Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
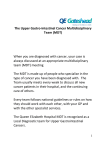
Trust Cancer Lead Clinician Presented by: Professor Clem F. Kiire – MD, FRCP Consultant Physician & Gastroenterologist Southport & Ormskirk Hospital NHS Trust www.southportandormskirk.nhs.uk 15 September 2008 Southport & Ormskirk Hospital Trust Background • A merger of two trusts, formerly West Lancashire NHS Trust and Southport & Formby Trust took place on 1 April 1999; the new Trust being named Southport & Ormskirk Hospital NHS Trust. • Southport & Ormskirk Hospital NHS Trust consists of two hospitals, one in Southport (Southport & Formby District General Hospital) and one in Ormskirk (Ormskirk & District General Hospital), some eight miles apart. The Trust provides a wide range of clinical services to the resident population of Southport & Formby and Ormskirk and surrounding districts, the catchment population being approximately 240,000 – the figure being equally divided between the two areas. Cancer Management Team Structure Southport & Ormskirk Hospital NHS Trust CANCER SERVICES ORGANISATION Executive Lead DEPUTY CHIEF EXECUTIVE Lead Clinician (Breast) Lead Clinician (Cancer) Lead Clinician (Lung) Cancer Services Manager Lead Clinician (Colorectal) Lead Nurse (Cancer) Lead Clinician (Gynaecology) Lead Clinician (Upper GI) Service Improvement Facilitator Lead Clinician (Urology) Cancer Service Support Manager (MDT Co-ordination/Cancer Patient Tracking) MDT Cancer Support Officers & Assistants (team of x 6) PA/Cancer Services Secretary x 2 Lead Clinician (Skin) Lead Clinician (Haematology) Lead Clinician (Palliative Care) Cancer Services Cancer Services Manager PA to Cancer Management Team PA to Cancer Lead Clinicians (x2) Cancer Research Nurse Practitioner Cancer Services Support Manager (employed & funded by Merseyside & Cheshire Cancer Research Network) Lead Cancer Nurse Clinical Trials Data Co-ordinator (funded by Cancer Research Network) Cancer Services Support Officer Cancer Services Support Officer Cancer Services Support Assistant Cancer Services Support Officer Cancer Services Support Assistant Cancer Services Support Officer Trust Cancer Lead Clinician Main Duties • Ensure site specific specialist MDTs are established. • Ensure there are mechanisms in place for the care of cancer patients to be formally reviewed by a specialist MDT either through direct assessment or through formal discussion with the team by the responsible clinician. • Ensure there is adequate non-surgical oncology support for cancer care. • In collaboration with the Lead Nurse, Lead Manager and other colleagues, supports and advises on the implementation of the national cancer services standards. Trust Cancer Lead Clinician Main Duties Cont: • Work with the Lead Nurse and Lead Manager to coordinate the preparation for peer review visits, including self-assessment against the national standards. • Work with the Lead Nurse and Lead Manager to ensure the implementation of the resulting action plans for continuous quality improvement. • To take part in the NHS Trust’s clinical governance activities which are of relevance to the cancer services of the Unit. • Ensure arrangements are in place for audit and continuing medical education with reference to cancer services. Trust Cancer Lead Clinician Main Duties Cont: • Meet regularly with colleagues from cancer centres/units and primary care representatives within the network to enable working to uniform standards. • Meet regularly with at least some representation from the community (eg patients and users and representatives). • Advise on and support the development of data collection on cancer services, in collaboration with the Cancer Registry and with cancer services in the network. • Develop the network wide services of the Cancer Unit MDT Lead Clinician Responsibilities • Ensure that objectives of MDT working (as laid out in Manual of Cancer Service Standards) are met: • To ensure that designated specialists work effectively together in teams such that decisions regarding all aspects of diagnosis, treatment and care of individual patients and decisions regarding the team’s operational policies are multidisciplinary decisions. • To ensure mechanisms are in place to support entry of eligible patients into clinical trials, subject to patients giving fully informed consent. MDT Lead Clinician Responsibilities continued: • Ensure that target of 100% of cancer patients discussed at the MDT is met. • To ensure that care is given according to recognised guidelines (including guidelines for onward referrals) with appropriate information being collected to inform clinical decision making and to support clinical governance/audit. • Overall responsibility for ensuring that MDT meeting and team meet Peer Review Quality Measures. MDT Lead Clinician Responsibilities continued: • Ensure attendance levels of core members are maintained, in line with Quality Measures. • Provide link to CNG, either by attendance at meetings or by nominating another MDT member to attend. • Lead on, or nominate lead for service improvement. MDT Lead Clinician Responsibilities continued: • Organise and chair annual meeting examining functioning of team and reviewing operational policies, and collate any activities that are required to ensure optimal functioning of the team (e.g. training for team members). • Ensure MDT’s activities are audited and results documented • Ensure that the outcomes of the meeting are clearly recorded and clinically validated and that appropriate data collection is supported. • Ensure target of communicating MDT outcomes to primary care is met. Management Meetings Internal External • Chair – Cancer Lead Clinicians’ Group (meets 3 x year) • PCT Locality Implementation Team meetings • Cancer Services Manager weekly update meetings • Merseyside & Cheshire Cancer Network:- • Tumour Groups: – – – – – Breast (meets 2 x year) Colorectal/Upper GI (quarterly) Urology (3 x year) Lung (quarterly) Gynaecology (quarterly) – Taskforce Group – Lead Clinician/CNG – Clinical Network Groups Multi-disciplinary Teams (MDTs) Southport & Ormskirk Hospital NHS Trust has well-established MDT’s in the following specialties. In addition, members of the teams also provide input into specialist multi-disciplinary teams (MDT’s) within the Network. • • Colorectal Upper Gastrointestinal (Liver & Pancreatic input into Aintree Hospitals & Royal Liverpool Hospital sMDTs) • • • • • • • Breast Urology Lung Gynaecology (input into Liverpool Women’s Hospital sMDT) Haematology (input into Aintree Hospitals sMDT) Skin (input into Royal Liverpool/Broadgreen sMDT) Head and Neck (input into Aintree Hospitals sMDT) Ten Most Common Cancers Southport & Formby Residents Pie chart of the 10 most common cancers occurring in Southport & Formby residents, 2001-2005 Females Males Pancreas 2% other 19% Non Melanoma skin cancer 23% Malignant melanoma 2% Non Melanoma skin cancer 24% Rectum 2% Malignant Oesophagus 3% neoplasm without specification of Ovary site 3% 3% Rectum 3% Stomach 3% Bladder 5% Colon 7% Liver 2% other 20% Prostate 22% Lung 11% Source: North West Cancer Intelligence Service (NWCIS) – data based on PCT geographic boundaries as at 2001-2005 Malignant melanoma 3% Uterus 4% Colon Lung 6% 9% Breast 24% Ten Most Common Cancers West Lancashire Residents Pie chart of the 10 most common cancers occurring in West Lancashire residents, 2001-2005 other 17% Pancreas Malignant 2% melanoma 3% Males Non Melanoma skin cancer 24% Oesophagus 3% Rectum 4% Bladder 4% Stomach 4% Colon 6% Females Prostate 21% Lung 12% Source: North West Cancer Intelligence Service (NWCIS) – data based on PCT geographic boundaries as at 2001-2005 other 21% Breast 26% Pancreas 2% Malignant melanoma 2% Rectum 3% Uterus 3% Malignant neoplasm without specification of site 4% Ovary 4% Colon 6% Lung 9% Non Melanoma skin cancer 20% Cancer Waiting Time Targets During 2007/08 the Trust was successful in delivering all of the National Cancer Treatment Times targets. This was achieved following detailed work to streamline patient pathways, examine capacity and demand, establish a tracking system for all cancer patients and adopt other service improvement methodology. Targets Met • 14 Day Target - (A 2 week maximum wait for urgent GP referrals) – 100% compliance maintained throughout the year. • 31 Day Target - (A maximum waiting time of 1 month from diagnosis to treatment for all cancers) – Exceeded the national standard of 98% and England average performance, by achieving an overall compliance of 99.6%. • 62 Day Target - (A maximum waiting time of 2 months from urgent GP referral to treatment for all cancers) – Exceeded the national standard of 95% and England average performance, by achieving an overall compliance of 97.6%. Extended waiting times standards • By Dec 2008 - patients will wait no longer than 31 days for second or subsequent surgery & chemotherapy. • By Dec 2008 – all patients with a suspected cancer detected through screening programmes or by a hospital consultant will be treated within 62 days. • By Dec 2009 - all women referred by their GP with breast symptoms will be seen within 2 weeks. • By Dec 2010 – where radiotherapy is a second or subsequent treatment this will be done within 31 days. Peer Review • The Cancer Peer Review programme aims to improve care for people with cancer & their families. The process involves teams of specialist reviewers who are responsible for making judgements on the level of compliance against National Measures for each of the tumour sites. Qualitative elements of care & treatment are explored, including governance, leadership, teamwork, research, patient involvement & end of life care. • Following the two day Peer Review visit to the Hospital Trust in Autumn 2005 the final report highlighted that the review team considered the Locality/NHS Hospital Trust as an exemplar in its approach to Cancer Services Peer Review and its Palliative Care Services in particular. The service also had a successful peer review appraisal visit in 2007. Trust Cancer Lead Clinician In Summary: • Essentially the role is that of Lead Clinician for a Hospital Trust. Reporting to the Executive Director for Cancer, the Lead Clinician will ensure that cancer services are managed and organised effectively to support high quality care. The role is to provide clear leadership of the cancer unit and working with the Lead Manager and Lead Nurse to deliver the increasing agenda set out in the National Cancer Plan and Cancer Services Standards.