Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
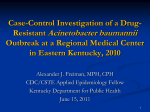
Journal of Medical Microbiology (2014), 63, 1154–1159 DOI 10.1099/jmm.0.071712-0 Rapid identification of Acinetobacter baumannii, Acinetobacter nosocomialis and Acinetobacter pittii with a multiplex PCR assay Te-Li Chen,1,2 Yi-Tzu Lee,1,3 Shu-Chen Kuo,1,2,4 Su-Pen Yang,2,5 Chang-Phone Fung1,2,5 and Shou-Dong Lee6 Correspondence 1 Shou-Dong Lee 2 [email protected] Institutes of Clinical Medicine, School of Medicine, National Yang-Ming University, Taipei, Taiwan Division of Infectious Diseases, Taipei Veterans General Hospital, Taipei, Taiwan 3 Department of Emergency, Taipei Veterans General Hospital, Taipei, Taiwan 4 National Institute of Infectious Diseases and Vaccinology, National Health Research Institutes, Miaoli County, Taiwan 5 Emergency and Critical Care Medicine, National Yang-Ming University, Taipei, Taiwan 6 Department of Medicine, Cheng Hsin General Hospital, Taipei, Taiwan Received 9 December 2014 Accepted 24 June 2014 Acinetobacter baumannii, Acinetobacter nosocomialis and Acinetobacter pittii are clinically relevant members of the Acinetobacter calcoaceticus–A. baumannii (Acb) complex and important nosocomial pathogens. These three species are genetically closely related and phenotypically similar; however, they differ in their epidemiology, antibiotic resistance and pathogenicity. In this study, we investigated the use of a multiplex PCR-based assay designed to detect internal fragments of the 16S–23S rRNA intergenic region and the gyrB and recA genes. The assay was capable of differentiating A. baumannii, A. nosocomialis and A. pittii in a reliable manner. In 23 different reference strains and 89 clinical isolates of Acinetobacter species, the assay accurately identified clinically relevant Acb complex species except those ‘between 1 and 3’ or ‘close to 13TU’. None of the non-Acb complex species was misidentified. In an analysis of 1034 positive blood cultures, the assay had a sensitivity of 92.4 % and specificity of 98.2 % for Acb complex identification. Our results show that a single multiplex PCR assay can reliably differentiate clinically relevant Acb complex species. Thus, this method may be used to better understand the clinical differences between infections caused by these species. INTRODUCTION Acinetobacter baumannii, Acinetobacter nosocomialis and Acinetobacter pittii have become important nosocomial pathogens worldwide (Dijkshoorn et al., 2007; Peleg et al., 2008). These three clinically relevant Acinetobacter species, as well as an environmental species, Acinetobacter calcoaceticus (Nemec et al., 2011), cannot be reliably differentiated with phenotypic tests. Because of their similar phenotypic characteristics, these four species are grouped as A. calcoaceticus–A. baumannii (Acb) complex (Gerner-Smidt et al., 1991). A. baumannii is distinct from A. nosocomialis and A. pittii, being resistant to more classes of antimicrobial agents, associated with a relatively worse clinical outcome and responding differently to appropriate therapy (Lee et al., 2010, 2012b; Chuang et al., 2011; Wisplinghoff et al., 2012; Abbreviations: Acb, Acinetobacter calcoaceticus–Acinetobacter baumannii; ITS, intergenic spacer; MALDI-TOF MS, matrix-assisted laser desorption ionization–time of flight mass spectrometry. 1154 Kuo et al., 2013). Methods that can differentiate these three clinically relevant Acinetobacter species are critical for advancing our knowledge of the biology, pathogenicity and therapy of these individual species. The use of PCR assays offers the potential for rapid detection and species identification of pathogens (Fredricks & Relman, 1998). In this study, we describe a multiplex PCR-based assay that can differentiate A. baumannii, A. nosocomialis and A. pittii in bacterial colonies and positive blood culture media. METHODS Bacterial isolates and identification. Three sets of bacteria were examined in this study. The first set of bacteria included 23 reference strains and 89 clinical isolates of Acinetobacter species with known genomic species identification (Table 1). The reference strains were purchased from public culture collections or kindly provided by T.-C. Chang (Chang et al., 2005) and Alexandr Nemec (Nemec et al., Downloaded from www.microbiologyresearch.org by 071712 G 2014 The Authors IP: 88.99.165.207 On: Sun, 14 May 2017 02:03:14 Printed in Great Britain Rapid identification of the Acb complex Table 1. Reference and clinical isolates used to validate the multiplex PCR assay for the identification of A. baumannii, A. nosocomialis and A. pittii Genomic species Acinetobacter Acinetobacter Acinetobacter Acinetobacter Acinetobacter Acinetobacter Acinetobacter Acinetobacter Acinetobacter Acinetobacter Acinetobacter Acinetobacter Acinetobacter Acinetobacter Acinetobacter Acinetobacter Acinetobacter Acinetobacter Acinetobacter Acinetobacter Acinetobacter Acinetobacter Acinetobacter Acinetobacter Acinetobacter Acinetobacter Acinetobacter Total Reference strains calcoaceticus baumannii pittii haemolyticus junii genomic species 6 johnsonii lwoffii bereziniae guillouiae* radioresistens nosocomialis genomic species 13BJ/14TU genomic species 15TU genomic species 15BJ genomic species 16 genomic species 17 baylyi beijerinckii* gyllenbergii* parvus schindleri soli* ursingii venetianus belonging to ‘close to 13TU’ belonging to ‘between 1 and 3’ ATCC 17987 ATCC 19606T and 15151 ATCC 17922T ATCC 17906T ATCC 17908T ATCC 17979 ATCC 17909T 0 0 LMG 988T ATCC 43998T ATCC 17903 0 CCUG 26390 CCUG 34436 BCRC 15883 CCUG 34437 ATCC 33305 NIPH 838T NIPH 2150T CCUG 48800T LMG 19576T CCUG 59023T LMG 19575T CCUG 45561T 0 0 No. clinical isolates 0 20 12 1 5 0 0 2 3 1 3 14 2 4 0 0 0 7 1 1 0 1 1 5 0 4 2 89 *Generous gifts from Professor A. Nemec. 2009, 2010). The clinical isolates were collected from 10 different medical centres in Taiwan (Chen et al., 2010) or generously provided by Alexandr Nemec (Nemec et al., 2009, 2010). The second set of bacteria comprised 100 clinical Acb complex isolates that were obtained from the Taipei Veterans General Hospital, without knowledge of the genomic species prior to PCR identification. These two sets of Acinetobacter isolates were used to verify the practicality of the multiplex PCR method. Acinetobacter species were identified by sequence analysis of the 16S–23S rRNA intergenic spacer (ITS) region (Chang et al., 2005), amplified rDNA restriction analysis (Dijkshoorn et al., 1998; Nemec et al., 2003, 2011) and rpoB sequence cluster analysis (Nemec et al., 2009). Clonality of the clinical isolates of A. baumannii, A. pittii and A. nosocomialis was determined by PFGE by using the ApaI enzyme as described previously (Huang et al., 2008). The third set comprised 1034 micro-organisms of different genera and species (Table 2), based on results of the VITEK 2 system (bioMérieux), that were prospectively collected from the Taipei Veterans General Hospital from July 2010 to June 2012. This set was used to test whether the multiplex PCR method could directly detect and identify Acb complex in blood culture media. Development of the multiplex PCR assay. Three pairs of primers that had been previously designed and verified were included in the multiplex PCR assay. The primers P-rA1 (59-CCTGAATCTTCTGGTAAAAC-39) and P-rA2 (59-GTTTCTGGGCTGCCAAACATTAC-39), http://jmm.sgmjournals.org which target a highly conserved 425 bp region of the recA gene of Acinetobacter species, were used as a reaction control (Krawczyk et al., 2002). Primers sp4F (59-CACGCCGTAAGAGTGCATTA-39) and sp4R (59-AACGGAGCTTGTCAGGGTTA-39) yielded an amplicon of 294 bp from the gyrB genes of A. baumannii and A. nosocomialis (Higgins et al., 2007). Primers P-Ab-ITSF (59-CATTATCACGGTAATTAGTG-39) and P-Ab-ITSB (59-AGAGCACTGTGCACTTAAG39) were used to specifically amplify an internal 208 bp fragment from the ITS region of A. baumannii (Chen et al., 2007). For identification of A. pittii, all of the available ITS sequences of different Acinetobacter species deposited in GenBank were downloaded and aligned using CLUSTAL W software. After considering specificity and annealing temperature, primers P-AGS3-F (59-CTCAAGAGTTTAGATTAAGCAAT-39) and P-AGS3-R (59-GTCCGTGCGATTCTTCATCG-39) were selected to amplify a 150 bp internal fragment from the ITS region of A. pittii. GoTaq Flexi DNA polymerase (Promega) was used for PCR assays performed in the GeneAmp PCR System 2700 (Applied Biosystems). PCR amplification consisted of an initial denaturation step at 94 uC for 5 min; 35 cycles at 94 uC for 1 min, 58 uC for 30 s and 72 uC for 30 s; and a final extension at 72 uC for 10 min. For the PCR assays of the first and second sets of Acb complex isolates, the DNA template was prepared by boiling (Vaneechoutte et al., 1995). For the bacterial PCR assays from blood culture media, the DNA templates were prepared as described in the following section. Downloaded from www.microbiologyresearch.org by IP: 88.99.165.207 On: Sun, 14 May 2017 02:03:14 1155 T.-L. Chen and others Table 2. Clinical isolates used in the validation of the multiplex PCR assay for detection and identification of A. baumannii, A. nosocomialis and A. pittii from positive blood cultures Micro-organism* n Multiplex PCR result A. b Gram-negative bacteria A. baumannii A. nosocomialis A. pittii A. junii A. lwoffii Other Acinetobacter spp.D Achromobacter spp. Aeromonas hydrophila Aeromonas sobria Bacteroides fragilis group Burkholderia cepacia Chryseobacterium indologenes Chryseobacterium meningosepticum Citrobacter diversus Citrobacter freundii Comamonas testosteroni Escherichia coli Enterobacter aerogenes Enterobacter asburiae Enterobacter cloacae Fusobacterium spp. Klebsiella oxytoca Klebsiella ozaenae Klebsiella pneumoniae Kluyvera ascorbata Morganella morganii Pantoea spp. Plesiomonas shigelloides Prevotella spp. Proteus mirabilis Proteus penneri Providencia stuartii Pseudomonas aeruginosa Pseudomonas putida Ralstonia mannitolilytica Salmonella group B Salmonella group D Salmonella paratyphi Serratia marcescens Shewanella algae Sphingomonas paucimobilis Stenotrophomonas maltophilia Vibrio fluvialis Vibrio mimicus Gram-positive bacteria Bacillus spp. Coagulase-negative Staphylococcus spp. Corynebacterium spp. Enterococcus faecalis Enterococcus gallinarum Enterococcus spp. Lactobacillus spp. 1156 981 70 51 10 1 2 9 4 10 1 9 12 10 12 9 6 1 372 18 1 36 1 7 1 180 1 4 1 1 2 24 2 1 40 3 1 3 30 1 13 1 2 15 2 1 46 2 18 2 1 1 4 1 76 65 0 0 0 0 0 0 1 0 0 0 0 0 0 0 0 0 0 0 4 0 0 0 4 0 0 0 0 0 1 0 0 0 1 0 0 0 0 0 0 0 0 0 0 2 0 0 1 0 0 1 0 A. n A. p Negative 50 0 48 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 1 0 1 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 8 0 0 8 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 1 0 0 0 0 0 0 0 847 5 3 2 1 2 9 4 9 1 9 12 10 12 9 6 1 372 18 1 31 1 6 1 176 1 4 1 1 2 23 2 1 40 2 1 3 30 1 13 1 2 15 2 1 43 2 18 1 1 1 3 1 Downloaded from www.microbiologyresearch.org by IP: 88.99.165.207 On: Sun, 14 May 2017 02:03:14 Journal of Medical Microbiology 63 Rapid identification of the Acb complex Table 2. cont. Micro-organism* n Multiplex PCR result A. b Rhodococcus equi Staphylococcus aureus Staphylococcus hominis Streptococcus agalactiae Streptococcus group C Streptococcus group D Viridans group streptococci Yeast Total 1 11 1 1 1 1 1 7 1034 A. n A. p Negative 0 0 0 0 0 0 0 0 50 0 1 0 0 0 0 0 0 9 1 10 1 1 1 1 1 7 897 0 0 0 0 0 0 0 0 78 A. b, A. baumannii; A. n, A. nosocomialis; A. p, A. pittii. *Acinetobacter species identification of the Acb complex was performed using the PCR method; A. junii and A. lwoffii were identified using amplified rDNA restriction analysis and rpoB sequence cluster analysis. DIncluding A. haemolyticus (n51), A. johnsonii (n52), A. bereziniae (n51), A. radioresistens (n51), Acinetobacter genomic species 13BJ/14TU (n51), A. baylyi (n51) and A. ursingii (n52). All were identified using rpoB sequence cluster analysis. DNA purification from blood culture media. When bacterial growth was detected in the culture bottle by the culture system (BacT/ Alert; Organon Teknika), 0.5 ml culture medium was collected from the bottle and analysed by Gram staining. Samples that yielded Gramnegative coccobacilli or bacilli were subjected to DNA purification followed by multiplex PCR identification. Gram-positive organisms and yeast collected in the first 2 weeks were used to validate the PCR identification method. DNA purification from positive culture media was performed using the benzyl alcohol–guanidine hydrochloride organic extraction method, as described previously (Fredricks & Relman, 1998). Briefly, 0.1 ml inoculated blood culture media was treated with lysis buffer containing guanidine hydrochloride in Tris buffer and then mixed with 99 % benzyl alcohol (Sigma-Aldrich). DNA templates in the aqueous supernatant were precipitated with sodium acetate and 2-propanol. A. pittii. For Acinetobacter isolates not belonging to the Acb complex, only a 425-bp fragment corresponding to the recA gene was found (Fig. 1, lane 1). Two bands, one corresponding to the recA gene and the other to the gyrB gene (294 bp), were found in A. baumannii and A. M 1 2 3 4 5 M RESULTS AND DISCUSSION Validation of the multiplex PCR assay in identifying A. baumannii, A. nosocomialis and A. pittii Among the 23 reference and 89 clinical Acinetobacter isolates in the first set of bacteria analysed (Table 1), the PCR method showed 100 % sensitivity for the identification of A. baumannii (n522), A. nosocomialis (n513) and A. pittii (n515). However, this method could not identify Acinetobacter species belonging to ‘between 1 and 3’ or ‘close to 13TU’ (generous gifts from Alexandr Nemec). Isolates belonging to ‘between 1 and 3’ were identified as A. pittii, whereas those belonging to ‘close to 13TU’ were identified as A. nosocomialis or showed patterns combining A. nosocomialis and A. pittii (data not shown). Since these Acinetobacter species are rare and their clinical importance has not been delineated, this rapid method is still appropriate for identifying Acb complex. Among the 56 non-Acb complex isolates, none was misidentified as any of A. baumannii, A. nosocomialis or http://jmm.sgmjournals.org 500 bp Fig. 1. Multiplex PCR products resolved by agarose gel electrophoresis. PCR analyses were performed using A. baumannii-specific primers (P-Ab-ITSF and P-Ab-ITSB), internal control primers (P-rA1 and P-rA2) specific for the recA gene of all Acinetobacter species, A. nosocomialis-specific primers (gyrBdirected primers: sp4F and sp4R) and A. pittii-specific primers (AGS3-R and AGS3-F). Lanes: M, 100 bp DNA ladder; 1, A. calcoaceticus; 2, A. baumannii; 3, A. pittii; 4, A. nosocomialis; 5, negative control. Downloaded from www.microbiologyresearch.org by IP: 88.99.165.207 On: Sun, 14 May 2017 02:03:14 1157 T.-L. Chen and others nosocomialis isolates. A. baumannii was differentiated from A. nosocomialis by the presence of another fragment corresponding to its ITS region (208 bp) (Fig. 1, lane 2). Two fragments were observed for the A. pittii isolate and ‘between 1 and 3’, one corresponding to the recA gene and the other to the ITS region (150 bp) (Fig. 1, lane 3). The multiplex PCR method was then validated using the second set of 100 clinical Acb complex isolates. This method correctly identified 48 isolates as A. baumannii, 15 as A. pittii and 35 as A. nosocomialis. In addition, two nonAcb complex Acinetobacter species (Acinetobacter lwoffii and Acinetobacter johnsonii) were found. The identification of all species was confirmed by ITS sequence analysis. PFGE results showed that the clinical Acb complex isolates in the first and second sets had diverse pulsotypes (data not shown). At present, PCR-based methods to identify A. baumannii use primers that specifically amplify a fragment from blaOXA51-like genes, which are intrinsic to this species (Turton et al., 2006), and the ITS region of this species (Chen et al., 2007). However, blaOXA51-like genes have spread to other Acinetobacter species and may not be fully reliable targets for identifying A. baumannii (Lee et al., 2012a). Another PCR method targeting gyrB can differentiate between A. baumannii and A. nosocomialis (Higgins et al., 2007), and this gyrB multiplex has been expanded to enable the identification of A. calcoaceticus and A. pittii (Higgins et al., 2010). In the present study, we developed a multiplex PCR method that is able to differentiate the three clinically relevant Acb complex species in a single reaction. Although matrix-assisted laser desorption ionization–time of flight mass spectrometry (MALDI-TOF MS) is increasingly used for species identification, it can only be applied to bacterial colonies and not to blood samples (Šedo et al., 2013). In addition, the accuracy of MALDI-TOF MS has been described as ‘not acceptable for species-level identification of Acinetobacter spp.’ (Šedo et al., 2013). Application of the multiplex PCR method to identify A. baumannii, A. nosocomialis and A. pittii from positive blood culture media A total of 1034 positive blood culture samples were prospectively collected over a period of 24 months, consisting of 131 blood cultures showing growth of Acb complex isolates (70 A. baumannii, 51 A. nosocomialis and 10 A. pittii) and 903 positive blood cultures showing growth of organisms other than Acb complex (Table 2). Genomic species identifications of the Acb complex isolates were verified using a DNA template prepared from colonies. Genomic species identification of other Acinetobacter isolates was performed using different molecular methods, as shown in the footnotes to Table 2. Among the 1034 positive blood culture samples, the multiplex PCR assay had a sensitivity of 92.4 % (121/131) and specificity of 98.2 % (887/903). Among the 981 blood culture specimens positive for Gram-negative organisms, the multiplex PCR assay had 1158 a sensitivity of 92.4 % (121/131) and specificity of 98.5 % (837/850). All reactions were completed within 4 h. False-positive and -negative results may be a significant drawback to the multiplex method. False-positive results were observed in 16 blood culture samples, showing growth of Aeromonas hydrophila (n51), Enterobacter cloacae (n55), Klebsiella pneumoniae (n54), Klebsiella oxytoca (n51), Proteus mirabilis (n51), Pseudomonas putida (n51), Corynebacterium species (n51), Enterococcus species (n51) and Staphylococcus aureus (n51). One possible explanation is that Acb complex species were present in these blood culture media but in too few numbers to be detected on agar plates with routine blood culture methods, while the moresensitive multiplex PCR assay was able to identify them. To prove this hypothesis, multiple sets of blood cultures or a larger volume of blood may be needed to increase the diagnostic yield. However, the clinical significance of the presence of such a small amount of bacteria in blood needs to be further investigated. An alternative explanation is that the primers non-specifically bind to the DNA of organisms other than Acb complex. However, this theory is refuted by the negative multiplex PCR results obtained with these nonAcinetobacter bacterial colonies as templates. False-negative results were observed in 10 blood culture samples, which showed the growth of A. baumannii (n55), A. nosocomialis (n53) and A. pittii (n52). These results may be attributed to contamination with Acb complex species during the phenotypic identification process or the presence of PCR inhibitors in the samples, even after DNA purification with benzyl alcohol extraction. In conclusion, we have developed a convenient, rapid and cost-effective method that can identify the three clinically relevant Acb complex species. This method provides an opportunity to better understand the biology, pathogenicity and ecology of individual Acinetobacter species of the Acb complex. ACKNOWLEDGEMENTS This work was supported by grants from the Fund of Cheng Hsin General Hospital and Yang-Ming University (102F218C06), the Taipei Veterans General Hospital (V101E4-003 and V101C-021), the National Science Council (NSC98-2314-B-010-010-MY3) and the Yen Tjing Ling Medical Foundation (CI-100-35). This work was performed at Taipei Veterans General Hospital, No. 201, Section 2, Shih-Pai Road, Taipei 11217, Taiwan. REFERENCES Chang, H. C., Wei, Y. F., Dijkshoorn, L., Vaneechoutte, M., Tang, C. T. & Chang, T. C. (2005). Species-level identification of isolates of the Acinetobacter calcoaceticus–Acinetobacter baumannii complex by sequence analysis of the 16S-23S rRNA gene spacer region. J Clin Microbiol 43, 1632–1639. Chen, T. L., Siu, L. K., Wu, R. C., Shaio, M. F., Huang, L. Y., Fung, C. P., Lee, C. M. & Cho, W. L. (2007). Comparison of one-tube multiplex PCR, automated ribotyping and intergenic spacer (ITS) sequencing Downloaded from www.microbiologyresearch.org by IP: 88.99.165.207 On: Sun, 14 May 2017 02:03:14 Journal of Medical Microbiology 63 Rapid identification of the Acb complex for rapid identification of Acinetobacter baumannii. Clin Microbiol Infect 13, 801–806. Chen, T. L., Lee, Y. T., Kuo, S. C., Hsueh, P. R., Chang, F. Y., Siu, L. K., Ko, W. C. & Fung, C. P. (2010). Emergence and distribution of non-baumannii species of Acinetobacter harboring a blaOXA-51-like gene that is intrinsic to A. baumannii. Antimicrob Agents Chemother 56, 1124–1127. Lee, Y. T., Kuo, S. C., Yang, S. P., Lin, Y. T., Tseng, F. C., Chen, T. L. & Fung, C. P. (2012b). Impact of appropriate antimicrobial therapy on plasmids bearing the blaOXA-51-like gene with an upstream ISAba1 in carbapenem-resistant Acinetobacter baumannii isolates in Taiwan. Antimicrob Agents Chemother 54, 4575–4581. mortality associated with Acinetobacter baumannii bacteremia: relation to severity of infection. Clin Infect Dis 55, 209–215. Chuang, Y. C., Sheng, W. H., Li, S. Y., Lin, Y. C., Wang, J. T., Chen, Y. C. & Chang, S. C. (2011). Influence of genospecies of Acinetobacter Nemec, A., Dijkshoorn, L., Cleenwerck, I., De Baere, T., Janssens, D., Van Der Reijden, T. J., Jezek, P. & Vaneechoutte, M. (2003). baumannii complex on clinical outcomes of patients with Acinetobacter bacteremia. Clin Infect Dis 52, 352–360. Acinetobacter parvus sp. nov., a small-colony-forming species isolated from human clinical specimens. Int J Syst Evol Microbiol 53, 1563– 1567. Dijkshoorn, L., Van Harsselaar, B., Tjernberg, I., Bouvet, P. J. & Vaneechoutte, M. (1998). Evaluation of amplified ribosomal DNA restriction analysis for identification of Acinetobacter genomic species. Syst Appl Microbiol 21, 33–39. Dijkshoorn, L., Nemec, A. & Seifert, H. (2007). An increasing threat in hospitals: multidrug-resistant Acinetobacter baumannii. Nat Rev Microbiol 5, 939–951. Fredricks, D. N. & Relman, D. A. (1998). Improved amplification of microbial DNA from blood cultures by removal of the PCR inhibitor sodium polyanetholesulfonate. J Clin Microbiol 36, 2810–2816. Gerner-Smidt, P., Tjernberg, I. & Ursing, J. (1991). Reliability of phenotypic tests for identification of Acinetobacter species. J Clin Microbiol 29, 277–282. Higgins, P. G., Wisplinghoff, H., Krut, O. & Seifert, H. (2007). A PCR- based method to differentiate between Acinetobacter baumannii and Acinetobacter genomic species 13TU. Clin Microbiol Infect 13, 1199– 1201. Higgins, P. G., Lehmann, M., Wisplinghoff, H. & Seifert, H. (2010). gyrB multiplex PCR to differentiate between Acinetobacter calcoaceticus and Acinetobacter genomic species 3. J Clin Microbiol 48, 4592– 4594. Huang, L. Y., Chen, T. L., Lu, P. L., Tsai, C. A., Cho, W. L., Chang, F. Y., Fung, C. P. & Siu, L. K. (2008). Dissemination of multidrug-resistant, class 1 integron-carrying Acinetobacter baumannii isolates in Taiwan. Clin Microbiol Infect 14, 1010–1019. Krawczyk, B., Lewandowski, K. & Kur, J. (2002). Comparative studies of the Acinetobacter genus and the species identification method based on the recA sequences. Mol Cell Probes 16, 1–11. Kuo, S. C., Lee, Y. T., Yang, S. P., Chiang, M. C., Lin, Y. T., Tseng, F. C., Chen, T. L. & Fung, C. P. (2013). Evaluation of the effect of appropriate antimicrobial therapy on mortality associated with Acinetobacter nosocomialis bacteraemia. Clin Microbiol Infect 19, 634–639. Lee, N. Y., Chang, T. C., Wu, C. J., Chang, C. M., Lee, H. C., Chen, P. L., Lee, C. C., Ko, N. Y. & Ko, W. C. (2010). Clinical manifestations, antimicrobial therapy, and prognostic factors of monomicrobial Acinetobacter baumannii complex bacteremia. J Infect 61, 219–227. Lee, Y.-T., Kuo, S.-C., Chiang, M.-C., Yang, S.-P., Chen, C.-P., Chen, T.-L. & Fung, C.-P. (2012a). Emergence of carbapenem-resistant http://jmm.sgmjournals.org Nemec, A., Musı́lek, M., Maixnerová, M., De Baere, T., van der Reijden, T. J., Vaneechoutte, M. & Dijkshoorn, L. (2009). Acinetobacter beijerinckii sp. nov. and Acinetobacter gyllenbergii sp. nov., haemolytic organisms isolated from humans. Int J Syst Evol Microbiol 59, 118–124. Nemec, A., Musı́lek, M., Sedo, O., De Baere, T., Maixnerová, M., van der Reijden, T. J., Zdráhal, Z., Vaneechoutte, M. & Dijkshoorn, L. (2010). Acinetobacter bereziniae sp. nov. and Acinetobacter guillouiae sp. nov., to accommodate Acinetobacter genomic species 10 and 11, respectively. Int J Syst Evol Microbiol 60, 896–903. Nemec, A., Krizova, L., Maixnerova, M., van der Reijden, T. J., Deschaght, P., Passet, V., Vaneechoutte, M., Brisse, S. & Dijkshoorn, L. (2011). Genotypic and phenotypic characterization of the Acinetobacter calcoaceticus–Acinetobacter baumannii complex with the proposal of Acinetobacter pittii sp. nov. (formerly Acinetobacter genomic species 3) and Acinetobacter nosocomialis sp. nov. (formerly Acinetobacter genomic species 13TU). Res Microbiol 162, 393–404. Peleg, A. Y., Seifert, H. & Paterson, D. L. (2008). Acinetobacter baumannii: emergence of a successful pathogen. Clin Microbiol Rev 21, 538–582. Šedo, O., Nemec, A., Křı́žová, L., Kačalová, M. & Zdráhal, Z. (2013). Improvement of MALDI-TOF MS profiling for the differentiation of species within the Acinetobacter calcoaceticus–Acinetobacter baumannii complex. Syst Appl Microbiol 36, 572–578. Turton, J. F., Woodford, N., Glover, J., Yarde, S., Kaufmann, M. E. & Pitt, T. L. (2006). Identification of Acinetobacter baumannii by detection of the blaOXA-51-like carbapenemase gene intrinsic to this species. J Clin Microbiol 44, 2974–2976. Vaneechoutte, M., Dijkshoorn, L., Tjernberg, I., Elaichouni, A., de Vos, P., Claeys, G. & Verschraegen, G. (1995). Identification of Acinetobacter genomic species by amplified ribosomal DNA restriction analysis. J Clin Microbiol 33, 11–15. Wisplinghoff, H., Paulus, T., Lugenheim, M., Stefanik, D., Higgins, P. G., Edmond, M. B., Wenzel, R. P. & Seifert, H. (2012). Nosocomial bloodstream infections due to Acinetobacter baumannii, Acinetobacter pittii and Acinetobacter nosocomialis in the United States. J Infect 64, 282–290. Downloaded from www.microbiologyresearch.org by IP: 88.99.165.207 On: Sun, 14 May 2017 02:03:14 1159