Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Child psychopathology wikipedia , lookup
Combat stress reaction wikipedia , lookup
Mental disorder wikipedia , lookup
Drug rehabilitation wikipedia , lookup
Factitious disorder imposed on another wikipedia , lookup
Biology of depression wikipedia , lookup
Major depressive disorder wikipedia , lookup
Munchausen by Internet wikipedia , lookup
Behavioral theories of depression wikipedia , lookup
History of mental disorders wikipedia , lookup
Diagnostic and Statistical Manual of Mental Disorders wikipedia , lookup
Emil Kraepelin wikipedia , lookup
Causes of mental disorders wikipedia , lookup
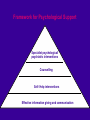
PSYCHOLOGICAL MEDICINE Dr Eugene M Cassidy MD, MRCPsych, MMedSc (Physiol.) Consultant Liaison Psychiatrist CUH [email protected] CUH Liaison Psychiatry Outline • • • • • • Mental Health Problems in General Hospital - Overview Psychological Adjustment to illness Depression in Medical Illness Alcohol Problems Somatisation Management CUH Liaison Psychiatry Mental Health in the General Hospital • Deliberate self-harm • Drug and alcohol misuse • Acute organic disorders (delirium) • Psychological adjustment to illness • Physical and psychiatric co-morbidity • Medically unexplained symptoms • Behavioural problems (e.g. non-adherence to treatment, capacity issues) CUH Liaison Psychiatry Psychological adjustment to illness CUH Liaison Psychiatry Stress and Physical illness • Major health problems are stressful • Response to this stress dependent upon individual – Perception / Beliefs of illness – Vulnerability – Coping ability – Response of others CUH Liaison Psychiatry Illness Perception / Beliefs • • • • • Illness identity Cause Consequences Course Cure/controllability • Influenced by – Medical Communication, Personal experience, Norms CUH Liaison Psychiatry Individual Vulnerability • Personality traits (e.g. tendency to worry about illness) • Prior experience of illness within a family • An individual’s psychological state at the time of the illness • Previous experience of trauma, or a neglected or abusive childhood CUH Liaison Psychiatry Helpful Coping • • • • • • Seeking information Seeking practical and social support Learning new skills Developing new interests Helping others Emotion-focused coping CUH Liaison Psychiatry Less Helpful Coping • • • • Hoping the condition will just disappear Denial Obsessively focusing on minute details of the disorder Seeking others to blame CUH Liaison Psychiatry Response of Others to illness • • • • Closing in Drifting away Infantilising Depersonalising • Guthrie CUH Liaison Psychiatry Physical and Psychiatric Co-morbidity CUH Liaison Psychiatry Psychological Medicine • Applies bio-psychosocial model to medical care (irrespective of psychiatric morbidity) • Involves all staff and all patients • More than just Liaison Psychiatry & Health Psychology • Is there a need? – Psychiatric disorders in medical illness – Benefits most obvious in Somatoform disorder CUH Liaison Psychiatry Depression in Medical Illness • Vulnerability – Stress model • Bio-psycho-social • Dimensional (significant depressive symptoms) • Categorical (Major Depression) CUH Liaison Psychiatry Depression is common in medical illness • Major Depressive disorder 8% • All depressive disorders 15-36% Magni et al, 1986, Feldman et al, 1987, Koenig et al, 1997, Von Ammon et al, 2001 CUH Liaison Psychiatry Depression is under recognised • Physicians have been found to recognise depression in only one fourth to one half of their depressed medical outpatients Wells et al, 1989; Schulberg et al, 1985; RCP/RCPsych, 1995 CUH Liaison Psychiatry Detection of Depression in Medical Setting • Be vigilant – Depression is common • Ask about it: • If positive, look for: – mood and motivation symptoms – cognitive changes (always enquire about suicidal thoughts) – biological symptoms – Disability or physical symptoms in xs of expected CUH Liaison Psychiatry Screening for Major Depression Please ask the following: 1. During the past month have you been bothered by feeling down, depressed or hopeless? No Yes 2. During the past month have you been bothered by little interest or pleasure in doing things? No Yes If Yes to either of the above 2 questions, please ask: 3. Is this something with which you would like help? No Yes, but not today Yes Likelihood Ratio for MDD = 17.5 (ST elevation in MI 11.2; D-Dimers>1092ng/ml 3.1) Depression affects medical outcome • Morbidity • Survival • Length of hospital stay • Cost of medical care • Compliance with therapy, • Quality of life Creed et al, 2002; Katon et al, 2003 CUH Liaison Psychiatry Frasure-Smith et al, 1993 CUH Liaison Psychiatry Lesperance et al, 2002 CUH Liaison Psychiatry Impact of depression on DM • • • • More complications Poorer glycemic control Reduced dietary / oral hypoglycemic adherance More typical DM symptoms even when severity of DM controlled for • Poorer quality of life • Increased healthcare costs x 4.5 (Egede et al, 2002) CUH Liaison Psychiatry Depression is treatable ….. But it isn’t always treated • Beware empathy and understanding • Antidepressants • Psychological therapies CUH Liaison Psychiatry CUH Liaison Psychiatry Gill & Hatcher, 2000 CUH Liaison Psychiatry The Burden of Alcohol Misuse on emergency inpatient hospital admissions among residents from a health board region in Ireland O’Farrell, S. Allwright, J. Downey, D Bedford, F. Howell. Addiction (2004): 99, 1279-1285 Acute Alcohol intoxication • 2.0% all emergency admissions • 203/100,000 population CUH Liaison Psychiatry PREVALENCE 147/759 (19.4%) CAGE + 19% DSM-IV Abuse / Dependence • 30% male • 8% female DETECTION 80% doctors enquire 46% record consumption 1% recorded CAGE 18% recognised by medic •64% discharge summaries •37% referred on CUH Liaison Psychiatry PHARMACOTHERAPY OF WITHDRAWAL Pharmacological Management of Alcohol Withdrawal: Evidence-based practice guideline Mayo-Smith et al, JAMA, 1997 Benzodiazepines •Reduce symptoms •Prevent seizures •Prevent delirium CUH Liaison Psychiatry Fixed Dose or Symptom Triggered Withdrawal Scales Thiamine for Wernicke-Korsakoff Syndrome in people at risk from alcohol abuse Day E, Bentham P, Callaghan R, Kuruvilla T, George S Cochrane Review (2004) + CUH Liaison Psychiatry A Good place to Intervene 60 50 40 gen hosp gen populn. 30 20 10 0 pre-cont action CUH Liaison Psychiatry Rumpf et al, 1987 Feedback Helps! • Health Consequences Feedback increases the proportion of patients willing to accept brief advice by @¼ R Patton, MJ Crawford, R Touquet. Emerg Med J (2003)20: 451-452 CUH Liaison Psychiatry “With respect to alcohol abuse, our charge is straightforward: first we must ask something, then we must do something.” CUH Liaison Psychiatry Somatisation • See other PPT PRESENTATION as part of this lecture series CUH Liaison Psychiatry Management of Mental Health Problems in Medical Illness CUH Liaison Psychiatry Framework for Psychological Support Specialist psychological/ psychiatric interventions Counselling Self- Help interventions Effective information giving and communication Stepped care approach (1) • Prevention • Information and Communication • Involve and Support families / carers CUH Liaison Psychiatry Stepped care approach (2) • • • • Simple advice and problem-solving Self-help Relaxation techniques Counselling – problem focussed CUH Liaison Psychiatry Stepped care approach (3) • Drug treatments – Drug interactions – Benefits in co-morbid illness symptomatology • Specific psychological therapies – CBT – Marital therapy – Family therapy CUH Liaison Psychiatry Biopsychosocial Management INTERESTED IN A CAREER IN PSYCHIATRY ??? • Please contact me at : [email protected] • Tel: 021-4920007 CUH Liaison Psychiatry







































![HFN2_GP_presentation_2012_septFinal [Compatibility Mode]](http://s1.studyres.com/store/data/001774704_1-8552a80a3327859a3984e095598400da-150x150.png)