Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
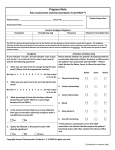
IMAGING REQUEST FORM Referring Clinician:(please print) X Number: Appt. Date & Time: Surname: Address: Forename: Account to be billed (tick) PRIVATE GP PRACTICE Address: (No LOG required) Telephone: INSURANCE (Pre-auth required for CT, Postcode: MRI and Nuclear Med.) Patient Contact Details: Date of birth: CLIENT E-mail / Fax: (No LOG required) Sex: Male □ Female Mobility: Walking □ □ Chair THIRD PARTY / EMBASSY (LOG required) □ Trolley □ PATIENT Preferred Radiologist: (Payment required) Authorisation No. / Fee Quoted: Examination Requested: Under the IR(ME)R 2000 regulations, all Imaging Requests must be justified by an Imaging Department practitioner to ensure that there is a net benefit, from the examination, to the patient. Therefore, any request that is illegible, unsigned by a doctor or clinical nurse specialist or lacking the required information will be returned for completion. Clinical Information: Referring Clinician Signature: Date: I V Contrast (Iodine or Gadolinium): To minimise the risk of contrast nephrotoxicity it is the responsibility of the referring clinician to provide an indication of renal status or to ensure that a recent eGFR and a serum creatinine level are available. Serum Creatinine: eGFR: Date measured: Initials: M R I: Does the patient have any of the following contra-indications? History of intra-orbital FB? Intracranial Aneurysm clips? Cardiac Pacemaker / ICD? Prosthetic Heart Valve? Exam Comments: DAP: Operator: Date: The Manchester Institute of Health and Performance 299 Alan Turning Way Manchester M11 3BS T: 0161 641 8300 HCA International Ltd | Registered Office: 242 Marylebone Road, London NW1 6JL. Registered in England No. 3020522 52AR.RAD.FORM.100 v2 Feb 15