Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
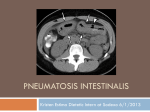
GI Grand Rounds Johanna Chan Gastroenterology Fellow Baylor College of Medicine 12/13/2012 No conflicts of interest No financial disclosures HPI • RFC: nausea, vomiting, abdominal pain • 61yo WM with HCV/EtOH cirrhosis, admitted with nausea and nonbloody emesis x 3 wks • Dull, diffuse abdominal pain, no radiation • Worse with eating and drinking • Early satiety • Poor PO intake x 3 weeks • No fever, chills, constipation, diarrhea, dysuria, edema Past Medical History • HCV genotype 3a ▫ Nonresponder to pegylated interferon and ribavirin in 2004 • HCV/EtOH cirrhosis, Child Class A • Bladder carcinoma s/p TURBT 1999 • BPH Medications • Omeprazole 20mg PO daily (recently prescribed at urgent care) • No other OTC medications, including NSAID or aspirin use Other history • Family history negative for GI malignancy, liver disease • Social history ▫ Current 1 pack/day smoker since teen years ▫ Prior h/o IVDA, none since 1990s ▫ Prior heavy EtOH since teen years, quit in 1980s Exam • • • • • • • T 98, BP 108/75, HR 78, RR 12, O2 sat 98% RA Gen: uncomfortable but nontoxic, NAD, AAOx4 HEENT: PERRL, EOMI, dry MM, OP clear Neck: supple, no LAD, flat neck veins CV: RRR no m/r/g Lungs: CTAB, no wheeze/crackles Abd: markedly distended, diffusely tender, no guarding, +BS, dull to percussion • Ext: WWP no c/c/e Labs 125 55 94 147 4.4 45 5.6 11.1 17.6 52.3 77% PMNs Total protein 7.4 Albumin 3.6 Total bili 3.1 ALT 109 AST 123 Alk phos 39 187 INR 1.1 PTT 32 MCV 99 Imaging Initial thoughts? Differential diagnosis? Next steps in management? • • • • A) NPO +/- NG tube decompression B) Broad-spectrum antibiotics C) Consult surgery D) Endoscopy (and timing?) Clinical course • • • • • • NPO, IV ceftriaxone and flagyl General surgery consult Negative blood and urine cultures Remained clinically well and nontoxic Symptoms improved Tolerated clear liquids for 2-3 days Clinical course • • • • Return of nausea and vomiting NG tube decompression: >3L nonbloody output Saline load test markedly positive Repeat KUB Endoscopy Gastric emphysema • Diagnosis: gastric emphysema due to gastric outlet obstruction • Pneumatosis intestinalis ▫ Gastric pneumatosis Gastric emphysema Emphysematous gastritis ▫ Pneumatosis coli Clinical questions • What is pneumatosis intestinalis (PI)? • Differential diagnosis of PI? • Management of PI? ▫ Indications for surgery? ▫ Role for endoscopy? • Relation to gastric outlet obstruction? What is pneumatosis intestinalis? • First described in 1754 by Du Vernoy • Presence of extraluminal bowel gas within bowel wall • Breakdown of mucosal and immunological barrier of intestine, especially in the setting of increased intraluminal pressure Galundiuk S et al. DCR. 1986; (29)5: 358-363. Heng Y et al. Am J of Gastroenterol. 1995; (90)10: 1747-1758. Koss LG. Arch Pathol. 1952; (53): 523-549. What is pneumatosis intestinalis? • • • • 0.03% in general population (autopsy series) Incidence rising with increasing CT use Most asymptomatic, incidentally detected Complications occur in up to 3% of patients ▫ Pneumoperitoneum, bowel obstruction, volvulus, intussusceptions, hemorrhage Galundiuk S et al. DCR. 1986; (29)5: 358-363. Heng Y et al. Am J of Gastroenterol. 1995; (90)10: 1747-1758. Differential diagnosis for PI • Idiopathic (rare) – 10-15% by review of 213 cases • Secondary ▫ ▫ ▫ ▫ Bowel necrosis Mucosal disruption Increased mucosal permeability Pulmonary disease Koss LG. Arch Pathol. 1952; (53): 523-549. Pear BL. Radiology. 1998; 207(1):13-19. DDx PI: Bowel necrosis • • • • • • Ischemia/infarction Necrotizing enterocolitis Neutropenic colitis Volvulus Sepsis In the stomach, emphysematous gastritis or ingestion of caustic agents DDx PI: Mucosal disruption • Over-distention (peptic ulcer, pyloric stenosis, annular pancreas, or distal obstruction) • Ulceration, erosions, trauma • Iatrogenic (feeding tubes, stent perforation, sclerotherapy, or surgical or endoscopic trauma) • Connective tissue disease: scleroderma, SLE • Medications that cause bowel distention: sortibol, lactulose DDx PI: Increased mucosal permeability • Mucosal erosions or defects in intestinal crypts (inflammatory bowel disease) • Immunocompromise (due to steroids, chemotherapy, radiation therapy, or AIDS) with defects in bowel wall lymphoid tissue • Acute graft vs. host disease DDx PI: Pulmonary disease • • • • • • Chronic obstructive pulmonary disease Asthma Cystic fibrosis Barotrauma After chest tube placement Increased intrathoracic pressure (retching, vomiting, PEEP) Management of PI • • • • • Exclude acute intra-abdominal emergency Antibiotics Elemental diet (for pneumatosis coli) High-flow oxygen or hyperbaric oxygen therapy Endoscopic therapy (particularly obstructive symptoms) *No randomized controlled data Indications for surgery • Clinical indications of bowel ischemia • Combination of PI and serum lactate >2 mmol/L associated with >80% mortality (Hawn et al) • Radiographic signs: ▫ Hepatic portal and portomesenteric venous gas ▫ Vascular distribution suggesting ischemia ▫ Additional abnormal bowel wall findings • Others: obstruction, ileus, toxic megacolon, severe collagen vascular disease Hawn MT et al. Am Surg. 2004; (70)1:19-23. Wayne E et al. J Gastrointest Surg 2010; 14:437. Role for endoscopy • Non-surgical cases • Diagnosis of underlying etiology • Gastric emphysema ▫ Submucosal “bubbles” with pale/bluish mucosa ▫ Deflate when biopsied ▫ Edema, erosions • Emphysematous gastritis ▫ Edematous, friable, ulceration with exudates ▫ Histology: fibrin thrombi, gas-forming organisms, bacterial infiltration, microabscesses Cordum NR et al. Am J Gastroenterol 1997; 92:692. Gastric emphysema in relation to gastric outlet obstruction • Well-reported in the pediatric literature • Most commonly due to pyloric stenosis ▫ Also duodenal stenosis, tumor, protracted vomiting • Mortality rate for gastric pneumatosis 41% in adults, 6% in children D’Cruz R et al. J Pediatr Surg 2008 ;43:2121-3. Taylor D et al. Int Pediatr 2000; 15:117-20. Lim RK et al. CMAJ 2010. 182(5): E227. Patient case follow-up • Esophagus, biopsy ▫ Gastric-type mucosa with mild chronic and focally acute inflammation ▫ Intestinal metaplasia • Stomach ulcer, biopsy ▫ Reactive gastropathy • Stomach, random biopsy ▫ Reactive gastropathy with focal chronic inflammation • Duodenum “mass”, biopsy ▫ Mild chronic focally active duodenitis, suggestive of Brunner’s gland hyperplasia References • Braumann C, Menenakas C, and Jacobi CA. “Pneumatosis intestinalis – a pitfall for surgeons?” Scandinavian Journal of Surgery. 2005; (94)1: 47-50. • Cordum NR, Dixon A, Campbell DR. Gastroduodenal pneumatosis: endoscopic and histologic findings. Am J Gastroenterol 1997; 92:692. • Galundiuk S and Fazio VW. “Pneumatosis cystoides intestinalis: a review of the literature.” Diseases of the Colon and Rectum. 1986; (29)5: 358-363. • Hawn MT, Canon CL, Lockhart ME, et al. “Serum lactic acid determines the outcomes of CT diagnosis of pneumatosis of the gastrointestinal tract.” Am Surg. 2004; (70)1:19-23. • Heng Y, Schuffler MD, Haggitt RC, and Rohrmann CA. “Pneumatosis intestinalis: a review.” American Journal of Gastroenterology. 1995; (90)10: 1747-1758. • Ho LM, Paulson EK, and Thompson WM. “Pneumatosis intestinalis in the adult: benign to life-threatening causes.” American Journal of Roentgenology. 2007; (188)6: 1604-1613. References (con’t) • Hoer J, Truong S, Virnich N, Fuzesi L, Schumpelick V. “Pneumatosis cystoides intestinalis: confirmation of diagnosis by endoscopic puncture a review of pathogenesis, associated disease and therapy and a new theory of cyst formation. Endoscopy. 1998; (30)9:793-799. • Koss LG. “Abdominal gas cysts (penumatosis cystoides intestinorum hominis): an analysis with a report of a case and a critical review of the literature.” Arch Pathol. 1952; (53): 523-549. • Pear BL. “Pneumatosis intestinalis: a review.” Radiology. 1998; 207(1):1319. • Pieterse AS, Leong AS, Rowland R. “The mucosal changes and pathogenesis of pneumatosis cystoides intestinalis. Hum Pathol 1985; 16:683. • Wayne E, Ough M, Wu A et al. “Management algorithm for pneumatosis intestinalis and portal venous gas: treatment and outcome of 88 consecutive cases.” J Gastrointest Surg 2010; 14:437. Thank you! Additional slides Histology • Histology: pseudocysts (no epithelium) with rim of histiocytes, multinuclear giant cells, lymphocytes, neutrophils, eosinophils, granulomas, fibrosis