Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
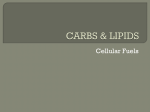
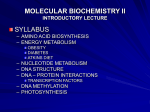
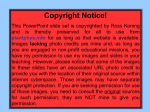
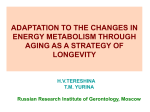
+ model ARTICLE IN PRESS YEXNR-09316; No. of pages: 8; 4C: Experimental Neurology xx (2006) xxx – xxx www.elsevier.com/locate/yexnr Brain neuroprotection by scavenging blood glutamate Alexander Zlotnik a , Boris Gurevich a , Sergei Tkachov a , Ilana Maoz b , Yoram Shapira a , Vivian I. Teichberg b,⁎ a Division of Anesthesiology and Critical Care, Soroka Medical Center, Ben-Gurion University of the Negev, Beer-Sheva, Israel b Department of Neurobiology, Weizmann Institute of Science, Rehovot 76100, Israel Received 27 June 2006; revised 2 August 2006; accepted 4 August 2006 Abstract Excess glutamate in brain fluids characterizes acute brain insults such as traumatic brain injury and stroke. Its removal could prevent the glutamate excitotoxicity that causes long-lasting neurological deficits. As blood glutamate scavenging has been demonstrated to increase the efflux of excess glutamate from brain into blood, we tested the prediction that oxaloacetate-mediated blood glutamate scavenging causes neuroprotection in a pathological situation such as closed head injury (CHI), in which there is a well established deleterious increase of glutamate in brain fluids. We observed highly significant improvements of the neurological status of rats submitted to CHI following an intravenous treatment with 1 mmol oxaloacetate/100 g rat weight which decreases blood glutamate levels by 40%. No detectable therapeutic effect was obtained when rats were treated IV with 1 mmol oxaloacetate together with 1 mmol glutamate/100 g rat. The treatment with 0.005 mmol/100 g rat oxaloacetate was no more effective than saline but when it was combined with the intravenous administration of 0.14 nmol/100 g of recombinant glutamateoxaloacetate transaminase, recovery was almost complete. Oxaloacetate provided neuroprotection when administered before CHI or at 60 min post CHI but not at 120 min post CHI. Since neurological recovery from CHI was highly correlated with the decrease of blood glutamate levels (r = 0.89, P = 0.001), we conclude that blood glutamate scavenging affords brain neuroprotection Blood glutamate scavenging may open now new therapeutic options. © 2006 Elsevier Inc. All rights reserved. Keywords: Acute brain neurodegeneration; Closed head injury; Brain glutamate levels; Blood glutamate scavenging; Oxaloacetate; Glutamate-oxaloacetate transaminase; Neuroprotection; Neurological severity score; Spontaneous recovery Introduction It is nowadays well established that abnormally high glutamate (Glu) levels in brain interstitial and cerebrospinal fluids (ISF and CSF, respectively) are the hallmark of several neurodegenerative conditions that result from acute events, such as stroke, traumatic brain injury or bacterial meningitis (Castillo et al., 1996; Johnston et al., 2001; Zauner et al., 1996) or develop chronically in diseases such as glaucoma, amyotrophic lateral sclerosis or HIV dementia (Ferrarese et al., 2001; Shaw et al., 1995; Spranger et al., 1996; Spreux-Varoquaux et al., 2002). Because excess Glu exerts neurotoxic properties, a great deal of efforts have been made in recent years to reach a better ⁎ Corresponding author. E-mail address: [email protected] (V.I. Teichberg). understanding of how the brain protects itself from excess Glu, and on ways drugs could provide neuroprotection. Brain inherent protection is credited mainly to the presence, both on nerve terminals and on astrocytes, of members of a large family of Na+-dependent Glu transporters which bind and take up Glu and guarantee that the very high concentrations of Glu transiently present after synaptic or astrocytic release (Danbolt, 2001) are soon decreased to concentrations at which Glu exerts neither overt excitatory nor excitotoxic activities (Sattler and Tymianski, 2001). So far, however, little attention has been given to the Glu transporters present on brain blood vessels (Danbolt, 2001) and on their role in the control of brain extracellular Glu. The existence of a brain-to-blood efflux of Glu, though discovered already 45 years (Berl et al., 1961) ago, has also been widely ignored. Nevertheless, in vitro studies (O'Kane et al., 1999) have proposed that the Glu transporters present on the 0014-4886/$ - see front matter © 2006 Elsevier Inc. All rights reserved. doi:10.1016/j.expneurol.2006.08.021 Please cite this article as: Alexander Zlotnik et al., Brain neuroprotection by scavenging blood glutamate, Experimental Neurology (2006), doi:10.1016/j. expneurol.2006.08.021 ARTICLE IN PRESS 2 A. Zlotnik et al. / Experimental Neurology xx (2006) xxx–xxx antiluminal side of the brain capillary endothelial cells could be responsible for the elimination of Glu from brain into blood while in vivo studies (Hosoya et al., 1999) have detailed the efflux of L-aspartate through the blood–brain barrier. Following this lead, we recently established (Gottlieb et al., 2003) that a rapid brain-to-blood Glu efflux indeed takes place since one observes radioactive Glu appearing in blood as soon as it is injected into rat brain lateral ventricles. We further showed that this brain-to-blood Glu efflux can be accelerated by the creation of a larger Glu concentration gradient between the cerebrospinal fluid/capillary endothelial cell and blood plasma. Using two paradigms based on the fate of radiolabeled Glu infused into brain, we observed its increased appearance in blood and enhanced disappearance from brain following a decrease of blood Glu levels (Gottlieb et al., 2003). A decrease of blood Glu levels and an increase of the driving force for the brain-to-blood Glu efflux was achieved by exploiting the Glu scavenging properties of the blood resident enzymes glutamate-pyruvate transaminase (GPT) and glutamate-oxaloacetate transaminase (GOT) which transform Glu into 2-ketoglutarate in the presence of the respective Glu co-substrates, pyruvate and oxaloacetate (Gottlieb et al., 2003). Having demonstrated that the latter co-substrates, also called blood Glu scavengers (Gottlieb et al., 2003), cause an increased brain-to-blood Glu efflux, we have tested now the prediction that the intravenous administration of oxaloacetate should provide brain neuroprotection to rats submitted to an insult resulting in the release of excess Glu in brain interstitial and cerebrospinal fluids. In rats as in humans, traumatic brain injury is accompanied by a large increase of Glu in brain fluids (Baker et al., 1993; Bullock et al., 1998; Palmer et al., 1993; Richards et al., 2003; Rose et al., 2002; Vespa et al., 1998) and there is a tight correlation between the elevated levels of Glu and the poor neurological outcome (Koura et al., 1998; Zauner et al., 1996; Zhang et al., 2001). Using a rat model of traumatic brain injury, we confirm here the prediction of the brain neuroprotective effects of blood Glu scavenging and establish a very tight correlation between the improvement of the neurological status and the reduction of blood Glu levels. These observations could have clinical implications. and to the Guidelines for the Use of Experimental Animals of the European Community. The experiments were approved by the Animal Care Committees of Ben-Gurion University of the Negev and of the Weizmann Institute. Spontaneously breathing male Sprague Dawley rats weighing 200–300 g were anesthetized with a mixture of isoflurane (initial inspired concentration 2%) in 100% oxygen (1 l/min). The rectal temperature was maintained at 37°C using a heating pad and anesthesia was considered as sufficient for surgery when tail reflex was abolished. Catherization of the tail vein was carried out with a BD Neoflon 24 g catheter for allowing fluid infusion. Catherization of the tail artery was performed to allow blood sampling and determination of blood pressure and heart rate. Blood samples were analyzed for pH, pO2, pCO2, HCO3−. Glucose levels were measured with Accu-Chek sensor comfort. After scalp infiltration with bupivacaine 0.5%, it was incised and reflected laterally and a cranial impact of 0.5 J was delivered by a silicone-coated rod which protruded from the center of a free-falling plate as previously described (Shapira et al., 1988). The impact point was 1–2 mm lateral to the midline on the skull's convexity. Following closed head injury (CHI), the incision was sutured and rats were laid on their left side in order to recover from anesthesia. A neurological severity score (NSS) was evaluated 1 h after CHI. Neurological severity score The NSS was determined (Shapira et al., 1988) by a blinded observer. Points are assigned for alterations of motor functions and behavior so that the maximal score of 25 represents severe neurological dysfunction while a score of 0 indicates an intact neurological condition. Specifically, the following were assessed: ability to exit from a circle (3 point scale), gait on a wide surface (3 point scale), gait on a narrow surface (4 point scale), effort to remain on a narrow surface (2 point scale), reflexes (5 point scale), seeking behavior (2 point scale), beam walking (3 point scale), and beam balance (3 point scale). Experimental design Materials and methods Materials pET28 was purchased from Novagen. L-Glutamate, oxaloacetate, NAD, glycine, and hydrazine hydrate were purchased from Sigma. Glutamate dehydrogenase was purchased from Roche. Glutamate-oxaloacetate transaminase (GOT) cDNA was cloned from human hepatoma cells hepG2, expressed in E. coli and purified by Ni-agarose chromatography. GOT assay kit was purchased from Sigma. Animal anesthesia The experiments were conducted according to the recommendations of the Declarations of Helsinki and Tokyo The 1-h assessment of NSS was followed 15 min later by a 30-min-long intravenous administration at a rate of 30 μl/ min/100 g of a solution containing either saline, or the drugs to be administered. Following treatment, the animals were returned to their cages and given free access to food and water. At 24 h and 48 h, the assessment of NSS was repeated. Determination of blood/plasma Glu Aliquots of deproteinized whole blood/plasma (200 μl aliquot) were used for the determination of Glu concentration by the fluorometric method of Graham and Aprison (1966). All determinations were done at least in duplicates. The results are expressed as mean ± SD. Please cite this article as: Alexander Zlotnik et al., Brain neuroprotection by scavenging blood glutamate, Experimental Neurology (2006), doi:10.1016/j. expneurol.2006.08.021 ARTICLE IN PRESS A. Zlotnik et al. / Experimental Neurology xx (2006) xxx–xxx 3 Brain water content Brain hemispheres were removed 120 min after CHI in some groups while in others, brain tissue samples of approximately 50 mg were excised at 24 h post CHI from a location immediately adjacent to the area of macroscopic damage in the left hemisphere and from a corresponding area in the right hemisphere. These tissue samples were used for determination of water content. Water content was determined from the difference between wet weight (WW) and dry weight (DW). Specifically, after WW of fresh brain tissue samples was obtained, samples were dried in a desiccating oven at 120°C for 24 h and weighed again to obtain DW. Tissue water content (%) was calculated as (WW − DW) × 100 / WW. Statistical analysis The a priori hypothesis was that the Glu concentrations in blood samples would differ for treatment groups versus controls. Accordingly, this comparison was made with a t-test (differences were considered as significant when P < 0.05). The significance of comparisons of the NSS between different groups was assessed using analysis of variance (ANOVA) with Bonferroni post hoc testing. The minimal level of significance accepted was P < 0.05. Data are presented as means ± SD or SEM when n > 8. Differences were considered as significant when P < 0.05. Results Intravenous OxAc improves recovery from CHI We examined whether OxAc-mediated blood Glu scavenging (Gottlieb et al., 2003) causes neuroprotection in a pathological situation, such as closed head injury (CHI), in which there is a well-established deleterious increase of Glu in brain fluids (Baker et al., 1993; Bullock et al., 1998; Palmer et al., 1993; Richards et al., 2003; Rose et al., 2002; Vespa et al., 1998). We therefore submitted rats to CHI and treated them either with intravenous OxAc, Glu or saline, as described in Fig. 1. We also investigated the effects of an intravenous treatment with OxAc + Glu, as the presence of elevated Glu in blood is expected to neutralize the OxAc-mediated decrease of blood Glu levels. Fig. 1 shows that at both 24 and 48 h post CHI, animals treated with OxAc recovered best from CHI while those treated with Glu recovered the least. Animals treated with OxAc + Glu had a similar recovery as those treated with saline. It is of interest to note that in comparison to the NSS measured 1 h post CHI, all rats showed a very significant recovery after 48 h. To correlate the therapeutic effect of OxAc with its blood Glu scavenging activity, we investigated the blood Glu levels before and after CHI, as well as the outcome of the subsequent 30-minlong treatments with either OxAc or saline. Fig. 2 shows that CHI caused by itself a 20% reduction (Student's t-test P = 5 × 10− 4) of the blood Glu levels measured after 60 min, and those were further reduced to 40% by the treatment with Fig. 1. Effects of a blood Glu scavenger and of Glu on the recovery from TBI. Rats were submitted to TBI and a NSS established after 60 min. Rats were then injected intravenously for a total duration of 30 min (as in Fig. 3A) either with saline (30 μl/min/100 g), OxAc (30 μmol/min/100 g) or OxAc + Glu (30 μmol/ min/100 g each). Twenty-four and forty-eight hours later, rats were submitted to various tests to establish the NSS. The scores shown above each column correspond to NSS averages with bars indicating the standard error of the mean. The groups from left to right are as follows: control saline (n = 33) at 1 h and 24 h; OxAc (n = 32); Glu (n = 32); OxAc + Glu (n = 17) at 24 h and 48 h; one-way ANOVA and Bonferroni multiple comparison tests: at 24 h: saline versus OxAc: P < 0.05; saline versus Glu: P < 0.01; Glu versus OxAc: P < 0.001; saline versus OxAc + Glu: P > 0.05. At 48 h: saline versus OxAc: P < 0.001; OxAc versus Glu: P < 0.001; OxAc versus OxAc + Glu: P < 0.05. intravenous OxAc, but not with saline. The OxAc-induced decrease of blood Glu is transient and is soon followed by a suggested compensatory influx into blood of Glu originating from peripheral organs that sense the momentous decrease in the blood Glu levels (Gottlieb et al., 2003). Intravenous OxAc fastens recovery from CHI To compare the time course of the spontaneous recovery from CHI of saline- versus OxAc-treated rats, we monitored their NSS values over 24 days. Fig. 3 shows that an extensive recovery from the neurological deficits inflicted by CHI occurs over this time period. However, the rate of recovery in the OxAc-treated rats is significantly faster than that of the salinetreated rats, and the latter remain at 25 days with an overt neurological handicap. The recovery from CHI correlates with the decrease of blood Glu levels In order to demonstrate that the NSS changes are correlated with the changes of blood Glu levels, we plotted in Fig. 4 the % NSS improvement of individual rats assessed 24 h after CHI versus the %decrease of their blood Glu levels measured 90 min after CHI. A strong correlation (r = 0.89) with a high statistical significance (P = 0.001) was observed revealing that a 40% decrease of blood Glu levels affords an almost optimal improvement of the NSS. Thus, low blood Glu levels that facilitate an increased brain-to-blood Glu efflux appear to exert a brain neuroprotective effect while high blood Glu levels are deleterious. This conclusion is in line with the clinical Please cite this article as: Alexander Zlotnik et al., Brain neuroprotection by scavenging blood glutamate, Experimental Neurology (2006), doi:10.1016/j. expneurol.2006.08.021 ARTICLE IN PRESS 4 A. Zlotnik et al. / Experimental Neurology xx (2006) xxx–xxx Fig. 2. Blood Glu levels following a traumatic brain injury. Glu levels are expressed as the percent of the basal Glu levels measured before TBI. Blood aliquots are removed 60 min after TBI, at 75 min (i.e., 15 min of intravenous injection of either saline 30 μl/min/100 g or 30 μmol/min/100 g OxAc) and at 90 min (end of intravenous treatment). The results are presented as mean ± standard error of the mean (n = 12–13). Paired t-test: 0 versus 60 min saline P = 5 × 10− 4; 0 versus 60 min OxAc P = 10− 4; 60 min versus 75 min saline: P = 0.59; 60 min versus 75 min OxAc: P = 3 × 10− 3; 75 min versus 90 min saline: P = 0.89; 75 min versus 90 min OxAc: P = 2 × 10− 4. observations that establish a linear correlation between CSF and plasma Glu concentrations (Castillo et al., 1997), and a very significant association between the high blood Glu levels and the neurological deterioration and outcome after stroke (Castillo et al., 1997; Serena et al., 2001) and intracerebral hemorrhage (Castillo et al., 2002). OxAc decreases brain edema after CHI To assess whether the treatment with OxAc improves, in addition to the NSS, other parameters that reflect the severity of the inflicted CHI, we also measured, 120 min and 24 h after CHI, the extent of brain edema in OxAc-treated versus salinetreated animals. Brain edema is partly due the presence of excess Glu since it is decreased by glutamate receptor antagonists (Furukawa et al., 2003; Shapira et al., 1992; Westergren and Johansson, 1992; Westergren and Johansson, 1993). The efficient removal of brain excess Glu is thus expected to decrease the edema. Fig. 5 shows that the OxAc Fig. 3. Time course of the recovery from TBI in saline (n = 7) and OxAc-treated (n = 7) rats as monitored by NSS values presented here as mean ± standard deviation. Student's t-test for saline versus OxAc at 25 days: P = 0.006. Fig. 4. Correlation between the decrease of blood Glu levels and the improvement of NSS. The %blood Glu decrease and the %NSS decrease of individual rats were calculated respectively as follows: (Glut=0 − Glut=90 min) / Glut=0, (NSSt=1 h − NSSt=24 h) / NSSt=1 h. treatment caused a significant reduction of brain water content at 24 h. The beneficial effect of OxAc was not observed in the other groups for which the treatment includes the intravenous administration of Glu (data not shown). Since OxAc could act on brain edema as an osmotic agent, we measured both the blood osmolality and Na content both before and after the 30min-long treatments with OxAc or saline. There was no change in the saline group (303 ± 3.5 mosM (pretreatment) versus 299 ± 3 mosM (post-treatment); Na: 140 ± 1 meq/l versus 141 ± 0.8 meq/l) but a very significant increase in the OxAcgroup: (301 ± 5 mosM versus 338 ± 8 mosM; Na: 139 ± 1 meq/ l versus 164 ± 3.4 meq/l). The hypernatriema and hyperosmolarity in the OxAc-treated rats can be accounted by the fact that OxAc is administered together with 2 Na equivalents. To determine that the NSS improvement and edema reduction in the OxAc-treated rats were not due to an osmotic “therapy”, we submitted rats after CHI to a hypertonic (3% NaCl) saline treatment. As the respective NSS values obtained at 60 min and Fig. 5. Brain edema formation at 120 min and 24 h following TBI and treatment with either saline 30 μl/min/100 g or 30 μmol/min/100 g OxAc. The columns represent mean ± standard deviation; 120 min: saline (n = 6); OxAc (n = 6); P = 0.09; 24 h: saline (n = 7); OxAc (n = 6) P = 0.008; the P values correspond to unpaired t-tests. Please cite this article as: Alexander Zlotnik et al., Brain neuroprotection by scavenging blood glutamate, Experimental Neurology (2006), doi:10.1016/j. expneurol.2006.08.021 ARTICLE IN PRESS A. Zlotnik et al. / Experimental Neurology xx (2006) xxx–xxx 5 24 h post CHI were 15.6 ± 3.6 and 12.4 ± 5.3 (n = 7; P = 0.16), we conclude that the beneficial effects of OxAc are not the result of an osmotic therapy. Therapeutic dose range of OxAc The pharmacological effects described above were all obtained following the administration of 1 mmol OxAc/100 g rat weight. This dose produces an almost complete recovery of rat submitted to CHI. To determine the effective dose range of OxAc, we repeated CHI experiments while decreasing the OxAc dose administrated down to 0.01 mmol/100 g rat weight. Fig. 6 shows that the therapeutic effects of OxAc are dosedependent with an EC50 value around 0.01 mmol/g rat weight. The therapeutic effect of OxAc depends on the presence of GOT As the smaller extent of neurological recovery obtained with the low doses of OxAc (< 1 mmol/100 g rat weight—Fig. 6) could be due to slower rates of activation of blood resident GOT, we investigated whether the low doses of OxAc (i.e., of the GOT co-substrate concentration) could be compensated by increasing blood GOT concentrations, as expected from the Michaelis–Menten enzyme rate equation. Fig. 7 shows that it is indeed the case since an almost complete neurological recovery could be obtained when rats were treated IV with 0.005 mmol OxAc/100 g (a dose which by itself has no detectable therapeutic effect) administered together with 0.14 nmol recombinant GOT/100 g rat. This GOT dose increases by about 30-fold the basal amount of blood GOT. Therapeutic time window of OxAc Fig. 8 illustrates the fact that OxAc exerts a neuroprotective action when administered just before submitting rats to CHI or Fig. 6. The neurological improvement caused by OxAc after TBI is dose-dependent. The %neurological recovery at 24 h was calculated as (NSSt=1 h − NSSt=24 h) / NSSt=1 h. The results are presented as mean±standard deviation (n=6–8). Note that the abscissa show the amounts of OxAc injected in mmol/100 g. Fig. 7. Potentiation of the therapeutic effects of OxAc after TBI by the concomitant intravenous administration of recombinant glutamate-oxaloacetate transaminase. GOT. Rats were submitted to TBI and treated with a solution containing 0.14 nmol GOT/100 g rat and increasing amounts of OxAc. The % neurological recovery at 24 h was calculated as (NSSt=1 h−NSSt=24 h)/NSSt=1 h. The results are presented as mean ± standard deviation (n = 6–8). Note that the abscissa show the amounts of OxAc injected in μmol/100 g. when the treatment is delayed to 60 min post CHI. It is however no more effective when it is delayed by 2 h post CHI. These particular time points were selected because of the well-established duration of the excess Glu in rat brain fluids following CHI (Faden et al., 1989; Palmer et al., 1993; Rose et al., 2002; Stoffel et al., 2002) or stroke (Guyot et al., 2001; Margaill et al., 1996; Phillis et al., 1996). In all cases, following the brain insult, there is a rapid and transient elevation of excess Glu in brain fluids that does not last more than 2 h. Thus, one can predict that OxAc will be effective in removing excess brain Glu only when administered before the brain injury or during the time window of elevated Glu but not after. The results presented in Fig. 8 are in line with this prediction. Fig. 8. Therapeutic time window of OxAc. Rats submitted to TBI were either pretreated with 30 μmol/min/100 g OxAc or treated after 60 min or 120 min post TBI with 30 μmol/min/100 g OxAc. Twenty-four and forty-eight hours later, rats were submitted to various tests to establish the NSS. The results are presented as NSS averages with bars indicating the standard deviation (n = 8). Please cite this article as: Alexander Zlotnik et al., Brain neuroprotection by scavenging blood glutamate, Experimental Neurology (2006), doi:10.1016/j. expneurol.2006.08.021 ARTICLE IN PRESS 6 A. Zlotnik et al. / Experimental Neurology xx (2006) xxx–xxx Discussion In the present work, we tested the prediction that blood Glu scavenging should produce brain neuroprotection in a pathological situation characterized by the presence of excess Glu in brain fluids. CHI was chosen as a test system because the occurrence of elevated Glu levels in brain fluids upon brain injury has been extensively documented (Baker et al., 1993; Bullock et al., 1998; Palmer et al., 1993; Richards et al., 2003; Rose et al., 2002; Vespa et al., 1998). Moreover, there is a tight correlation between the elevated levels of Glu and the poor neurological outcome (Koura et al., 1998; Zauner et al., 1996; Zhang et al., 2001) suggesting that the removal of excess Glu may possibly improve the neurological outcome after CHI. OxAc was chosen as a blood Glu scavenger because it is more effective than pyruvate (Gottlieb et al., 2003). As predicted from its blood Glu scavenging activity and ability to increase the efflux of excess Glu from brain into blood (Gottlieb et al., 2003), OxAc was found here to exert a potent brain neuroprotection manifested by the enhanced neurological recovery after CHI and brain edema reduction. It could be argued that the neuroprotective effects of OxAc are not due to its blood Glu scavenging activity but rather to a therapeutic activity exerted within the brain. Two major neuroprotective mechanisms could be here involved: (a) OxAc can contribute to an improvement of NAD-linked mitochondrial energetics via an enhancement of the malateaspartate shuttle. (b) Being a ketoacid, OxAc has the ability to scavenge hydrogen peroxide (H2O2), one of the main reactive oxygen species generated by traumatic brain injury (Desagher et al., 1997). Several rather compelling arguments, however, can be raised to support the contention that OxAc exerts its neuroprotective effects mainly via blood Glu scavenging. (1) The OxAc-induced neurological recovery after CHI is not observed in rats treated with OxAc and glutamate. This finding is in line with the view that the presence of excess Glu in blood prevents OxAc to effectively exert its blood Glu scavenging action which is necessary for a therapeutic enhanced efflux of excess Glu from brain into blood. Would OxAc exert its therapeutic effect in brain, it is not clear why this action would be prevented by intravenous excess Glu since the entrance of OxAc first from blood into the brain and then further into neurons takes place via dicarboxylate transporters such as the NaDC-3 which are not inhibited by Glu (Burckhardt et al., 2005; Pajor et al., 2001). One can further argue that the Gluinduced neutralization of the therapeutic effect of OxAc must be exerted within the blood and not within the brain since Glu does not significantly penetrate from blood into brain neither in normal physiological conditions (Smith, 2000) nor after the breakdown of the blood–brain barrier (Ronne Engstrom et al., 2005). (2) The OxAc-induced neurological recovery after CHI takes place following the administration of OxAc within the time window during which excess Glu is present in brain i.e., up to 2 h post CHI. Though we did not measure the kinetics of brain Glu elevation after CHI, numerous studies demonstrate that the excess Glu in rat brain fluid does not last more than 2 h following either CHI or stroke (Faden et al., 1989; Farooque et al., 1996; Guyot et al., 2001; Phillis et al., 1996; Rose et al., 2002) but see (Alves et al., 2005). Assuming that OxAc therapeutic action is unrelated to blood Glu scavenging but rather to an improvement of mitochondrial energetics, the observation that OxAc has no therapeutic effect when administered 2 h after CHI cannot be easily reconciled with the observation that mitochondrial dysfunction is observed for several hours after CHI (Singh et al., 2006; Takamatsu et al., 1998; Xiong et al., 2005). (3) The observation that the neurological recovery after CHI depends on the presence in blood of both OxAc and GOT (Figs. 6 and 7) is in line with two predictions: (a) that neuroprotection can be achieved upon OxAc/GOT-mediated blood Glu scavenging; (b) that the rate of GOT-mediated blood Glu scavenging via transamination will not change if the product of the OxAc and GOT concentrations is kept constant, i.e., that lowering the OxAc concentration in the solution injected into blood can be compensated by increasing the GOT concentration in that solution. The tight therapeutic synergism between blood OxAc and GOT is also difficult to reconcile with the suggestion of an intraparenchymal site of action, as OxAc and GOT should be both translocated from blood into brain to exert beneficial effects. The respective kinetics of intraparenchymal entry of OxAc (which is specifically transported via a dicarboxylate transporter) and GOT (which cannot gain access into the brain via an intact BBB) are probably incompatible with a synergy of action since the BBB opening that begins at the time of the trauma is transient, and lasts no more than 30 min (Barzo et al., 1996), while GOT is administered after 60–90 min post trauma. (4) The observation that the neurological recovery after CHI is highly correlated with the decrease of blood Glu levels (Fig. 4) is strongly in line with the concept that blood Glu scavenging enhances the efflux of excess Glu from brain into blood and provides thereby neuroprotection. This strong correlation cannot be explained by an intraparenchymal site of action of OxAc. Though we do not rule out the possibility that OxAc exerts some neuroprotective effects within the brain, we believe that the major therapeutic action of OxAc is decisively linked to its blood Glu scavenging activity. It is of interest to note that saline-treated rats recover from TBI to a significant extent, though neither as fast nor as much as the OxAc-treated rats. It is a tantalizing hypothesis that the spontaneous recovery of rats after TBI would rely on the same mechanism as that amplified by OxAc. OxAc is here shown to have a relatively short time window that appears to be tightly linked to the limited duration of excess Glu in the rat brain after CHI (Faden et al., 1989; Farooque et al., 1996; Guyot et al., 2001; Phillis et al., 1996; Rose et al., 2002). Since, excess Glu in human brain can be observed after CHI for hours and even days (Baker et al., 1993; Bullock et al., 1998; Palmer et al., 1993; Richards et al., 2003; Rose et al., 2002; Vespa et al., 1998), and is in correlation with the poor neurological outcome (Koura et al., 1998; Zauner et al., 1996; Zhang et al., 2001), one might possibly expect for Please cite this article as: Alexander Zlotnik et al., Brain neuroprotection by scavenging blood glutamate, Experimental Neurology (2006), doi:10.1016/j. expneurol.2006.08.021 ARTICLE IN PRESS A. Zlotnik et al. / Experimental Neurology xx (2006) xxx–xxx OxAc a much longer therapeutic time window in human patients than in rats. One might further expect that the administration of this blood Glu scavenger may display in man a therapeutic effect which has so far not been observed for glutamate receptor antagonists. One possible benefit is that the enhanced brain-toblood Glu efflux produced by blood Glu scavenging is selflimiting since it slows down in parallel with the decrease of brain Glu. Thus, it will eliminate excess Glu without preventing Glu from exerting a role in neurorepair (Biegon et al., 2004), a factor that has been suggested (Ikonomidou and Turski, 2002) to account for the failure of glutamate receptor antagonists in human clinical studies. Acknowledgments This work was supported in part by grants to VIT from the Nella and Leon Benoziyo Center for Neurological Diseases; the Irwin Green Fund for Studying the Development of the Brain, the Yeshaya Horowitz Foundation, the Carl and Micaela EinhornDominic Institute for Brain Research, the Weizmann-Negri Fund and the Israel Cancer Research Fund. The data obtained are part of A.Z.'s PhD thesis. VIT is the incumbent of the Louis and Florence Katz-Cohen Chair of Neuropharmacology. References Alves, O.L., Bullock, R., Clausen, T., Reinert, M., Reeves, T.M., 2005. Concurrent monitoring of cerebral electrophysiology and metabolism after traumatic brain injury: an experimental and clinical study. J. Neurotrauma 22, 733–749. Baker, A.J., Moulton, R.J., MacMillan, V.H., Shedden, P.M., 1993. Excitatory amino acids in cerebrospinal fluid following traumatic brain injury in humans. J. Neurosurg. 79, 369–372. Barzo, P., Marmarou, A., Fatouros, P., Corwin, F., Dunbar, J., 1996. Magnetic resonance imaging-monitored acute blood–brain barrier changes in experimental traumatic brain injury. J. Neurosurg. 85, 1113–1121. Berl, S., Lajtha, A., Waelsch, H., 1961. Amino acid and protein metabolism-VI cerebral compartments of glutamic acid metabolism. J. Neurochem. 7, 186–197. Biegon, A., Fry, P.A., Paden, C.M., Alexandrovich, A., Tsenter, J., Shohami, E., 2004. Dynamic changes in N-methyl-D-aspartate receptors after closed head injury in mice: implications for treatment of neurological and cognitive deficits. Proc. Natl. Acad. Sci. U. S. A. 101, 5117–5122. Bullock, R., Zauner, A., Woodward, J.J., Myseros, J., Choi, S.C., Ward, J.D., Marmarou, A., Young, H.F., 1998. Factors affecting excitatory amino acid release following severe human head injury. J. Neurosurg. 89, 507–518. Burckhardt, B.C., Lorenz, J., Kobbe, C., Burckhardt, G., 2005. Substrate specificity of the human renal sodium dicarboxylate cotransporter, hNaDC3, under voltage-clamp conditions. Am. J. Physiol.: Renal. Physiol. 288, F792–F799. Castillo, J., Davalos, A., Naveiro, J., Noya, M., 1996. Neuroexcitatory amino acids and their relation to infarct size and neurological deficit in ischemic stroke. Stroke 27, 1060–1065. Castillo, J., Davalos, A., Noya, M., 1997. Progression of ischaemic stroke and excitotoxic aminoacids. Lancet. 349, 79–83. Castillo, J., Davalos, A., Alvarez-Sabin, J., Pumar, J.M., Leira, R., Silva, Y., Montaner, J., Kase, C.S., 2002. Molecular signatures of brain injury after intracerebral hemorrhage. Neurology 58, 624–629. Danbolt, N.C., 2001. Glutamate uptake. Prog. Neurobiol. 65, 1–105. Desagher, S., Glowinski, J., Premont, J., 1997. Pyruvate protects neurons against hydrogen peroxide-induced toxicity. J. Neurosci. 17, 9060–9067. Faden, A.I., Demediuk, P., Panter, S.S., Vink, R., 1989. The role of excitatory 7 amino acids and NMDA receptors in traumatic brain injury. Science 244, 798–800. Farooque, M., Hillered, L., Holtz, A., Olsson, Y., 1996. Changes of extracellular levels of amino acids after graded compression trauma to the spinal cord: an experimental study in the rat using microdialysis. J. Neurotrauma 13, 537–548. Ferrarese, C., Aliprandi, A., Tremolizzo, L., Stanzani, L., De Micheli, A., Dolara, A., Frattola, L., 2001. Increased glutamate in CSF and plasma of patients with HIV dementia. Neurology 57, 671–675. Furukawa, T., Hoshino, S., Kobayashi, S., Asakura, T., Takahashi, M., Atsumi, T., Teramoto, A., 2003. The glutamate AMPA receptor antagonist, YM872, attenuates cortical tissue loss, regional cerebral edema, and neurological motor deficits after experimental brain injury in rats. J. Neurotrauma 20, 269–278. Gottlieb, M., Wang, Y., Teichberg, V.I., 2003. Blood-mediated scavenging of cerebrospinal fluid glutamate. J. Neurochem. 87, 119–126. Graham Jr., L.T., Aprison, M.H., 1966. Fluorometric determination of aspartate, glutamate, and gamma-aminobutyrate in nerve tissue using enzymic methods. Anal. Biochem. 15, 487–497. Guyot, L.L., Diaz, F.G., O'Regan, M.H., McLeod, S., Park, H., Phillis, J.W., 2001. Real-time measurement of glutamate release from the ischemic penumbra of the rat cerebral cortex using a focal middle cerebral artery occlusion model. Neurosci. Lett. 299, 37–40. Hosoya, K., Sugawara, M., Asaba, H., Terasaki, T., 1999. Blood–brain barrier produces significant efflux of L-aspartic acid but not D-aspartic acid: in vivo evidence using the brain efflux index method. J. Neurochem. 73, 1206–1211. Ikonomidou, C., Turski, L., 2002. Why did NMDA receptor antagonists fail clinical trials for stroke and traumatic brain injury? Lancet Neurol. 1, 383–386. Johnston, M.V., Trescher, W.H., Ishida, A., Nakajima, W., 2001. Neurobiology of hypoxic–ischemic injury in the developing brain. Pediatr. Res. 49, 735–741. Koura, S.S., Doppenberg, E.M., Marmarou, A., Choi, S., Young, H.F., Bullock, R., 1998. Relationship between excitatory amino acid release and outcome after severe human head injury. Acta Neurochir., Suppl. 71, 244–246. Margaill, I., Parmentier, S., Callebert, J., Allix, M., Boulu, R.G., Plotkine, M., 1996. Short therapeutic window for MK-801 in transient focal cerebral ischemia in normotensive rats. J. Cereb. Blood Flow Metab. 16, 107–113. O'Kane, R.L., Martinez-Lopez, I., DeJoseph, M.R., Vina, J.R., Hawkins, R.A., 1999. Na(+)-dependent glutamate transporters (EAAT1, EAAT2, and EAAT3) of the blood–brain barrier. A mechanism for glutamate removal. J. Biol. Chem. 274, 31891–31895. Pajor, A.M., Gangula, R., Yao, X., 2001. Cloning and functional characterization of a high-affinity Na(+)/dicarboxylate cotransporter from mouse brain. Am. J. Physiol.: Cell Physiol. 280, C1215–C1223. Palmer, A.M., Marion, D.W., Botscheller, M.L., Swedlow, P.E., Styren, S.D., DeKosky, S.T., 1993. Traumatic brain injury-induced excitotoxicity assessed in a controlled cortical impact model. J. Neurochem. 61, 2015–2024. Phillis, J.W., Smith-Barbour, M., O'Regan, M.H., 1996. Changes in extracellular amino acid neurotransmitters and purines during and following ischemias of different durations in the rat cerebral cortex. Neurochem. Int. 29, 115–120. Richards, D.A., Tolias, C.M., Sgouros, S., Bowery, N.G., 2003. Extracellular glutamine to glutamate ratio may predict outcome in the injured brain: a clinical microdialysis study in children. Pharmacol. Res. 48, 101–109. Ronne Engstrom, E., Hillered, L., Enblad, P., Karlsson, T., 2005. Cerebral interstitial levels of glutamate and glutamine after intravenous administration of nutritional amino acids in neurointensive care patients. Neurosci. Lett. 384, 7–10. Rose, M.E., Huerbin, M.B., Melick, J., Marion, D.W., Palmer, A.M., Schiding, J.K., Kochanek, P.M., Graham, S.H., 2002. Regulation of interstitial excitatory amino acid concentrations after cortical contusion injury. Brain Res. 943, 15–22. Sattler, R., Tymianski, M., 2001. Molecular mechanisms of glutamate receptormediated excitotoxic neuronal cell death. Mol. Neurobiol. 24, 107–129. Serena, J., Leira, R., Castillo, J., Pumar, J.M., Castellanos, M., Davalos, A., Please cite this article as: Alexander Zlotnik et al., Brain neuroprotection by scavenging blood glutamate, Experimental Neurology (2006), doi:10.1016/j. expneurol.2006.08.021 ARTICLE IN PRESS 8 A. Zlotnik et al. / Experimental Neurology xx (2006) xxx–xxx 2001. Neurological deterioration in acute lacunar infarctions: the role of excitatory and inhibitory neurotransmitters. Stroke 32, 1154–1161. Shapira, Y., Shohami, E., Sidi, A., Soffer, D., Freeman, S., Cotev, S., 1988. Experimental closed head injury in rats: mechanical, pathophysiologic, and neurologic properties. Crit. Care Med. 16, 258–265. Shapira, Y., Artru, A.A., Lam, A.M., 1992. Ketamine decreases cerebral infarct volume and improves neurological outcome following experimental head trauma in rats. J. Neurosurg. Anesthesiol. 4, 231–240. Shaw, P.J., Forrest, V., Ince, P.G., Richardson, J.P., Wastell, H.J., 1995. CSF and plasma amino acid levels in motor neuron disease: elevation of CSF glutamate in a subset of patients. Neurodegeneration 4, 209–216. Singh, I.N., Sullivan, P.G., Deng, Y., Mbye, L.H., Hall, E.D., 2006. Time course of post-traumatic mitochondrial oxidative damage and dysfunction in a mouse model of focal traumatic brain injury: implications for neuroprotective therapy. J. Cereb. Blood Flow Metab. (Electronic publication ahead of print). Smith, Q.R., 2000. Transport of glutamate and other amino acids at the blood– brain barrier. J. Nutr. 130, 1016S–1022S. Spranger, M., Krempien, S., Schwab, S., Maiwald, M., Bruno, K., Hacke, W., 1996. Excess glutamate in the cerebrospinal fluid in bacterial meningitis. J. Neurol. Sci. 143, 126–131. Spreux-Varoquaux, O., Bensimon, G., Lacomblez, L., Salachas, F., Pradat, P.F., Le Forestier, N., Marouan, A., Dib, M., Meininger, V., 2002. Glutamate levels in cerebrospinal fluid in amyotrophic lateral sclerosis: a reappraisal using a new HPLC method with coulometric detection in a large cohort of patients. J. Neurol. Sci. 193, 73–78. Stoffel, M., Plesnila, N., Eriskat, J., Furst, M., Baethmann, A., 2002. Release of excitatory amino acids in the penumbra of a focal cortical necrosis. J. Neurotrauma 19, 467–477. Takamatsu, H., Kondo, K., Ikeda, Y., Umemura, K., 1998. Hydroxyl radical generation after the third hour following ischemia contributes to brain damage. Eur. J. Pharmacol. 352, 165–169. Vespa, P., Prins, M., Ronne-Engstrom, E., Caron, M., Shalmon, E., Hovda, D.A., Martin, N.A., Becker, D.P., 1998. Increase in extracellular glutamate caused by reduced cerebral perfusion pressure and seizures after human traumatic brain injury: a microdialysis study. J. Neurosurg. 89, 971–982. Westergren, I., Johansson, B.B., 1992. NBQX, an AMPA antagonist, reduces glutamate-mediated brain edema. Brain Res. 573, 324–326. Westergren, I., Johansson, B.B., 1993. Blockade of AMPA receptors reduces brain edema following opening of the blood–brain barrier. J. Cereb. Blood Flow Metab. 13, 603–608. Xiong, Y., Shie, F.S., Zhang, J., Lee, C.P., Ho, Y.S., 2005. Prevention of mitochondrial dysfunction in post-traumatic mouse brain by superoxide dismutase. J. Neurochem. 95, 732–744. Zauner, A., Bullock, R., Kuta, A.J., Woodward, J., Young, H.F., 1996. Glutamate release and cerebral blood flow after severe human head injury. Acta Neurochir. Suppl. 67, 40–44. Zhang, H., Zhang, X., Zhang, T., Chen, L., 2001. Excitatory amino acids in cerebrospinal fluid of patients with acute head injuries. Clin. Chem. 47, 1458–1462. Please cite this article as: Alexander Zlotnik et al., Brain neuroprotection by scavenging blood glutamate, Experimental Neurology (2006), doi:10.1016/j. expneurol.2006.08.021