Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
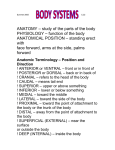
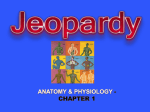
Journal of Biomechanics 36 (2003) 731–736 Modeling the relation between cardiac pump function and myofiber mechanics T. Artsa,b,*, P. Bovendeerdb, T. Delhaasc, F. Prinzenc a Faculty of Biomedical Engineering, Eindhoven University of Technology, Eindhoven, The Netherlands b Departments of Biophysics, Maastricht University, Maastricht 6200 MD, The Netherlands c Department of physiology, Maastricht University, Maastricht 6200 MD, The Netherlands Accepted 25 November 2002 Abstract Complexity of the geometry and structure of the heart hampers easy modeling of cardiac mechanics. The modeling can however be simplified considerably when using the hypothesis that in the normal heart myofiber structure and geometry adapt, until load is evenly distributed. A simple and realistic relationship is found between the hemodynamic variables cavity pressure and volume, and myofiber load parameters stress and strain. The most important geometric parameter in the latter relation is the ratio of cavity volume to wall volume, while actual geometry appears practically irrelevant. Applying the found relationship, a realistic maximum is set to left ventricular pressure after chronic pressure load. Pressures exceeding this level are likely to cause decompensation and heart failure. Furthermore, model is presented to simulate left and right ventricular pump function with left–right interaction. r 2003 Elsevier Science Ltd. All rights reserved. 1. Introduction The heart consists of four cavities. For each cavity, the work generated by the myofibers in the wall is converted to pump work. Wall mass is about proportional with generated contractile work. Pump work is closely related to the product of stroke volume and generated systolic pressure. Consequently, the left ventricle is the cavity with the largest wall mass, followed by the right ventricle, the left atrium and the right atrium, respectively. Pump function of a cavity can be characterized by the time-variant relation between cavity pressure pcav and cavity volume Vcav during the cardiac cycle. Plotting pressure as a function of volume, a pV-diagram is obtained with the shape of a loop. The area of the loop represents stroke work. The shape and position of the loop in the pV-diagram is characteristic for the quality of pump function. According to the variable elastance model (Sagawa, 1978) pressure may be modeled as a *Corresponding author. Department of Biophysics, Maastricht University, PO Box 616, 6200 MD Maastricht, The Netherlands, Tel.: +31-43-3881656. E-mail address: [email protected] (T. Arts). time-variant compliance. During activation, the cavity stiffens considerably, forcing the cavity to a low volume. In a closer look, active cavity pressure also appeared to depend on the time derivative of cavity volume (Suga and Yamakoshi, 1977), implying an inherent timedependent viscous behavior. Pump work is generated by the summed action of all separate cardiomyocytes, arranged in a specific structure of myofiber orientations (Streeter, 1979). Local myofiber work is quantified by stress and strain as a function of time. In experiments on isolated myofibers, under a variety of circumstances myofiber force has been described as a function of sarcomere length, velocity of sarcomere shortening and time (De Tombe and Ter Keurs, 1990; Guccione et al., 1997). In the literature, stress, force and cavity pressure are closely related subjects. Similarly, myofiber strain is closely related to changes in sarcomere length and cavity volume. Myofiber stress sf is a function of sarcomere length ls and time. This stress is a summation of a passive elastic component (spas ) and an active component (sact ). The active component is modeled by a contractile element with length lce in series with a series elastic element. The velocity of contractile element shortening dlce/dt is a 0021-9290/03/$ - see front matter r 2003 Elsevier Science Ltd. All rights reserved. doi:10.1016/S0021-9290(02)00451-7 732 T. Arts et al. / Journal of Biomechanics 36 (2003) 731–736 function of time (t) and active stress (sact ) (Hill, 1939). The following model may be used: 2. Three-dimensional models of cardiac mechanics sf ¼ spas ðls Þ þ sact ðls ; lce ; tÞ dlce ¼ functionðsact ðls ; lce ; tÞ; tÞ: dt To investigate the relation between left ventricular pump function and local, time-variant myofiber mechanics, a finite element model of left ventricular mechanics was developed (Bovendeerd et al., 1992). The reference shape of the wall was taken to be rotationally symmetric, having a realistic wall thickness. The angulation of myofiber orientation with the circumferential direction was taken from Streeter (Streeter, 1979). When simulating normal cardiac mechanics, the distribution of systolic myofiber stress appeared very sensitive to the chosen distribution of myofiber orientation. Within the range of accuracy of the myofiber orientation measurements, systolic myofiber stress could vary locally by a factor of two (Bovendeerd et al., 1992). In designing a realistic model, the needed accuracy for local myofiber orientation appeared much higher than measurements could provide. The transmural gradient in myofiber orientation is about 201/mm in humans. So an error in the location by 0.25 mm causes already a significant error in the stress calculation. Spatial inaccuracies due to biological variance are likely to be much higher. Lack of accuracy forced us to give up using in vivo measurements on myofiber orientation for the purpose of stress calculation. In stead we used the hypothesis that in the normal heart, myofiber orientation adapts locally so that myofiber stress and strain are about uniform. This hypothesis was investigated in a model, using a rotationally symmetric ventricle. Local wall thickness and local myofiber orientation were optimized to reach a minimum value for the standard deviation of strain within the wall (Rijcken et al., 1999). The thus found distribution of myofiber orientation inside the wall was not significantly different from reported measurements. Thus it was concluded that the use of calculated myofiber orientation should be preferred over measured values. Interestingly, stress was transmitted predominantly along the direction of maximum stiffness. In systole, and also in diastole be it to a lesser degree, this direction practically coincided with the myofiber direction. We therefore designed the one-fiber model by simplifying the complex threedimensional material behavior of the tissue to a model with uniform uniaxial stress. ð1Þ Quantification of the relation between pump variables like pressure and volume to myofiber variables like stress and strain has been subject of discussion for a long time. For a given systolic pressure and stroke volume it has been shown that metabolism is not uniquely determined. At constant stroke work, oxygen consumption increases with end-diastolic volume (Suga et al., 1987). Apparently, the starting conditions of a contraction cycle are important to mechanics and metabolism. To further elucidate the relation between myofiber mechanics and pump function, numerical models of cardiac mechanics have been designed (Vetter and McCulloch, 2000; Bovendeerd et al., 1996). Currently for many applications, sufficient information is available to establish this relation. Myocardial material has to be considered anisotropic (Arts et al., 1979; Hunter et al., 1998). Passive myocardial material properties are known from biaxial loading experiments (Humphrey et al., 1990) on the excised septum. Active myofiber mechanics is known from experiments on isolated myofibers (De Tombe and Ter Keurs, 1990; Guccione et al., 1997; Hunter et al., 1998). Cardiac geometry can be measured directly by for instance magnetic resonance imaging (MRI) or post mortem anatomical measurements. Regional myofiber orientation and collagen lamina organization may be obtained from anatomical measurements (Streeter, 1979; LeGrice et al., 1995; Costa et al., 1999; Arts et al., 2001; Bovendeerd et al., 1999). In the present study, we have investigated what properties are crucial in relating pump function to myofiber dynamics, and what properties may be less relevant under what circumstances. Efficiency in modeling requires customizing the model design. Recent models of cardiac mechanics most often use finite element analysis (Vetter and McCulloch, 2000; Bovendeerd et al., 1996). The strong point of these models is the ability to deal with non-uniformities in material properties within the heart, occurring for instance in the paced or in the infarcted heart. From these models, in the normal heart properties as well as load appeared to be quite uniform, especially during systole. In the present study a tremendous simplification was applied by leaving out spatial variations in modeling the relation between tissue mechanics and pump function in the normal heart. The resulting one-fiber model of cardiac mechanics relates cavity pressure and volume to myofiber stress and strain. Finally, applications of this model are shown, concerning 1) adaptation possibilities and limitations to pressure load, and 2) left and right ventricular mechanics with their mutual interaction. 3. The one-fiber model of cardiac mechanics Having myofiber orientation optimized for reaching uniform stress and strain in the wall, myofiber dynamics in the normal heart simplifies considerably. In absence of spatial differences, mean values are good estimates of local shortening and stress. Following earlier ideas on the cardiac myofiber structure (Torrent-Guasp, 1959, T. Arts et al. / Journal of Biomechanics 36 (2003) 731–736 Fig. 1. The wall of a myocardial cavity may be considered as a single long thin fiber, wrapped around the cavity. Suppose the fiber starts at midwall equator. After following the circular circumferential pathway, the fiber end just slightly displaces to a toroidal layer, enclosing the starting pathway. Following a helical pathway in the toroidal layer, this layer can be filled completely. Similarly a next toroidal layer is filled, until the outer toroidal layer, encompassing the epicardium and endocardium, is filled completely. Thus a whole ventricular wall, having a realistic distribution of fiber orientations, has been filled with one single fiber. Streeter, 1979, p. 856) we consider the cavity to be wrapped in one single long fiber, filling the whole wall (Fig. 1), comparable to a rope wrapped on a core, representing the cavity. Since mechanical load is transmitted predominantly along the myofibers, the myocardial tissue was described by a fluid fiber model, in which total Cauchy stress stotal is composed of a hydrostatic pressure pwall and fiber stress sf : stotal ¼ pwall I þ sf ef ef ; ð2Þ where ef represents fiber direction. Assuming the myofibers to be parallel with the wall surface (ef;r ¼ 0), using Eq. (2) for myofiber stress sf it is found: sf ¼ scc þ szz 2srr : ð3Þ The indices c, z and r refer to the circumferential, base to apex and transmural direction. The variables scc ; szz and srr are components of the stress tensor stotal : In many model studies of left ventricular wall mechanics, stress in the wall is estimated as a function of cavity pressure and various geometric parameters. In performing simulations with many of these models, often having various wall geometries, fiber structures, and material properties, the following general relation between myofiber stress sf and cavity pressure pcav has been found having an accuracy as good as 75% (Arts et al., 1991): sf Vcav E1 þ 3 : ð4Þ pcav Vwall Eq. (4) shows that for a given pressure wall stress increases with cavity volume, which is consistent with common models on wall stress. In relating cavity 733 pressure to myofiber stress, the ratio of cavity volume to wall volume appears by far the most important geometric parameter. The actual shape of the wall appeared of minor importance (Arts et al., 1991). In an extended trial, the definition of sf according to Eq. (3) was also applied to models having isotropic wall material. Unexpectedly, under these conditions, Eq. (4) appeared to be valid too. So, using Eq. (3) as a definition of stress, the validity range of the one-fiber model can be extended to the passive, more isotropic wall material properties as well. Having this simple relationship of Eq. (4), the very robust physical law of conservation of work was applied to derive a relation for myofiber strain ef : Using that incremental pump work is equal to incremental mechanical work generated by the myofibers, it follows: def pcav ¼ : pcav dVcav ¼ Vwall sf def dVcav =Vwall sf ð5Þ Note that sf def represents incremental mechanical myofiber work per unit of tissue volume. Substituting Eq. (4) into Eq. (5), followed by integration with respect to normalized cavity volume Vcav /Vwall ; the following expression was found for the change Def in fiber strain when cavity volume changes from Vcav1 to Vcav2 : 1 1 þ 3Vcav2 =Vwall Def ¼ ln : ð6Þ 3 1 þ 3Vcav1 =Vwall Note that myofiber strain ef is a natural strain, linked to sarcomere length li by: ls ef ¼ ln : ð7Þ ls;ref Parameter ls;ref refers to a reference sarcomere length. This length becomes irrelevant when considering strain between two states like it occurs in Eq. (6). Inversion of Eq. (6) provides expressions for cavity volume Vcav as a function of myofiber strain ef : Vcav 1 Vcav;ref 3ðef ef;ref Þ 1þ3 ¼ 1 : ð8Þ e Vwall 3 Vwall Eq. (8) requires knowledge of Vwall and Vcav;ref at some reference state, which may be used as the zero reference of ef : In Fig. 2 at known wall volume, for a given time course of cavity volume, myofiber strain was calculated using Eq. (6). For a given time course of left ventricular pressure, using the cavity volume data, myofiber stress was calculated using Eq. (4). Myofiber stress was thus determined as a function of myofiber strain by using measurements that can be performed non-invasively in the clinic. During ejection the level of left ventricular pressure is relatively constant, causing the pressure volume loop to be about symmetric. In contrast, at the beginning of ejection, fiber stress is considerably higher than at the 734 T. Arts et al. / Journal of Biomechanics 36 (2003) 731–736 about the stress-strain relation of myofibers are obtained only in experiments on isolated myofibers. 4. Adaptation of cavity and wall volume to load The circulation requires a given amount of stroke volume Vstroke at a given amount of stroke work Estroke : We define ejection pressure peject by: Estroke peject ¼ : ð9Þ Vstroke Fig. 2. Simulation of left ventricular cavity mechanics during a cardiac cycle. The left panel shows the myofiber parameters fiber strain ef and myofiber stress sf ; and the pump parameters cavity volume Vlv and cavity pressure plv ; as a function of time. Cavity volume is normalized to wall volume Vwall : In the right panel the high narrow loop shows myofiber stress as a function of myofiber strain. The area of the sf 2Def loop represents myofiber stroke work per unit of tissue volume. Similarly, the wide low curve represents the plv 2Vlv loop. The area of the loop represents pump stroke work, normalized to wall volume. Note: Both loops have the same physical dimension along their axes and the same area, showing that pump work is equal to the mechanical work as generated by the tissue. end of ejection, causing the stress–strain loop to be clearly asymmetric. The presented model provides an instantaneous relation between cardiac pump function parameters and myofiber function parameters. Despite its simplicity, realistic time dependent myofiber stress results in realistic time courses of left ventricular pressure (Fig. 2). For instance an isometric myofiber stress of 120 kPa in an end-diastolic left ventricle with a cavity to wall volume ratio of 0.6 results in an isovolumic pressure of 43 kPa (=300 mmHg), which is a very realistic value for a healthy, intact left ventricle (Arts et al., 1982). A thorough test of the model under many circumstances was considered beyond the scope of this article. Eqs. (4)–(8) form the backbone of the one-fiber model. In models it is often convenient to express pressure as a function of volume, applying the constitutive behavior of the myofibers. Then sarcomere length ls can be calculated from volume by Eqs. (8) and (7). Stress sf is calculated from ls through the constitutive equations of the myocardial material. Finally, Eq. (4) is used to calculate cavity pressure. In another application, shown in relation to Fig. (2), from in vivo measured time courses of left ventricular volume and pressure, the stress–strain relation of the myocardial tissue can be estimated as a function of time during the cardiac cycle (Schreuder et al., 2000). Thus in patients the constitutive behavior of the myofiber may be obtained from non-invasive or moderately invasive hemodynamic measurements. Currently, information The variable peject represents afterload. Normally, healthy cardiac tissue adapts mass and myofiber direction such that regular mechanical load reaches a given, biologically determined level. Normal load levels of myocardial tissue may be characterized by mechanical stroke work per unit of tissue volume wstroke and myofiber strain Def during ejection. Wall volume after adaptation is proportional to stroke work Estroke peject Vstroke Vwall ¼ ¼ : ð10Þ wstroke wstroke Using Eq. (6), substituting for cavity volumes Vcav1 and Vcav2 the volumes at the beginning (Vbe ) and end of ejection (Vee ), while applying Vbe ¼ Vee þ Vstroke and Eq. (10), it is found: Vstroke Vwall 1 peject ¼ Vstroke 3De Vee ¼ 3De : e f 1 3wstroke e f 1 3 ð11Þ According to Eqs. (11) after complete adaptation to load, ventricular cavity and wall volume are determined by the tissue properties of adaptation, wstroke and Def ; and required afterload peject and stroke volume Vstroke : We found the following tissue parameter values to be reasonable: wstroke E6000 Jm3 and Def E0:16: Note that the physical dimension of wstroke is the same as that of pressure, i.e. [Pa]=[N m2]=[J m3]. 4.1. Maximum pressure load Interestingly, in adapting geometry to pressure load using Eq. (11), an upper limit is set to systolic pressure peject ; because end-systolic cavity volume has to be positive. The latter condition is equivalent to: ejection fraction o100%. Using Eqs. (11) it is found: 3wstroke peject opeject;max ¼ 3De : ð12Þ e f 1 For the abovementioned normal values of wstroke and Def ; maximum pressure with full adaptive compensation appears peject;max ¼ 29:2 kPa (E218 mmHg). Normally, left ventricular pressure during ejection is readily below this upper limit. However, the pressure safety margin may decrease considerably by: (1) increase of afterload, caused by aortic stenosis or by stiffening of the blood T. Arts et al. / Journal of Biomechanics 36 (2003) 731–736 735 Table 1 Predicted wall and cavity volumes Cavity a Left ventricle Right ventriclea Outer wall Inner wall Left ventricleb Right ventricleb Peject (kPa) Vstroke (ml) Vwall (ml) Vcav;be (ml) Vcav;ee (ml) 15 3.75 3.75 11.25 15 3.75 80 80 160 80 80 80 200 50 100 150 143 193 386 160 147 117 63 113 226 80 67 37 Stroke work per tissue volume: wstroke ¼ 6000 N m2 : Systolic myofiber shortening: Def ¼ 0:16: a Separate ventricular walls. b Overlapping ventricular walls, overlap volume: Voverlap ¼ 40 ml: vessels due to aging, or (2) deterioration of myocardial tissue performance, to be expressed by a decreased value of wstroke : Qualitatively as well as quantitatively, the latter conditions are in remarkable agreement with known clinical risks of heart failure. Limitation of afterload by reducing load pressure and/or limiting systolic myofiber shortening by for instance negative inotropic drugs, vasodilators or b-blockade may also help to increase the pressure safety margin. The maximum pressure set by Eq. (12) is likely to be an overestimation, because maximum ejection fraction is always less than the assumed 100%. 4.2. Left and right ventricular wall volume and cavity size Knowing pressure load peject during ejection and stroke volume Vstroke ; wall volume and begin- and endsystolic cavity volumes can be predicted by using Eqs. (11). For the left and right ventricle, stroke volume is about 80 ml for both, and systolic pressure load is about 15 and 3.75 kPa, respectively. In the upper two lines of Table 1, the thus calculated values for wall volume, and cavity volume at the beginning and end of ejection are shown. In modeling the left and right ventricle one may consider a different set up (Fig. 3, middle panel) (Arts and Reneman, 1988). A common outer wall, having a transmural pressure equal to right ventricular pressure, and a stroke volume of the two cavities together, encapsulates the right and left ventricular cavities. The inner wall encapsulates the left ventricular cavity only, having a transmural pressure equal to the difference between left and right ventricular pressure, and a stroke volume of one cavity only. Using Eqs. (10)–(11) inner and outer wall volumes and cavity volumes are calculated (Table 1). In this composite, even at the end of ejection, the inner side of the outer shell is slightly wider than the outer side of the inner shell. To free some extra space for the right cavity, the shells are assembled slightly asymmetrically (Fig. 3, right panel). As a result, the outer and inner wall partially overlap inside the free wall of the left ventricle. The left ventricular free wall appears somewhat thicker than the septum. From a realistic Fig. 3, the overlap volume is estimated to be about a fraction of 0.4 of the outer wall. The left ventricular cavity is estimated to be smaller by about one third of the overlap volume due to the increase of free wall thickness. The thus found composite appears very realistic. Representing the heart (Fig. 3) by an outer wall (index o), encapsulating the related cavity, the inner wall and cavity (index i), inner and outer cavity volumes, Vcav;i and Vcav;o ; are determined from left and right ventricular cavity volumes, Vlv and Vrv ; by: 1 Vcav;i ¼ Vlv Voverlap ; 3 Vcav;o ¼ Vlv þ Vrv þ ðVwall;i Voverlap Þ: Fig. 3. Composing left (LV) and right (RV) ventricle to a heart in endsystole. Left panel: Separate left and right ventricular walls. Middle panel: In a more realistic configuration an outer wall (o) encapsulates an inner (i) wall. Right panel: The inner wall encapsulates the LV only. Overlap of the outer wall with the inner wall enlarges the RV cavity. The crosshatched area represents the extra volume of the LV free wall due to this overlap. ð13Þ The volume Voverlap is considered a constant, representing the overlap of the inner wall and outer wall in the composite of left and right ventricle. Eq. (10) is used to estimate outer and inner wall volume from the related ejection pressures and stroke volumes. Next, Eq. (6) is used to express inner and outer shell myofiber strain (Def;i and Def;o ; respectively) as a function of inner and outer cavity (Vcav;i and Vcav;o ; respectively) and wall T. Arts et al. / Journal of Biomechanics 36 (2003) 731–736 736 (Vwall;i and Vwall;o ; respectively) volume: 1 1 þ 3Vcav;i;be =Vwall;i Def;i ¼ ln and 3 1 þ 3Vcav;i =Vwall;i 1 1 þ 3Vcav;o;be =Vwall;o : Def;o ¼ ln 3 1 þ 3Vcav;o =Vwall;o ð14Þ Begin of ejection (be) has been used as strain reference state. Myofiber stresses are determined from myofiber strains, using the constitutive equations of myofibers (Eq. (1)). From these stresses, applying Eq. (4), pressures in the inner and outer cavities are calculated. Finally, these pressures are converted to left and right cavity pressures by plv ¼ pcav;i þ pcav;o and prv ¼ pcav;o : ð15Þ Thus, a model of the composite of right and left ventricle is designed, estimating cavity pressures as a function of cavity volumes, and presenting left right interaction. For example, imagine the presence of a pulmonary artery hypertension. Then the elevated pressure in the right ventricular cavity is added to this pressure in the left ventricular cavity (Eq. (15)), thus influencing both filling and ejection. 5. Summary For the non-uniform heart, a three-dimensional finite element model is needed to relate the hemodynamic parameters cavity pressure and volume to the local myocardial parameters myofiber strain and myofiber stress. In the normal heart, we use the hypothesis that myofiber structure and geometry adapt so that the myofiber shortening and tissue workload are constant. Using this hypothesis: (1) a realistic relationship is found between myofiber mechanics and hemodynamic parameters, (2) the ratio of cavity volume to wall volume is the most important geometric parameter relating cavity pressure and volume to myofiber stress and strain, (3) a realistic maximum is set to chronic systolic pressure load, and (4) left and right ventricular interaction can be simulated. References Arts, T., Reneman, R.S., 1988. The importance of the geometry of the heart to the pump. In: ter Keurs, H., Noble, M. (Eds.), Starling’s Law of the Heart Revisited. Kluwer Acad Publishers, Dordrecht, pp. 94–111. Arts, T., Veenstra, P.C., Reneman, R.S., 1979. A model of the mechanics of the left ventricle. Annals of Biomedical Engineering 7, 299–318. Arts, T., Veenstra, P.C., Reneman, R.S., 1982. Epicardial deformation and left ventricular wall mechanics during ejection in the dog. American Journal of Physiology 243, H379–H390. Arts, T., Bovendeerd, P.H.M., Prinzen, F.W., Reneman, R.S., 1991. Relation between left ventricular cavity pressure and volume and systolic fiber stress and strain in the wall. Biophyscial Journal 59, 93–103. Arts, T., Costa, K.D., Covell, J.W., McCulloch, A.D., 2001. Relating myocardial laminar architecture to shear strain and muscle fiber orientation. American Journal of Physiology 280, H2222–H2229. Bovendeerd, P.H.M., Arts, T., Delhaas, T., Huyghe, J.M., Van Campen, D.H., Reneman, R.S., 1996. Regional wall mechanics in the ischemic left ventricle: numerical models and dog experiments. American Journal of Physiology 270, H398–H410. Bovendeerd, P.H.M., Arts, T., Huyghe, J.M., Van Campen, D.H., Reneman, R.S., 1992. Dependence of left ventricular wall mechanics on myocardial fiber orientation: a model study. Journal of Biomechanics 25, 1129–1140. Bovendeerd, P.H.M., Rijcken, J., Van Campen, D.H., Schoofs, A.J.G., Nicolay, K., Arts, T., 1999. Optimization of left ventricular muscle fiber orientation. In: Pederson, M.P.B.P. (Ed.), IUTAM Symposium on Synthesis in Bio Solid Mechanics. Kluwer Academic Publishers, Netherlands, pp. 285–296. Costa, K.D., Takayama, Y., McCulloch, A.D., Covell, J.W., 1999. Laminar fiber architecture and three-dimensional systolic mechanics in canine ventricular myocardium. American Journal of Physiology. 276, H595–607. De Tombe, P.P., Ter Keurs, H.E.D.J., 1990. Force and velocity of sarcomere shortening in trabeculae from rat heart. Circulation Research 66, 1239–1254. Guccione, J.M., Le Prell, G.S., de Tombe, P.P., Hunter, W.C., 1997. Measurements of active myocardial tension under a wide range of physiological loading conditions. Journal Biomechanics 30, 189–192. Hill, A.V., 1939. The transformation of energy and mechanical work of muscles. Proceedings of Physiological Society 51, 1–18. Humphrey, J.D., Strumpf, R.K., Yin, F.C.P., 1990. Biaxial mechanical behavior of excised ventricular epicardium. American Journal of Physiology 259, H101–H108. Hunter, P.J., McCulloch, A.D., ter Keurs, H.E., 1998. Modelling the mechanical properties of cardiac muscle. Progression Biophysics Molecular Biology 69, 289–331. LeGrice, I.J., Takayama, Y., Covell, J.W., 1995. Transverse shear along myocardial cleavage planes provides a mechanism for normal systolic wall thickening. Circulation Research 77, 182–193. Rijcken, J., Bovendeerd, P.H.M., Schoofs, A.J.G., van Campen, D.H., Arts, T., 1999. Optimization of cardiac fiber orientation for homogeneous fiber strain during ejection. Annals of Biomedical Engineering 27, 289–297. Sagawa, K., 1978. The ventricular pressure volume diagram revisited. Circ Research 43, 677–687. Schreuder, J.J., Steendijk, P., van der Veen, F.H., Alfieri, O., van der Nagel, T., Lorusso, R., van Dantzig, J.M., Prenger, K.B., Baan, J., Wellens, H.J., Batista, R.J., 2000. Acute and short-term effects of partial left ventriculectomy in dilated cardiomyopathy: assessment by pressure–volume loops. Journal of the American College of Cardiololgy 36, 2104–2114. Streeter, D.D., 1979. Gross morphology and fiber geometry of the heart. In: Berne, R.M. (Ed.), The Cardiovascular System, The Heart. American Physiological Society, Bethesda, Maryland, USA, pp. 61–112. Suga, H., Yamakoshi, K.I., 1977. Effect of stroke volume and velocity of ejection on end-systolic pressure of canine left ventricle. Circulation Research 40, 445–450. Suga, H., Yasumara, Y., Nozawa, T., Futaki, S., Igarashi, Y., Goto, Y., 1987. Prospective prediction of O2 consumption from pressurevolume area in dog hearts. American Journal of Physiology 252, H1258–H1264. Torrent-Guasp, F., 1959. An Experimental Approach on Heart Dynamics. Aguirre Torre, Madrid. Vetter, F.J., McCulloch, A.D., 2000. Three-dimensional stress and strain in passive rabbit left ventricle: a model study. Annals of Biomedical Engineering 28, 781–792.