Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
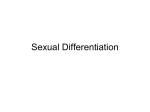
VIEWS AND REVIEWS Effect of rejuvenation hormones on spermatogenesis Jared L. Moss, M.D., Lindsey E. Crosnoe, B.S., and Edward D. Kim, M.D. University of Tennessee Graduate School of Medicine, Knoxville, Tennessee Objective: To review the current literature for the effect of hormones used in rejuvenation clinics on the maintenance of spermatogenesis. Design: Review of published literature. Setting: Not applicable. Patient(s): Men who have undergone exogenous testosterone (T) and/or anabolic androgenic steroid (AAS) therapies. Intervention(s): None. Main Outcome Measure(s): Semen analysis, pregnancy outcomes, and time to recovery of spermatogenesis. Result(s): Exogenous testosterone and anabolic androgenic steroids suppress intratesticular testosterone production, which may lead to azoospermia or severe oligozoospermia. Therapies that protect spermatogenesis involve human chorionic gonadotropin (hCG) therapy and selective estrogen receptor modulators (SERMs). The studies examining the effect of human growth hormone (HGH) on infertile men are uncontrolled and unconvincing, but they do not appear to negatively impact spermatogenesis. At present, routine use of aromatase inhibitors is not recommended based on a lack of long-term data. Conclusion(s): The use of hormones for rejuvenation is increasing with the aging of the Baby Boomer population. Men desiring children at a later age may be unaware of the side-effect profile of hormones used at rejuvenation centers. Testosterone and anabolic androgenic steroids have well-established detrimental effects on spermatogenesis, but recovery may be possible with cessation. Clomiphene citrate, human growth hormone (HGH)/insulin-like growth factor-1 (IGF-1), human chorionic gonadotropin (hCG), and aromatase inhibitors do not appear to Use your smartphone have significant negative effects on sperm production, but quality data are lacking. (Fertil to scan this QR code SterilÒ 2013;-:-–-. Ó2013 by American Society for Reproductive Medicine.) and connect to the Key Words: Hormones, rejuvenation, spermatogenesis Discuss: You can discuss this article with its authors and with other ASRM members at http:// fertstertforum.com/mossj-rejuvenation-hormones-spermatogenesis/ I n 1970, fewer than 15% of all men fathering children were over 35 years of age. Today, that percentage has risen to almost 25%. Likewise, the number of men in the 50 to 54 age group has seen a notable increase in fatherhood (1). Not only is the male population aging and reproducing later, but many men are also searching for the fountain of youth. A 2009 article in the Chicago Tribune by Bruce Jaspen (2) reported that the sale of anti-aging products sales in the U.S. alone has exceeded $50 billion annually. Many of these products are hormones that are being prescribed in antiaging centers known as rejuvenation clinics. Because of the off-label illicit use of these medications and the unregulated nature of this industry, little is known about the effect of these hormones on male fertility. This article reviews common antiaging hormones used in rejuvenation clinics and their mechanism of effect on spermatogenesis (Table 1). MATERIALS AND METHODS A PubMed literature search was conducted for the time period of Received January 15, 2013; revised and accepted April 2, 2013. J.L.M. has nothing to disclose. L.E.C. has nothing to disclose. E.D.K. has nothing to disclose. Reprint requests: Edward D. Kim, M.D., 1928 Alcoa Highway, Suite 222, Knoxville, Tennessee 37920 (E-mail: [email protected]). Fertility and Sterility® Vol. -, No. -, - 2013 0015-0282/$36.00 Copyright ©2013 American Society for Reproductive Medicine, Published by Elsevier Inc. http://dx.doi.org/10.1016/j.fertnstert.2013.04.003 discussion forum for this article now.* * Download a free QR code scanner by searching for “QR scanner” in your smartphone’s app store or app marketplace. 1984–2012, focusing on 45 studies examining the effect of hormones used for rejuvenation on semen analysis, pregnancy outcomes, and time to recovery of spermatogenesis. Those publications representing level 1 evidence were marked with the annotation (LOE 1). Six hormones were reviewed: exogenous testosterone, anabolic steroids, human growth hormone (HGH), clomiphene citrate (CC), human chorionic gonadotropin (hCG), and aromatase inhibitors (AI). These hormones were selected based on clinical experience and information publicly promoted by rejuvenation centers. There were insufficient published quality data for a metaanalysis, so a systematic review was performed for all hormones. Institutional review board approval was not necessary for a review paper. VOL. - NO. - / - 2013 1 REV 5.1.0 DTD FNS28165_proof 25 April 2013 5:24 am ce VW VIEWS AND REVIEWS TABLE 1 Overview of the effect(s) of rejuvenation hormones on spermatogenesis. Hormone Mode of action Testosterone Negative Anabolic androgenic steroids (AAS) Negative Clomiphene citrate (CC) Neutral/positive Growth hormone/Insulin-like growth factor (HGH/IGF-1) Aromatase inhibitor (AI) Neutral/positive Neutral Human chorionic gonadotropin (hCG) Neutral/positive Mechanism of effect on spermatogenesis Suppression of the HPG axis results in decreased ITT concentration, which decreases spermatogenesis. Suppression of the HPG axis results in decreased ITT concentration, which decreases spermatogenesis. This SERM increases testicular testosterone production, which may be beneficial for spermatogenesis. HGH stimulates IGF-1 formation, which may improve sperm maturation in a paracrine-autocrine manner. This cytochrome P450 enzyme blocks the conversion of androgens to estrogen, consequently increasing serum levels of LH, FSH, and testosterone and may stimulate spermatogenesis. This LH analog stimulates Leydig cell production of testosterone, which can initiate and maintain spermatogenesis in hypogonadotropic hypogonadal men. Note: FSH ¼ follicle-stimulating hormone; HPG ¼ hypothalamic-pituitary-gonadal; ITT ¼ intratesticular testosterone levels; LH ¼ luteinizing hormone; SERM ¼ selective estrogen receptor modulator. Moss. Rejuvenation hormones and spermatogenesis. Fertil Steril 2013. EXOGENOUS TESTOSTERONE Clinical Evidence Background Exogenous testosterone supplementation decreases sperm production. However, when it was evaluated as a male contraceptive agent, studies showed that most men have a return to normal sperm production within 1 year after discontinuing testosterone supplementation (LOE 1) (Table 2) (9). For example, a study by the World Health Organization (WHO) Task Force evaluated 271 men who had received 200 mg of testosterone enanthate weekly (LOE 1) (10). After 6 months, 157 (65%) of the men were azoospermic, and the mean time to azoospermia was 120 days. After 6 months of treatment, the patients entered the recovery phase where exogenous testosterone was discontinued. Although 84% of men were able to achieve a sperm density >20 million/mL after a median of 3.7 months, only 46% of patients were able to achieve their baseline sperm density. Gu et al. (11) administered testosterone 500 mg monthly of undecanoate for 30 months to a group of 855 Chinese men (LOE 1). Using a primary outcome of pregnancy rate, nine pregnancies were reported in >1,500 person-years of exposure in the 24-month efficacy phase (855 men) for a cumulative contraceptive failure rate of 1.1 per 100 men. Ninety-five percent of men achieved azoospermia or severe oligozoospermia (<1 106 sperm/mL), and the median time to onset of azoospermia or severe oligozoospermia was 108 days. The median time to recovery of spermatogenesis calculated from the beginning of the recovery phase was 196 days. It should be noted that the contraceptive trials were in men of Chinese ethnicity and that extrapolation of findings to men of non-Chinese ethnicities may not be reliable. Additionally, the use of testosterone therapy in a broad population of men may have varying results. A significant limitation of the published literature concerning this topic is a lack of pregnancy outcome data. The published literature represents the best available evidence to date regarding the recovery of spermatogenesis after testosterone supplementation, but it is largely limited to male contraceptive studies. This situation may not be Exogenous testosterone therapy is approved by the US Food and Drug Administration (FDA) for the treatment of symptomatic hypogonadism. Exogenous testosterone is one of the most common therapies used for the purpose of male rejuvenation. Examples of exogenous testosterone include topical gels, subcutaneous testosterone pellets, and intramuscular injectable testosterone. Over the past 5 years, there has been an increase in testosterone prescriptions by 170%. This correlates with the recent introduction of newer commercial products and an increased public awareness of androgen deficiency syndromes (3). It is estimated that more than 13.8 million men R45 years of age visiting a primary care doctor in the United States have symptomatic androgen deficiency (4). Importantly, many testosterone users/abusers and clinicians are unaware that exogenous testosterone suppresses the hypothalamic-pituitary-gonadal (HPG) axis and may result in infertility. In a recent survey of U.S. urologists, Ko et al. (5) observed that approximately 25% have used exogenous testosterone to treat low testosterone levels associated with male infertility. Mechanism of Action Exogenous testosterone inhibits spermatogenesis by suppressing the HPG axis. Specifically, testosterone therapy results in negative feedback on the HPG axis. It inhibits gonadotropinreleasing hormone (GnRH), thereby inhibiting the secretion of follicle-stimulating hormone (FSH) and luteinizing hormone (LH) (Fig. 1). Suppression of gonadotropins results in a decrease in intratesticular testosterone levels (ITT) and overall testosterone production. Normally, ITT concentrations are approximately 50 to 100 times serum levels. As exogenous testosterone therapies suppress ITT production, spermatogenesis can be dramatically compromised (6). Intratesticular testosterone is an absolute prerequisite for normal spermatogenesis, and its inhibition can result in azoospermia (7, 8). VOL. - NO. - / - 2013 2 REV 5.1.0 DTD FNS28165_proof 25 April 2013 5:24 am ce VW Fertility and Sterility® print & web 4C=FPO FIGURE 1 Rejuvenation hormones and mechanism of action. Exogenous testosterone and anabolic androgenic steroids (AAS) negatively affect the hypothalamic-pituitary-gonadal (HPG) axis. Selective estrogen receptor modulators (SERMs) block the negative feedback of estrogen on the HPG axis. Human chorionic gonadotropin (hCG) stimulates Leydig cells. Aromatase inhibitors prevent the conversion of testosterone to estrogen. Moss. Rejuvenation hormones and spermatogenesis. Fertil Steril 2013. reflective of the hypogonadal male seen in clinical practice. The caveat is that the consistency of spermatogenesis recovery in clinical practice may not be as predictable as seen in contraceptive studies (12). It is important to emphasize that semen analysis data do not correlate with pregnancy outcomes and that none of the literature assesses time to fecundity. Recommendations Exogenous testosterone should be avoided in men desiring future fertility, given the potential detrimental side effects and lack of data regarding long-term effects on spermatogenesis. ANABOLIC ANDROGENIC STEROIDS Background Synthetic anabolic androgenic steroids (AAS) have been FDA-approved for the treatment of testosterone replacement, renal-insufficiency associated anemia, hereditary angioedema, and weight loss. These cholesterol derivatives of testosterone are both anabolic and androgenic, which help patients to build lean muscle and enhance masculinization (13). Popular types of AAS are oral oxandrolone (Oxandrin), oral methandienone (Dianabol), injectable stanozolol (Winstrol-V), injectable nandrolone decanoate (Deca-Durabolin), and injectable boldenone TABLE 2 Model-based probability of spermatogenic recovery to various thresholds after discontinuation of exogenous testosterone. Probability of recovery (%, 96% CI) Individual baseline value 20 million/mL 10 million/mL 3 million/mL Within 6 mo Within 12 mo Within 16 mo Within 24 mo 54 (46–60) 67 (61–72) 79 (73–83) 89 (84–92) 83 (75–89) 90 (85–93) 95 (92–97) 98 (95–99) 95 (89–98) 96 (92–98) 99 (97–100) 100* 100* 100* 100* 100* Note: Adapted from Liu PY et al. Lancet 2006;367:1412–20. * Confidence interval could not be obtained from the model. Moss. Rejuvenation hormones and spermatogenesis. Fertil Steril 2013. VOL. - NO. - / - 2013 3 REV 5.1.0 DTD FNS28165_proof 25 April 2013 5:24 am ce VW VIEWS AND REVIEWS undecylenate (Equipoise). Although the practice has been prevalent, Kanayama et al. (14) showed the use of AAS is on the decline among high school athletes. More recently, a new population of aging males has surfaced who are self-administering AAS as a rejuvenation therapy. The lifetime prevalence of AAS use in males is estimated to be between 3.0% to 4.2% (15). There are likely hundreds of thousands of men in their 30s and 40s who began using AAS in high school and continue to be currently dependent on AAS (14). In 2003, the public became aware of this growing problem among high profile professional athletes when the Bay Area Laboratory Co-operative (BALCO) in Burlingame, California, was implicated in a steroid scandal that resulted in numerous arrests and tainted many professional careers (16). A growing trend is the use of these illegal drugs from rejuvenation clinics for noncompetitive reasons by the ‘‘regular Joe’’ (17). For example, a rejuvenation center in Florida was raided by authorities as part of a network of online clinics and pharmacies for illegal sales of steroids and growth hormones (18). HUMAN GROWTH HORMONE/INSULIN-LIKE GROWTH FACTOR 1 Mechanism of Action Mechanism of Action The mechanism by which AAS inhibit spermatogenesis is believed to be the same as exogenous testosterone (Fig. 1). These hormonal changes can lead to azoospermia, oligozoospermia, severe testicular atrophy, hypogonadotropic hypogonadism, and increased teratozoospermia (19). Growth hormone is a protein that is synthesized and secreted by cells called somatotrophs in the anterior pituitary gland. A critical concept in understanding growth hormone activity is that it has two distinct types of effects, direct and indirect. Direct effects are the result of growth hormone binding its receptor on target cells. Indirect effects are mediated primarily by insulin-like growth factor-1 (IGF-1), a hormone that is secreted from the liver and other tissues in response to growth hormone. A majority of the effects of HGH are due to IGF-1 acting on its target cells. In the testicle, levels of IGF-1 are measurably elevated when stimulated by HGH, which may stimulate maturation of spermatozoa in a paracrineautocrine manner (31). Clinical Evidence An understanding of how AAS affect spermatogenesis is complicated by several factors. Data collection is usually through uncontrolled, observational studies of AAS users from gymnasiums or the Internet, which introduces inherent selection biases. These studies are additionally complicated by dishonesty in reporting nonuse and lack of toxicology testing for confirmation of compliance. Many users also may not be fully disclosing concurrent medications such as antiestrogens, aromatase inhibitors, and human chorionic gonadotropin (hCG) (14). It is estimated that AAS users often take 600–5,000 mg of AAS per week (20–23). These doses are supraphysiologic in that they are 50 to 100 times greater than the 40–50 mg weekly production of testosterone by the normal male testes (24). Biological potency of anabolic agents cannot be accurately compared based on the weight of the product consumed. Spermatogenesis usually recovers spontaneously within 4 to 6 months after cessation of AAS, but recovery has been reported to take up to 3 years or longer (25–27). Reasons for the extended recovery time are not yet known, but are likely related to the variety of medication combinations and high doses. Recommendations Men desiring future fertility should not use AAS, given the significant potential for long-term effects on spermatogenesis. Background Human growth hormone (HGH) is FDA-approved for the treatment of the hormonal deficiency that causes short stature in children, adult short-bowel syndrome, adult growth hormone deficiency due to rare pituitary tumors or the treatment thereof, and muscle-wasting disease associated with human immunodeficiency virus/acquired immunodeficiency syndrome (HIV/AIDS). With limited success, HGH has been used off-label to treat men with poor sperm counts (28). Additionally, HGH has been abused by athletes looking for a performance advantage as well as patients of rejuvenation clinics seeking to improve their appearance and well-being (29). As an example, a rejuvenation clinic is Los Angeles, California, states on their Web site that HGH can increase muscle, improve mental acuity, boost the sex drive, burn fat more quickly, and increase energy and strength (30). Quality data supporting these claims efficacy and safety are lacking. Clinical Evidence Radicioni et al. (28) examined the use of recombinant HGH in infertile men with idiopathic oligozoospermia. This uncontrolled study was designed to evaluate the short-term efficacy of recombinant HGH on spermatogenesis in 10 infertile men with severe oligozoospermia (1–5 106) and normal or minimally elevated gonadotropin levels. All of the men received injections of 4 IU of recombinant HGH three times per week for 180 days. The posttreatment semen analysis showed that five responders experienced a significant increase in seminal parameters, including sperm concentration and motility. They concluded that HGH may be a reasonable option in men with idiopathic oligozoospermia who have failed other treatments. In another uncontrolled trial, Ovesen et al. (31) examined HGH treatment in 18 subfertile males with oligozoospermia (<5 106 sperm/mL) or asthenozoospermia (percentage motile sperm <30 and >15 106 sperm/mL). The results showed that seminal IGF-1 levels and sperm motility increased significantly in both groups although the sperm counts did not. There were three pregnancies in the azthenozoospermic group and none in the oligozoospermic group. VOL. - NO. - / - 2013 4 REV 5.1.0 DTD FNS28165_proof 25 April 2013 5:24 am ce VW Fertility and Sterility® Recommendations Quality data regarding the effect of HGH on spermatogenesis when it is used as a rejuvenation medication are completely lacking. There is no persuasive evidence that HGH, along with gonadotropin, is efficacious in promoting spermatogenesis in males with hypogonadotropic hypogonadism. The studies examining the HGH treatment in infertile men were uncontrolled and are unconvincing, but they do suggest a potential benefit for sperm count and motility. CLOMIPHENE CITRATE Background Clomiphene citrate (CC) is a selective estrogen receptor modulator (SERM) that has been FDA-approved to initiate ovulation in women (32). Additionally, this SERM is used off-label continuously in men of reproductive age to treat hypogonadism and low sperm concentration. Clomiphene citrate is also used by men taking AAS in a cyclic fashion as an aid to recovery of natural testosterone production after AAS or exogenous testosterone cessation. It is usually applied in short courses in this population to stimulate normal sex hormone secretion by producing a gonadotropin surge (33, 34). Web sites such as Steroid.com outline how to use and obtain CC while ‘‘cycling’’ steroids. Although CC can be used in a continuous or cyclic manner, there is no convincing evidence to date showing that one is superior to the other. Mechanism of Action Selective estrogen receptor modulators competitively bind to estrogen receptors on the hypothalamus and pituitary gland (Fig. 1). As a result, the pituitary sees less estrogen and makes more LH, which increases testosterone production by the testes. It is not as effective in raising serum testosterone levels when LH and FSH levels are already elevated, as seen in primary testis failure. By increasing ITT, the use of CC in hypogonadal men with poor sperm counts has been theorized to promote spermatogenesis (12). demonstrated that CC is an effective and safe alternative to testosterone supplementation therapy in hypogonadal men. However, it should be emphasized that studies of limited length have associated osteoporosis with long-term CC use. A randomized, prospective trial of CC for hypogonadal men with normal semen parameters is necessary to validate the recommendation for the use of SERMs for fertility preservation. This study would need to demonstrate that semen profiles are not adversely affected. Clomiphene citrate has been commonly used for the empiric treatment of male infertility; however, the double-blind, placebo-controlled studies that demonstrate the effects can be variable, unpredictable, and show no efficacy. Recommendations The off-label use of CC to improve serum testosterone levels appears to be safe and effective for use up to 2 years. This treatment represents the best alternative to androgenic medications for men who wish to maintain fertility while being treated for symptomatic hypogonadism/rejuvenation. HUMAN CHORIONIC GONADOTROPIN Background Human chorionic gonadotropin is FDA-approved as an injectable prescription drug for the treatment of female infertility. Human chorionic gonadotropin, a hormone produced by the human placenta and found in the urine of pregnant women, can also be derived from recombinant sources. It is used off-label in several ways. Similar to CC, hCG is used by AAS abusers to counteract the hypogonadotropic hypogonadism experienced after withdrawal of AAS. Additionally, the FDA has reported that hCG is being marketed as a rejuvenation drug to produce dramatic weight loss as part of an oral hCG diet. The FDA states on their Web site that this use is fraudulent and not FDA approved. The FDA is advising consumers to steer clear of hCG weight-loss products (36). Mechanism of Action Clinical Evidence Katz et al. (35) from the Memorial Sloan-Kettering Cancer Center observed that long-term use of CC was safe and effective in improving serum testosterone levels (LOE 1). In this moderately sized analysis, 86 men aged 22 to 37 years with hypogonadism (T levels <300 ng/dL) were evaluated and treated for a mean duration of 19 months. The treatment with CC started at 25 mg every other day and was titrated to 50 mg every other day. The target testosterone level was 550 ng/dL. Once the desired testosterone levels were achieved, the testosterone/gonadotropin levels were measured twice per year. In response to questions on the Androgen Deficiency in Aging Males (ADAM) questionnaire, the men reported improvements in every area except for loss of height. There was significant improvement in five of the 10 variables, including decreased libido, lack of energy, decreased life enjoyment, feeling sad/grumpy, and decreased sports performance. Over a long-term follow-up, this study Follicle-stimulating hormone and LH are made up of an alpha chain that is identical to the structure of hCG and thyroid-stimulating hormone (TSH). Accordingly, hCG is primarily an LH analog that stimulates Leydig cell production of testosterone (Fig. 1). When given in the exogenous form, hCG increases ITT concentrations and serum testosterone levels by stimulating Leydig cells (37). Clinical Evidence In a small case series by Depenbusch et al. (38), 13 azoospermic men with hypogonadotropic hypogonadism were initially administered hCG and human menopausal gonadotropin (hMG) to induce spermatogenesis. Human chorionic gonadotropin was then administered at 500–2,500 IU subcutaneously twice weekly alone for up to 2 years (range: 3–24 months). After 12 months, the sperm counts decreased gradually but remained present in all patients, except one VOL. - NO. - / - 2013 5 REV 5.1.0 DTD FNS28165_proof 25 April 2013 5:24 am ce VW VIEWS AND REVIEWS man who became azoospermic. This study identified that FSH is essential for maintenance of quantitatively normal spermatogenesis and that high doses of hCG are not needed to stimulate and maintain spermatogenesis. Roth et al. (39) induced experimental gonadotropin deficiency in 37 normal men with gonadotropin-releasing hormone (GnRH) antagonists and randomized the men to receive one of four doses of hCG: 0, 15, 60, or 125 IU SC every other day or 7.5 g daily testosterone gel for 10 days (LOE 1). Testicular fluid was obtained by percutaneous aspiration for steroid measurements at baseline and after 10 days of treatment. The ITT concentrations increased in a dosedependent manner, with very low-dose hCG administration from 77 nmol/L to 923 nM in the 0 IU and 125 IU groups, respectively (P< .001). Moreover, serum hCG was statistically significantly correlated with both ITT and serum testosterone (P< .01). The investigators concluded that doses of hCG that were far lower than those used clinically (1,000–2,000 IU SC three times weekly) increased ITT concentrations in a dose-dependent manner in normal men with experimental gonadotropin deficiency. Recommendations Low-dose hCG with testosterone supplementation can maintain production of ITT and spermatogenesis (40). There are no fecundity data. The substantial cost and need for frequent hCG injections are significant barriers to the use of this combination, especially when alternative therapies are available (12). AROMATASE INHIBITORS (ANASTROZOLE AND LETROZOLE) Background Aromatase inhibitors (AIs) are FDA-approved for the treatment of early and late-stage breast cancer. They work by inhibiting the enzyme aromatase, which is involved estrogen synthesis and conversion. Regarding their off-label use in rejuvenation clinics, AIs are used by men who are on exogenous testosterone and AAS therapy to prevent the gynecomastia associated with increased estrogen levels. As a man's serum testosterone rises, a corresponding increase in the level of serum estrogen occurs from peripheral conversion via aromatase. From a fertility standpoint, AIs have been used to treat men with idiopathic male infertility, lower serum testosterone to estradiol ratios (<10), and hypogonadism related to obesity. Mechanism of Action Aromatase is a cytochrome P450 enzyme concentrated in the testes, liver, brain, and adipose tissue. It is responsible for the conversion of testosterone to estradiol (T/E2). Estradiol inhibits gonadotropin secretion and may exert direct effects on ITT production; AIs function by blocking the conversion of androgens to estrogens, consequently increasing serum levels of LH, FSH, and testosterone and resulting in functional effects similar to antiestrogens. The primary concern associated with aromatase inhibitors in men is that long-term estrogen deficiency may lead to osteopenia or osteoporosis and ultimately may have a negative effect on bone density. Clinical Evidence Raman et al. (41) reported on infertile men with T/E2 ratios (<10) treated with either testolactone or anastrozole. Men in both treatment groups showed significant improvements in their T/E2 ratios, sperm concentration, morphology, and motility. However, in a crossover study, Clark et al. (42) examined the effect of testolactone on oligozoospermic infertility. This study enrolled 25 men with idiopathic oligozoospermia who were administered testolactone (2 g/day) or placebo for 8 months. The two arms were then crossed and observed for an additional 8 months. This study failed to show any spermatogenic benefits or improved fertility. In the small subset of 25 infertile men receiving anastrozole for oligozoospermia, the sperm concentration increased significantly from 5.5 to 15.6 million per mL, and the total motile sperm concentration (TMSC) per ejaculate increased from 833 to 2,931 million (P< .005). No change was noted in the azoospermic cohort who were receiving anastrozole, and no pregnancies were reported for any of the men in the study, regardless of their semen parameter improvements. Letrozole, a nonsteroidal third-generation AI, was recently shown by Saylam et al. (43) to be effective in infertile men with low serum T/E2 ratios <10. Of the 10 men with oligospermia, the mean total motile sperm concentration significantly increased from 6.4 2.7 million to 15.7 5.01 million after treatment. The partners of two of the 10 oligospermic men (20%) achieved spontaneous pregnancy, and four of 17 azoospermic men (23.5%) were noted to have sperm in their ejaculate, with a mean total motile sperm concentration of 1.11 0.69 million. Recommendations Aromatase inhibitors have no demonstrated detrimental effect on spermatogenesis and can be used to help preserve fertility in hypogonadal men. However, based on the lack of long-term data, their use cannot be recommended for men who wish to preserve their fertility. CONCLUSION The use of hormones for rejuvenation is increasing with the aging of the Baby Boomer population. Men desiring children at a later age may be unaware of the side-effect profile of the hormones used at rejuvenation centers. Testosterone and AAS have well-established detrimental effects on spermatogenesis, although recovery may be possible with cessation. Clomiphene citrate, HGH/IGF-1, hCG, and AIs do not appear to have significant negative effects on sperm production, but quality data are lacking. REFERENCES 1. Fisch H, Braun S. The male biological clock: the startling news about aging and fertility in men. New York: Free Press; 2005. VOL. - NO. - / - 2013 6 REV 5.1.0 DTD FNS28165_proof 25 April 2013 5:24 am ce VW Fertility and Sterility® 2. 3. 4. 5. 6. 7. 8. 9. 10. 11. 12. 13. 14. 15. 16. 17. 18. 19. 20. 21. 22. Jaspen B. AMA report questions science behind using hormones as antiaging treatment. Chicago Tribune, June 15, 2009. Available at: http://arti cles.chicagotribune.com/2009-06-15/news/0906140132_1_anti-aging-hor mones-ama-council. Nigro N, Christ-Crain M. Testosterone treatment in the aging male: myth or reality? Swiss Med Wkly 2012;142:w13539. Mulligan T, Frick MF, Zuraw QC, Stemhagen A, McWhirter C. Prevalence of hypogonadism in males aged at least 45 years: the HIM study. Int J Clin Pract 2006;60:762–9. Ko EY, Siddiqi K, Brannigan RE, Sabanegh ES Jr. Empirical medical therapy for idiopathic male infertility: a survey of the American Urological Association. J Urol 2012;187:973–8. Zirkin BR, Santulli R, Awoniyi CA, Ewing LL. Maintenance of advanced spermatogenic cells in the adult rat testis: quantitative relationship to testosterone concentration within the testis. Endocrinology 1989;124:3043–9. McLachlan RI, O'Donnell L, Meachem SJ, et al. Hormonal regulation of spermatogenesis in primates and man: insights for development of the male hormonal contraceptive. J Androl 2002;23:149–62. Weinbauer GF, Nieschlag E. Gonadotrophin-releasing hormone analogueinduced manipulation of testicular function in the monkey. Hum Reprod 1993;8(Suppl 2):45–50. Liu PY, Swerdloff RS, Christenson PD, Handelsman DJ, Wang C, Hormonal Male Contraception Summit Group. Rate, extent, and modifiers of spermatogenic recovery after hormonal male contraception: an integrated analysis. Lancet 2006;367:1412–20. Contraceptiveefficacy of testosterone-induced azoospermia in normal men. World Health Organization Task Force on methods for the regulation of male fertility. Lancet 1990;336:955–9. Gu Y, Liang X, Wu W, Liu M, Song S, Cheng L, et al. Multicenter contraceptive efficacy trial of injectable testosterone undecanoate in Chinese men. J Clin Endocrinol Metab 2009;94:1910–5. Kim ED, Crosnoe L, Bar-Chama N, Khera M, Lipshultz LI. The treatment of hypogonadism in men of reproductive age. Fertil Steril 2013;99:718–24. Bhasin S, Storer TW, Berman N, Callegari C, Clevenger B, Phillips J, et al. The effects of supraphysiologic doses of testosterone on muscle size and strength in normal men. N Engl J Med 1996;335:1–7. Kanayama G, Brower KJ, Wood RI, Hudson JI, Pope HG Jr. Anabolicandrogenic steroid dependence: an emerging disorder. Addiction 2009;104:1966–78. Fronczak CM, Kim ED, Barqawi AB. The insults of illicit drug use on male fertility. J Androl 2012;33:515–28. BALCO scandal. Wikipedia, updated March 6, 2013. Available at: http: //en.wikipedia.org/wiki/BALCO_Scandal. Cohen J, Collins R, Darkes J, Gwartney D. A league of their own: demographics, motivations and patterns of use of 1,955 male adult non-medical anabolic steroid users in the United States. J Int Soc Sports Nutr 2007;4:12. Williams L. The steroid user next door—who bought and why. San Francisco Chronicle February 15, 2009. Available at: http://www.sfgate.com/health/ article/The-steroid-user-next-door-who-bought-and-why-3251047.php. Bonetti A, Tirelli F, Catapano A, Dazzi D, Dei Cas A, Solito F, et al. Side effects of anabolic androgenic steroids abuse. Int J Sports Med 2008;29:679–87. Fudala PJ, Weinrieb RM, Calarco JS, Kampman KM, Boardman C. An evaluation of anabolic-androgenic steroid abusers over a period of 1 year: seven case studies. Ann Clin Psychiatry 2003:121–30. Parkinson AB, Evans N. Anabolic androgenic steroids: a survey of 500 users. Med Sci Sports Exerc 2006;38:644–51. Pope HG Jr, Katz DL. Psychiatric and medical effects of anabolic-androgenic steroid use. A controlled study of 160 athletes. Arch Gen Psychiatry 1994; 51:375–82. 23. 24. 25. 26. 27. 28. 29. 30. 31. 32. 33. 34. 35. 36. 37. 38. 39. 40. 41. 42. 43. Wilson-Fearon C, Parrott AC. Multiple drug use and dietary restraint in a Mr. Universe competitor: psychobiological effects. Percept Mot Skills 1999;88: 578–80. Reyes-Fuentes A, Veldhuis JD. Neuroendocrine physiology of the normal male gonadal axis. Endocrinol Metab Clin North Am 1993;22:93–124. Menon DK. Successful treatment of anabolic steroid-induced azoospermia with human chorionic gonadotropin and human menopausal gonadotropin. Fertil Steril 2003;79(Suppl 3):1659–61. Schurmeyer T, Knuth UA, Belkien L, Nieschlag E. Reversible azoospermia induced by the anabolic steroid 19-nortestosterone. Lancet 1984;1:417–20. Turek PJ, Williams RH, Gilbaugh JH 3rd, Lipshultz LI. The reversibility of anabolic steroid-induced azoospermia. J Urol 1995;153:1628–30. Radicioni A, Paris E, Dondero F, Bonifacio V, Isidori A. Recombinant-growth hormone (rec-hGH) therapy in infertile men with idiopathic oligozoospermia. Acta Eur Fertil 1994;25:311–7. Bidlingmaier M, Strasburger CJ. Technology insight: detecting growth hormone abuse in athletes. Nat Clin Pract Endocrinol Metab 2007;3: 769–77. LA Health & Rejuvenation Hormone Therapy Centers. HGH injections & testosterone: what is hormone replacement therapy (HRT). Available at: www.lahealthandrejuvenation.com. Accessed April 11, 2013. Ovesen P, Jørgensen JO, Ingerslev J, Ho KK, Orskov H, Christiansen JS. Growth hormone treatment of subfertile males. Fertil Steril 1996;66:292–8. Shelly W, Draper MW, Krishnan V, Wong M, Jaffe RB. Selective estrogen receptor modulators: an update on recent clinical findings. Obstet Gynecol Surv 2008;63:163–81. Guay AT, Bansal S, Heatley GJ. Effect of raising endogenous testosterone levels in impotent men with secondary hypogonadism: double blind placebo-controlled trial with clomiphene citrate. J Clin Endocrinol Metab 1995;80:3546–52. Tan RS, Vasudevan D. Use of clomiphene citrate to reverse premature andropause secondary to steroid abuse. Fertil Steril 2003;79:203–5. Katz DJ, Nabulsi O, Tal R, Mulhall JP. Outcomes of clomiphene citrate treatment in young hypogonadal men. BJU Int 2012;110:573–8. U.S. Food and Drug Administration. Import Alert 66–71. Available at: http://www.accessdata.fda.gov/cms_ia/importalert_204.html/. Accessed December 1, 2012. Coviello AD, Matsumoto AM, Bremner WJ, Herbst KL, Amory JK, Anawalt BD, et al. Low-dose human chorionic gonadotropin maintains intratesticular testosterone in normal men with testosterone-induced gonadotropin suppression. J Clin Endocrinol Metab 2005;90:2595–602. Depenbusch M, von Eckardstein S, Simoni M, Nieschlag E. Maintenance of spermatogenesis in hypogonadotropic hypogonadal men with human chorionic gonadotropin alone. Eur J Endocrinol 2002;147:617–24. Roth MY, Page ST, Lin K, Anawalt BD, Matsumoto AM, Snyder CN, et al. Dose-dependent increase in intratesticular testosterone by very low-dose human chorionic gonadotropin in normal men with experimental gonadotropin deficiency. J Clin Endocrinol Metab 2010;95:3806–13. Hsieh TC, Pastuszak AW, Hwang K, Lipshultz LI. Concomitant intramuscular human chorionic gonadotropin preserves spermatogenesis in men undergoing testosterone replacement therapy. J Urol 2013;189:647–50. Raman JD, Schlegel PN. Aromatase inhibitors for male infertility. J Urol 2002; 167:624–9. Clark RV, Sherins RJ. Treatment of men with idiopathic oligozoospermic infertility using the aromatase inhibitor, testolactone: results of a doubleblinded, randomized, placebo-controlled trial with crossover. J Androl 1989;10:240–7. Saylam B, Efesoy O, Cayan S. The effect of aromatase inhibitor letrozole on body mass index, serum hormones, and sperm parameters in infertile men. Fertil Steril 2011;95:809–11. VOL. - NO. - / - 2013 7 REV 5.1.0 DTD FNS28165_proof 25 April 2013 5:24 am ce VW VIEWS AND REVIEWS 1 Effect of rejuvenation hormones on spermatogenesis J. L. Moss, L. E. Crosnoe, and E. D. Kim Knoxville, Tennessee Testosterone and anabolic androgenic steroids suppress spermatogenesis. Clomiphene citrate, HGH/IGF-1, hCG, and aromatase inhibitors offer a protective effect for spermatogenesis, with either a neutral or positive overall effect. VOL. - NO. - / - 2013 REV 5.1.0 DTD FNS28165_proof 25 April 2013 5:24 am ce VW