution • Collagen binding • RIPA or platelet binding • FVIII binding • Platelet vWF studies • DNA sequencing of vWF gene Referral for other appropriate evaluation Fig. 3: Laboratory assessment for vWD or other bleeding disorders. The diagnosis, evaluation and management of von Willebrand disease (2007). Full report, NIH Publication No. 08-5832, December 2007. * Isolated decreased platelets may occur in VWD type 2B. **Correction in the PTT mixing study immediately and after 2-hour incubation remo ves a factor VIII (FVIII) inhibitor from consideration. Investigation of other intrinsic factors and lupus anticoagulant also may be indicated. CBC, complete blood count; PT prothrombin time; PTT partial thromboplastin time; RIPA, ristocetin-induced platelet aggregation; TT, thrombin time; vWF:Ag, vWF antigen; vWF:RCo, vWF ristocetin cofactor activity. Laboratory classification of von Willebrand disease Expected laboratory values in VWD Normal Type 1 Type 2A Type 2B Type 2M Type 2N Type 3 PLTVWD* VWF:Ag N L, ↓ or ↓ or L ↓ or L ↓or L N or L absent ↓ or L ↓↓ ↓ ↓or ↓ ↓↓ N or ↓ ↓↓ ↓↓ N or L absent ↓ ↓ N or ↓ N or ↓ ↓↓ N or L often N ↑↑↑ ↑ ↓ absent ↑ N absent N 1-9 IU/ dL absent absent ↑↑↑ ↑ ↓ or N ↑ ↓ FVIII N L, ↓ or ↓↓ N or ↓ RIPA LD-RIPA PFA100® CT BT Platelet count VWF multimer pattern N absent N often N ↓ absent absent N or ↑ ↑ N N N or ↑ N ↑ N ↑ N N N ↑↑↑ N N N abnormal abnormal N N absent abnormal VWF:Rco N often N ↑↑↑ ↑ Table 3 The symbols and values represent prototypical cases. In practice, laboratory studies in certain patients may deviate slightly from these expectations. L, 30-50 IU/dL; ↓, ↓↓, ↓↓↓, relative decrease; ↑, ↑↑, ↑↑↑, relative increase; BT, bleeding time; FVIII, factor VIII activity; LD-RIPA, low-dose ristocetin-induced platelet aggregation (concentration of ristocetin ≤ 0.6 mg/mL); N, normal; PFA-100® CT, platelet function analyzer closure time; RIPA, ristocetin-induced platelet aggregation; VWF, von Willebrand factor; VWF antigen; VWF:Rco, VWF ristocetin cofactor activity. *Note: persons who have platelet-type VWD (PLT-VWD) have a defect in their platelet GP1b. Laboratory test results resemble type 2B VWD, and both have a defect in their LD-RIPA. In the VWF:platelet binding assay, persons who have type 2B VWD have abnormally increased platelet binding. Normal persons and those who have PLT-VWD have no binding of their VWF to normal platelets at low ristocetin concentrations. Special considerations for laboratory diagnosis of vWD Repeated testing for vWD is sometimes needed to identify low levels of a • A number of factors (e.g. stress, surgery, pregnancy, systemic inflammation, oral contraceptives) can lead to increased plasma vWF levels Considerations in sample preparation •Ensure phlebotomy is as calm as possible to avoid stress-induced increases in vWF •Fasting or non-lipidaemic samples should be used; icteric or haemolysed samples may compromise the quality of testing results •Blood should be centrifuged promptly to obtain plasma and stored at room temperature if tests are to be performed within 2 hours. Frozen plasma samples should be thawed at 37°C to avoid cryoprecipitate •Plasma should be ‘platelet-poor’ or ‘platelet-free’; care is required during centrifugation; double centrifugation may be of benefit The vWF reference standard is critical to the laboratory diagnosis of vWD •Where possible, all laboratories should use the same standard to avoid artifactual discrepancies •Results of vWF assays can only be reported in international units (IU) if referenced to the WHO standard; if a reference plasma pool is used, it is usually reported as a percentage of normal Variability •The variability (CV) of the vWF:RCo assay and of the vWF:Ag assay is high (≥20–30% and ≥10–20%, respectively) •Interlaboratory variability is also considerable Source of reference 1 The Diagnosis, Evaluation, and Management of von Willebrand Disease (2007). Full report, NIH Publicaton No: 08-5832, December 2007. COBAS and LIFE NEEDS ANSWERS are trademarks of Roche. ©2012 Roche Roche Diagnostics International Ltd CH-6343 Rotkreuz Switzerland www.cobas.com