Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
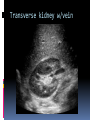
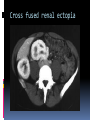
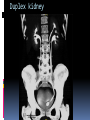
Holdorf ABDOMINAL SONOGRAPHY 1 LECTURE 9 THE KIDNEY AND URINARY TRACT PART 1 Outline Urinary Tract Part I of II Normal anatomy Anatomical Terminology Renal Congenital abnormalities Ectopic Kidney Horseshoe Kidney Cross fused Renalo Ectopia Fused pelvic kidney Dromedary Hump Junctional Parenchymal defect Duplex Kidney Column of Bertin Renal Agenesis Extrarenal Pelvis Posterior Urethral Valves Renal cysts Atypical renal cysts Autosomal Dominant Polycystic kidney disease Autosmal recessive polycystic kidney disease Multicystic Dysplastic kidney Normal Anatomy The paired kidneys and ureters are retroperitoneal, lying against the deep muscles of the back. The right is slightly inferior in location as compared to the left, mostly due to the liver’s location on the right. In relation to the right kidney, the: Adrenal gland is superomedial Liver is superolateral Right colic flexure is inferior 2nd portion of the duodenum is medial The right kidney Gerota’s Fascia The large intestine In relation to the left kidney, the: Adrenal gland and spleen are superior Pancreatic tail is anterior to the upper pole Left colic flexure is inferior The diaphragm, psoas muscle, and quadratus lumborum muscle are on the posterior aspect of the kidneys Diaphragm, psoas muscle Psoas At the hilum of the kidney: Vein exits anteriorly Artery enters between vein and ureter Ureter exits posteriorly The renal hilum (transverse) Transverse kidney w/vein Echogenicity Renal cortex is isoechoic or hypoechoic Medullary pyramids are anechoic Reanl sinus is hyperechoic Echogenicity of the kidney Anatomical Terminology Renal cortex -outer reanl parenchyma from renal sinus to renal capsule (normal= > 1 cm Renal medulla- inner portion of kidney from base of pyramids to center of kidney. Renal sinus-inner hyperechoic portion of kidney which contains fat, calyces, renal pelvis, connective tissue, renal vessels, and lymphatics Renal cortex, medulla Medullary pyramids- anechoic, equally spaced triangles of collecting tubules between cortex and renal sinus. Commonly seen in neonatal and pediatric kidneys. Renal pelvis- funnel shaped transition from the major calyces to the ureter. Renal hilum – medial opening from entry / exit of artery, vein, and ureter. Major calyces- 3 extensions for the renal pelvis Minor calyces- extensions of the major calyces that collects urine from the medullary pyramids. Medullary pyramids, Renal pelvis, renal hilum, major and minor calyces. Renal papilla – apex of medullary pyramids. Gerota’s fascia – fibrous sheath enclosing kidney and adrenal glands. This is also referred to as the perirenal space. Nephron- functional unit of kidney consisting of the renal corpuscle, proximal convoluted tubule, descending and ascending limbs of Henle’s loop, distal convoluted tubule, and collecting tubules. Renal corpuscle (Malpighian body) – consist of glomerulus and glomerular capsule (Bowman’s capsule). Renal Papilla, Gerota’s fascia, Nephron, Renal Corpuscle. RENAL VASCULATURE The kidneys are supplied with arterial blood via the main renal artery which branches off the aorta. At the hilum, the main renal artery divides into 5 segmental arteries. At the level of the medullary pyramids, the segmental arteries divide into the interlobar arteries which travel perpendicular to the renal capsule. At the base of the medullary pyramids, the arcuate arteries branch from the interlobar arteries in the manner that is parallel to the renal capsule. Typically the arcuate arteries are difficult to obtain an ideal spectral waveform as they typically travel perpendicular to the Doppler sound beam. The interlobular arteries are the smallest renal arteries that branch off the arcuate arteries running perpendicular to the renal capsule. Main renal Segmental Interlobar Arcuate Interlobular Renal blood flow Renal congenital abnormalities Embryologically, the kidneys originate in the pelvis and ascend into the upper abdomen so that the upper pole of each kidney is more medial than the lower pole (an inverted “V”). Congenial anomalies of he genitourinary tract are more common than any other organ system. Complications (Obstruction, stasis) associated with congenital abnormalities include: Impaired renal function Infection Calculus formation Ectopic Kidney The word ectopic means displaced or in a location away from the normal position. An ectopic kidney results from failure of the kidneys to ASCEND into the abdomen. Often, an ectopic kidney is also referred to as a pelvic kidney. With ectopic kidneys, there is an increased incidence of UPJ (Ureter-Pelvic Junction) obstruction, ureteral reflux, and multicystic renal dysplasia. Ectopic kidney Horseshoe kidney Most common fusion anomaly in which the lower poles typically connect across the midline anterior to the aorta. The larger U-shaped kidney lies lower in the abdomen because ascent is prevented by the inferior mesenteric artery. Sonographically, the isthmus or connection anterior to the aorta is frequently mistaken for lymphadenopathy. The ureter is typically located anterior to the isthmus. Horseshoe kidney Crossed fused renal ectopia The developing kidneys fuse in the pelvis and one kidney ascends to its normal position, carrying the other one with it across the midline. Two kidneys are visualized on one side of the abdomen with absence of a contralateral kidney. Ureters connect on both sides of the bladder thus one ureter crosses the midline. Cross fused renal ectopia Examples of Cross-Renal ectopia (only D is fused) A. Bilaterally crossed B. S-Shaped C. L-Shaped D. Disc kidney Fused pelvic kidney Kidneys may fuse to form a round mass in the pelvis know as a discord or pancake kidney. Fused pelvic kidney/Pancake kidney Dromedary Hump A common variant of cortical thickening on the lateral aspect of the left kidney. Make certain the “hump” has the same echogenicity as the rest of the renal cortex. Dromedary Hump Junctional parenchymal defect AKA Fetal lobulation Sonographically seen as a triangular hyperechoic area on the anterior aspect of the upper pole of he right kidney. This defect is also known as fetal lobulation, which is partial fusion of the embryonic kidney. Junctional Parenchymal Defect Duplex Kidney This is a duplication of the collecting system which occurs in approximately 15% of the population. The duplication may be: Complete – two ureters Incomplete – one ureter Sonographically, a duplex kidney is typically longer than normal and has a complete central cortical break within the hyperechoic sinus. With complete double ureters, the ureter draining the upper pole typically inserts in an ectopic location on the bladder. A frequent complication of ectopic ureter is a ureterocele; a prolapse of the distal ureter into the bladder. This will result in hydroureter and hydronephrosis of the upper collecting system of the kidney. Duplex kidney Duplex kidney Column of Bertin Hypertrophy of the renal cortical parenchyma located between two medullary pyramids. This may give the appearance of a mass effect although the echogenicity is equal to the peripheral cortical tissue. Column of Bertin Renal Agenesis Bilateral renal agenesis is associated with oligohydramnios and pulmonary hypoplasia. It is incompatible with life. Unilateral renal agenesis is frequently associated with: Bicornuate uterus in females Seminal vesicle agenesis in males. Compensatory hypertrophy of the solitary kidney maintains normal renal function. Extrarenal pelvis The renal pelvis normally is located within the renal sinus. An extrarenal pelvis lies outside the renal sinus sonographically appearing as a cystic collection medial to the renal hilum. Extrarenal pelvis Posterior Uretheral Valve Posterior urethral valve is a common cause of urinary obstruction in the male neonatal patient. This obstruction is due to a flap of mucosa that has a slit-like opening in the area of the prostatic urethra. Sonographic findings include: Large bladder Hydroureter Hydronephrosis Urinoma (an encapsulated collection of extravasated urine- typically found in the area adjacent to the kidneys) Keyhole sign (in the pelvis) PUVs Renal cysts Simple renal cysts occur in 50% of people over the age of 50. Sonographic criteria include: Acoustic enhancement Absence of internal echoes Sharply defined thin wall Round or oval shape Most renal cysts are simple cortical cysts that originate from obstructed uriniferous tubules. Types of renal cysts include: Pylogenic cystscalyceal diverticula that sonographically appear as a simple cyst. Parapelvic cysts- cortical cysts that bulge into the central sinus of the kidney. Paripelvic cysts- lymphatic cysts in the central sinus. Sonographically, the different types of renal cysts can not be distinguished. Ultrasound determines the location of the cyst. Cortical or parenchymal cysts – renal cysts located in the periphery of the kidney. Peripelvic cysts- renal cysts located in the center (RENAL SINUS) of the kidney. A renal psuedoaneurysm may mimic a simple cyst and is typically associated with a history of renal biopsy or trauma. Simple renal cyst Parapelvic cyst Parapelvic cysts that could be mistaken for a dilatated pelvicalyceal system Hemorrhagic renal cyst Atypical renal cysts Cysts with a single thin septation, minimal wall calcification, internal echoes caused by artifact or lobulated shapes may all be associated with simple benign cysts. Characteristics that are atypical and may suggest a malignant cystic lesion include: Multiple thick septation Irregular walls Solid component These cysts should require histological confirmation (FNA) for definitive diagnosis. Atypical renal cyst/ complex renal cyst Autosomal dominant: One of several ways that a trait or disorder can be passed down through families. A pattern of inheritance in which an affected individual has one copy of a mutant gene and one normal gene on a pair of Autosomal chromosomes. Autosomal recessive: A genetic condition that appears only in individuals who have received two copies of an Autosomal gene, one copy from each parent. Autosomal Dominant (adult) polycystic kidney disease: APKD Bilateral renal enlargement due to the development of numerous cysts of varying sizes. Associated with cysts in the liver, pancreas, and spleen. Multiple renal cysts may be identified as early as 20-30 years of age. Destruction of the residual renal tissue in advanced stages leads to renal failure and hypertension. Associated with arterial aneurysms especially cerebral arterial (Berry) aneurysms of the circle of Willis. Adult polycystic kidney disease Autosomal recessive (infantile) Polycystic kidney disease AKA IPCKD Sonographic findings include: Enlarged kidneys bilaterally Hyperechoic parenchyma Loss of cortical medullary distinction Sonographic appearance is due to multiple small cysts throughout the kidney. These cysts result from cystic dilation of the collecting tubules secondary to hyperplasia of eth interstitial portions of the ducts. Associated with Renal dysfunction Pulmonary hypoplasia Periportal fibrosis Portal hypertension Autosomal recessive polycystic kidney disease may be detected in utero with oligohydramnios. IPCKD Multicystic Dysplastic Kidney Most common cause of abdominal mass in NEWBORNS. It is typically unilateral, although may be bilateral. This non-functioning kidney consists of noncommunicating cysts with the absence of renal parenchyma. Usually the result of atresia of the uretro-pelvic junction during fetal development. Associated renal anomalies include: Contralateral UPJ obstruction. Contralateral renal agenesis or hypoplasia Horseshoe kidney Multicystic Dysplastic Kidney Neonate Diagnostic Medical Sonography Program Abdominal Sonography I Urinary Tract Part I of II Homework Define a hypertrophied Column of Bertin and show an image of it. What is a duplex collecting system and how an image of it. What is multicystic dysplastic kidney and show several images of it. Explain the scanning technique for imaging the kidneys with ultrasound. Include in your answer imaging the renal arteries. Explain the anomalies related to the ascent of the kidney. Provide an image of a horseshoe kidney. 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. 11. 12. 13. 14. 15. Name three notable structures posterior to the kidneys. What is the orientation of structures that enter and exit the renal hilum? Trace the branches or the renal artery. Name the fascia which encloses the kidneys, adrenal glands, and perinephric fat. What renal structure is a concentrated area of collecting tubules which is sonographically seen in newborns and infants as hypoechoic equally space triangles. Bilateral renal agenesis associated with Oligohydramnios and pulmonary hypoplasia is incompatible with life. What is associated with UNILATERAL renal agenesis? Describe the development and sonographic appearance of crossed renal ectopia and crossed fused renal ectopia. Describe the development and sonographic appearance of a horseshoe kidney. A duplex kidney is discovered with dilation of the upper pole collecting system. In this situation, is there partial or complete ureter duplication? What is the most common cause of urinary obstruction in male neonates? What are the sonographic findings of urinary obstruction in male neonates? Describe the appearance of a dromedary hump. Describe the appearance of a junctional parenchymal defect. Describe the appearance of eh column of Bertin. Describe the appearance of an extra renal pelvis.