Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
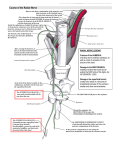
RAJIV GANDHI UNIVERSITY OF HEALTH SCIENCES, KARNATAKA, BANGALORE. ANNEXURE-II PROFORMA FOR REGISTRATION OF SUBJECTS FOR DISSERTATION TO BE SUBMITTED IN DUPLICATE 1. NAME OF THE DR. DIVYA.C CANDIDATE AND D/0 P V CHANDRASHEKAR REDDY, ADDRESS # 251, 3RD FLOOR, 13TH CROSS, 11TH MAIN, WILSON GARDEN, BANGALORE- 560027 2. 3. NAME OF THE M. S. RAMAIAH MEDICAL COLLEGE INSTITUTION BANGALORE - 560054 COURSE OF THE STUDY AND SUBJECT 4. 5. M.D ANATOMY DATE OF ADMISSION TO THE COURSE 27- 05- 2010 TITLE OF THE TOPIC AN ANATOMICAL STUDY OF INNERVATION OF THE THREE HEADS OF TRICEPS BRACHII 6. BRIEF RESUME OF INTENDED WORK. 6.1. INTRODUCTION AND NEED FOR THE STUDY: The extensor compartment of the arm is occupied by triceps muscle, through which runs the radial nerve and profunda brachii artery. Triceps arises by three heads namely long head, lateral head and medial head1. The long head arises by a flattened tendon from the infraglenoid tubercle of scapula, blending above with the gleno-humeral capsule. Its muscular fibres descend medial to lateral head and superficial to medial head and join them to form a common tendon. The lateral head arises from a narrow, linear, oblique ridge on posterior surface of humeral shaft and from the lateral intermuscular septum. These fibres also converge to the common tendon. Medial head which is overlapped posteriorly by the lateral and long heads has an extensive origin from the entire posterior surface of the humeral shaft, medial side of the radial groove, medial border of humerus, medial intermuscular septum and lower part of the lateral intermuscular septum. Some muscular fibres reach the olecranon directly and the rest converge to the common tendon. The tendon of triceps begins near the middle of the muscle. It has two laminae. One superficial in lower half of the muscle and other in its substance. After receiving the muscle fibres, the two layers unite above the elbow and are attached for the most part to upper surface of olecranon. Innervation - Triceps is innervated by radial nerve, C6, C7 and C8 with separate branches for each head1,2. Radial nerve arises from posterior cord C5, C6, C7, C8 (T1) of the brachial plexus. It descends from the axilla and along with profunda brachii artery it inclines dorsally passing through the triangular space below the lower border of teres major, between long head of triceps and humerus. Here it gives a branch which supplies long head of triceps and a muscular branch to the medial head, which is a long slender filament and lies close to ulnar neve as far as the distal third of arm. It is often termed as ulnar collateral nerve. Radial nerve then spirals obliquely across back of the humerus, lying first between lateral and medial head of triceps and then in a shallow groove deep to the lateral head. A large posterior branch arises from the radial nerve as it lies in humeral groove. It divides to supply medial and lateral heads of triceps. The nerve to medial head is long and descends in medial head of triceps and partially supplies it and passes behind the elbow to end in anconeus1. The presence of a separately innervated muscle unit of triceps may have possible surgical importance and can be used for motor reconstruction. Axillary nerve, ulnar nerve and ulnar collateral branch of the radial nerve are previously unrecognized sources of triceps brachii innervation. Additional study will be directed towards exploring these branches as potential sources for reinnervation of denervated muscle by direct nerve transfer without nerve grafting for management of brachial plexus injuries and biceps brachii denervation and eventually for reinnervation of other muscles in the arm and forearm3,4. 6.2. REVIEW OF LITERATURE: The pattern of triceps innervation is complex and as yet and has not been fully elucidated. Anatomy textbooks report that the motor branch of long head of triceps brachii arises from the radial nerve1,2. A retrospective clinical study of traumatic injuries of the axillary nerve with associated paralysis of the long head of triceps suggests that the motor branch of the long head of triceps may arise from the axillary nerve5. On the basis of cadaver specimen dissection and in vivo motor nerve stimulation, 65% of motor branch of the long head of triceps seems to originate from the axillary nerve3. New advances in peripheral nerve surgery such as neurotization of muscle by direct suture of the nerve end to muscle or transfer of healthy motor nerve branches to motor nerve end of a denervated muscle is used for motor reconstruction. Triceps muscle and its main motor nerve namely the radial nerve have multiple connection modalities. Each of the motor branches to triceps might be used as a donor for nerve transplantation. The motor branch to long head of triceps should be used preferentially when the intention is to establish triceps innervation 6. Motor function of deltoid muscle in patients with complete C5-6 root injury (upper brachial plexus injury) can be restored by transferring the nerve to the long head of triceps to the anterior branch of axillary nerve through a posterior approach7. The contribution of an ulnar nerve branch of motor function to triceps was observed in many surgical procedures that needed ulnar nerve dissection proximal to elbow. The ulnar innervated part of medial head of triceps muscle may be used like an independent motor unit for motor reconstructions4. In elbow surgeries the posterior side of elbow joint are approached through triceps splitting and triceps reflection. Although splitting of fibres of triceps proximally increases the exposure of the posterior humerus, innervation of the lateral portion of the medial head of triceps and anconeus muscle may be jeopardized. Therefore, surgeons interested in elbow surgery should revise the course of the nerve to medial head of triceps and anconeus and try to choose a more conservative posterior surgical approach8. 6. 3. OBJECTIVE OF THE STUDY: 1. To establish the anatomy of motor branches to triceps brachii. 2. To determine the exact origin of motor branch of the long head of triceps brachii. 3. To explore a possible contribution of the ulnar nerve to motor innervation of the medial head of the triceps. 7. MATERIALS AND METHODS: 7.1. SOURCE OF DATA: Materials for this study will be randomly selected 52 upper limbs of formalin embalmed cadavers from the department of anatomy. Study design: Cross sectional study. Study area: M.S.Ramaiah Medical College, Bangalore. Study subject: The study will be performed on 52 upper limbs of formalin embalmed cadavers from department of anatomy, M S Ramaiah Medical College. Sample size: 52, estimated using nMaster software, based on the study- “Does the motor branch of the long head of triceps brachii arise from the radial nerve?”. Considering the nerve supply to long head of triceps is from axillary nerve in 65% of specimens in the above study. Here the alpha error considered is 5% and relative precision is 20%. 7.2. METHOD OF COLLECTION OF DATA: Method of collection of data is by standard dissection method of posterior compartment of the arm in 52 formalin embalmed cadavers. Using a standard medial skin incision at the back of the arm, subcutaneous tissue will be removed. Deep fascia will be removed to expose the triceps muscle which fills the posterior compartment. Superiorly, the medially placed long head of triceps which arises from infraglenoid tubercle of scapula will be separated from the lateral head which has a linear origin from the posterior surfaces of humerus. The nerve supply to each head of triceps will be traced and carefully followed to the source of each nerve branch. Inclusion Criteria: Formalin embalmed upper limb specimens irrespective of age, sex or race. Exclusion Criteria: Upper limbs showing gross asymmetry, any injury to nerve supplying the triceps, or any surgical procedures done at brachial plexus will be excluded as unsuitable. Statistical Analysis: The descriptive study statistics of motor branches of three heads of triceps will be analysed and expressed in percentage. 7.3. Does the study require any investigations or interventions to be conducted on patients or other humans or animals? No 7.4. Has ethical clearance been obtained from your institution? Yes 8. LIST OF REFERENCES 1. Standring, Gray’s anatomy, 38th edition, Upper arm, ELBS. Elsevier, Churchill, Livingstone, 2005; 855. 2. Last R.J, Anatomy Regional and Applied, The Arm, 7th edition. ELBS. Edinburgh. Churchill Livingstone, 1984; 76. 3. De Seze M.P, Rezzouk J, et.al. Does the motor branch of the long head of the triceps brachii arise from radial nerve? Journal of surgical radiological anatomy. 2004; 26: 459-461. 4. Halil Bekler, Valerie M.Wolfe, et.al. A cadaveric study of ulnar nerve innervation of the medial head of triceps brachii. Clinical orthopaedics and related research. 2009; 467: 235-238. 5. Rezzouk J, Durandeau A. Long head of the triceps brachii in axillary nerve injury : anatomy and clinical aspects. Revue de chirurgic orthopedique et reparatrice de’l appareil moteur. 2002; 88: 561-564. 6. Bertelli J A, Santos M A, et.al. Triceps motor branch as donar or reciever in nerve transfer. Neurosurgery. 2007; 6: 333-338. 7.Witooncahart K, et.al. Nerve transfer to deltoid muscle using nerve to long head of triceps. Part 1- an anatomical feasibility study 1. Journal of hand surgery. 2003; 28: 628-632. 8. Ozer H, Acar H I , et.al. Course of the innervation supply of medial head of triceps and anconeus muscle at the posterior aspect of humerus (anatomical study). Archieves of orthopaedic and trauma surgery. 2006; 126: 549-553. 9 SIGNATURE OF THE CANDIDATE The study of innervation of triceps brachii is valuable aid for anatomical studies. Separately innervated muscle unit may have surgical 10 REMARKS OF THE GUIDE importance and can be used for motor reconstruction. This study will facilitate in surgical procedures and nerve grafting. 11 NAME AND DESIGNATION OF DR. SHESHGIRI.C. M.S. SENIOR PROFESSOR AND HEAD 11.1 GUIDE DEPARTMENT OF ANATOMY M.S.RAMAIAH MEDICAL COLLEGE BANGALORE. 11.2 SIGNATURE 11.3 CO GUIDE 11.4 SIGNATURE 11.5 HEAD OF THE DEPARTMENT DR. SHESHGIRI.C. M.S. SENIOR PROFESSOR AND HEAD DEPARTMENT OF ANATOMY M.S.RAMAIAH MEDICAL COLLEGE BANGALORE. 11.6 SIGNATURE 12.1 REMARKS OF PRINCIPAL AND DR. KUMAR S. DEAN M.D. PRINCIPAL AND DEAN, M.S. RAMAIAH MEDICAL COLLEGE, TEACHING AND MEMORIAL HOSPITALS, BANGALORE. 12.2 SIGNATURE