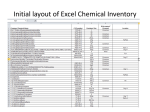
Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Innate immune system wikipedia , lookup
Crohn's disease wikipedia , lookup
Behçet's disease wikipedia , lookup
Transmission (medicine) wikipedia , lookup
African trypanosomiasis wikipedia , lookup
Sociality and disease transmission wikipedia , lookup
Immunosuppressive drug wikipedia , lookup
Autoimmunity wikipedia , lookup
Globalization and disease wikipedia , lookup
Inflammatory bowel disease wikipedia , lookup
Germ theory of disease wikipedia , lookup
Crohn’s Disease: A Complex Disease as described by Complexity Science Complexity Science arose out of the realization that the traditional reductionist approach to science failed to explain much of what we observe. Reductionism decomposes an entity into its component parts and studies the parts in an attempt to better explain the original whole. Taken to the extreme, everything can be reduced to quarks and vibrating strings. Much is lost by the reductionist approach. Complexity Science studies the interactions of the component parts (nodes) that make up a given entity and views them as an interacting complex system. This conceptual approach may be applied to all things occurring in different space and time scales. An important characteristic of complex systems is that they exhibit Emergent Behavior. Entities interact to form systems that display entirely new traits that may be totally unpredictable based on what is known about the components of the system. The new behavior traits may in turn define a new entity. An example would be the system formed when protons, neutrons and electrons interact to form a hydrogen atom, or when hydrogen and oxygen atoms interact to form water. New entities with new properties ‘emerge’ from the interactions of their component parts. Conceptualizing our Universe through the perspective of Complexity Theory is a powerful tool that may help us to understand and better manage complex problems. Complexity Science is the study of Complex Adaptive Systems (CAS). Key points need to be emphasized before continuing. 1. Entities can interact to form systems. 2. Systems increase in complexity as the number of interacting components increase. 3. As the complexity and energy of a system increases, the system may pass a threshold whereby it displays entirely new behavior patterns that cannot be predicted from knowledge about its component parts. 4. The original system may no longer be viewed as a system but is judged to be a new entity in its own right. 5. As a corollary, all single entities can be conceptualized as being a complex system composed of its component parts. 6. Complex Adaptive Systems display similarities with each other independent of the nature of their components. The components are referred to by the abstract term ‘nodes’. 7. Since the components of complex systems are themselves complex systems and since complex systems share similar characteristics, then similar patterns (fractals) can be observed amongst these systems acting on different scales of space and time. 8. Complexity Science is concerned with the similar patterns seen in Complex Adaptive Systems. Examples: a. Tires, pistons, gears, crankshafts etc. interact and display emergent behavior that we refer to as a single entity – the automobile. 1 b. Neurons in the brain interact and display emergent behavior that we refer to as the mind. The application of Complexity Theory to biological systems and medical diseases may provide insight into the complex processes involved. Crohn’s Disease (CD) is a complex process with behavior traits (phenotypes) that can be interpreted through the lens of Complexity Theory. Crohn’s Disease would be seen as the emergent properties that arise when the normal homeostatic balance of the involved Complex Adaptive System(s) are perturbed and shift away from the emergent states we normally call health. The human body is composed of many CAS all interacting with each. The emergent characteristics of all these lesser CAS define the global organism (human being). Health is defined as the optimum state that is obtained when all the CAS are working properly. An alteration in one of the component CAS may result in a disease state. The characteristics and phenotypes are the emergent traits of the altered systems. CAS may be composed of molecules, organelles, cells, organs etc. Components of a CAS interact within the same system (eg. cell to cell), horizontally with other CAS acting in the same biological level (macrophages with bacteria), or vertically with CAS acting at different levels ( molecules affecting cells, cells affecting organ function). Disruption at any level can spread to all levels such as a molecule that prolongs QT repolarization can result in arrythmias that bring about cessation of blood flow and death to the global organism. Complex Adaptive Systems existing in open energy states ‘far from equilibrium’ may display different emergent behaviors that vary with minor variations in initial conditions and/or interventions. Jason Bates describes three types of interventions that may occur. His explanations will be directly quoted rather than paraphrased.(1) The significance for biological systems is obvious. “Most minor perturbations that a healthy individual experiences in daily life, such as receiving a bruise or catching a cold, are transient experiences against which the body is able to mount a response that eventually returns things back to normal. By contrast, a general characteristic of complex diseases, apart from their resistance to elucidations, is that they tend to be chronic (e.g. asthma, hypertension); the homeostatic balance of health seems to become disrupted in a way that is resistant to treatment. In light of the foregoing, this suggests that minor ailments represent a small shift away from dynamic equilibrium, while in chronic disease a biological network is placed in a permanently altered state. We identify three distinct mechanisms by which the state of a dynamic network can be permanently altered. 1. Altered Network Structure: The most obvious way of changing network behavior is to damage it, either by loss of nodes or breakage of links. The causative agent could be either some external influence or simply degeneration from within. Treatment of a damaged network is presumably a matter of locating and repairing the damage. 2. Persistent Insult: A living system requires input from the environment, either continuously (e.g. oxygen) or periodically (food), but is also subject to noxious inputs. A noxious input applied briefly (a glass of whiskey) may upset the 2 homeostatic balance transiently, but this balance is expected to return to normal in time. By contrast, if the noxious input is applied persistently, an ongoing disruption of homeostasis is expected. The progressive granulomatous lesions caused by particles of silica in the lung may be such an example. Treatment of disease caused by a persistent insult is obviously a matter of finding and removing the insult. 3. Entrapment in a local energy minimum: The third way of altering network behavior is the most subtle and arises because dynamic networks may have more than one dynamically stable state defined by the pattern of activities of its nodes and links. Transition between different stable states may be elicited by suitable external stimuli. Furthermore, once such a state transition has been achieved, removal of the stimulus will not necessarily reverse the situation. Chronic diseases might then be the result of an environmental insult that moves the network from its state of health to one of permanent pathology. This would occur with no change in network structure, so there would be nothing to repair. Furthermore, searching for the initiating event, which could be long gone at the time of diagnosis, would also be futile. The enigmatic nature of a pathology of this kind would make its correction especially problematic.” Although the complexity paradigm can be used to explain any disease process, Crohn’s Disease is an interesting example because of the controversy surrounding questions about its etiology. This chronic inflammatory bowel syndrome was initially thought to be an infectious disease most probably caused by either Mycobacterium tuberculosis or another mycobacterium. The technology of the time could not identify a bacterial cause so Crohn, Oppenheimer and Ginsburg suggested that debate about its etiology be left open and that it be studied as a disease in its own right. Assumptions about the disease shifted. Some hypothesized that it was fundamentally a psychiatric disorder followed by the hypothesis that it was an autoimmune disorder. Both hypotheses have been largely abandoned due to lack of evidence for an underlying psychiatric disorder and failure to identify a selfantigen for the autoimmune hypothesis. Currently the most widely quoted hypothesis is in essence descriptive: CD is a chronic inflammatory disorder occurring in genetically susceptible hosts and triggered by an unknown environmental agent possibly coming from the normal gut flora. This description is accurate but says nothing about etiology. Clearly, dysregulated immune/inflammatory pathways are involved as they are in all chronic inflammatory conditions and the Genome Wide Association Study has identified over 40 genes that are risk factors for getting CD. However, why patients develop the disease after 20 to 30 years of health is not addressed. The other theory that is getting traction is that CD is caused by a chronic infection with Mycobacterium avium paratuberculosis (MAP). MAP is thought by some to be the environmental agent mentioned in the Immune Dysregulation hypothesis. Could interpreting CD through the Complexity Theory paradigm help in elucidating the cause? The answer is both a Yes and a No. The Immune Dysregulation hypothesis 3 suggests that an unknown agent shifts the Complex Adaptive Systems (primarily the mucosal immune system) such that it display emergent behaviors consistent with the pathologic phenotype of the disease. The altered network could result from perturbations resulting from the three mechanisms described by Bates: 1) altered network structure, 2) persistent intervention or 3)shifting the network to an alternative attractor basin. Chronic intracellular infections of macrophages and Dendritic Cells by pathogenic mycobacteria (MAP, M.tuberculosis and M. leprae) intervene in biological CAS by all three mechanisms. MAP alters network architecture by interfering with phagosome/lysosome fusion at the intracellular level with subsequent effects on mucosal barrier function, ulcerations, granuloma formation etc. Persistent intracellular infections of Antigen Presenting Cells continually alter the immune signaling pathways leading to both an immune deficiency state and excessive inflammation, and pathogenic mycobacteria may alter the Complex Adaptive Immune System so that it shifts to another semi-stable energy state (cycles around another attractor basin) and displays the emergent behavior of a chronic inflammatory disease. Interpreting CD through the Complexity theory paradigm does not by itself settle the controversy surrounding the etiologic theories. However, describing the issues in Complexity terminology does emphasize just how closely the two theories are to each other. The recent publication from Melbourne, Australia associating MAP with CD by PCR technology contributes to the mounting evidence that MAP is associated with CD. (2) And the joint effort from the labs at the University of Central Florida, University of Wisconsin and the Centers for Disease Control whereby they cultured MAP from the blood confirms Naser’s earlier work showing that MAP is an invasive mycobacterium when it is associated with Crohn’s disease.(3) Whether or not MAP is a causative agent of CD is now more a matter for political and sociological discussion. Irrespective of how the debate goes, it would be wise to devote our energies to eradicating MAP from those CD patients who harbor it. How can the Complexity paradigm improve therapeutic strategies? A workshop on “Causality and Influence Networks in Complex Systems” held in Mt. Tamborine, Australia attempted to address this issue although their intent was to find ways to identify and manipulate key nodes in complex systems involved in other disciplines. (4) The three previously mentioned mechanisms serve as a framework for discussing potential therapeutic interventions. #1. Network Structure: Biologic complex adaptive systems exhibit fractal geometry. Smaller CAS lay within larger CAS. Manipulating key molecular nodes may affect the phenotypes of the larger systems. CD is defined by the dysregulated immune responses associated with inappropriate, ineffective cytokine profiles. Altering molecular components such as key inflammatory cytokines may induce emergent traits that alter the global phenotype. As an example, corticosteroids down-regulate the production of excessive, inappropriate inflammatory cytokines thus partially suppressing the destructive inflammatory state. Unfortunately, corticosteroids don’t restore the whole system to optimal balance as evidenced by the deleterious effects on immunity, energy metabolism, bone demineralization etc. 4 #2. Persistent Stimulus: If Mycobacterium avium paratuberculosis or other persistent infectious microbes are causative agents of the CD syndrome then treatment should be directed at removing them. There removal conceivably will allow the systems to return to their proper attractor basins. The optimum therapies against infectious agents are a combination of antibiotics and immune enhancement. #3. Alternative Attractor Basins: Assuming that the initiating triggering agent has been removed, restoring the systems so that their emergent traits display healthy homeostasis is synonymous with cure. How to achieve this end defines the problem. The glucocorticoid (GC) example may be instructive. GC and the glucocorticoid receptor (GR) sit atop a cascade of intracellular, interconnecting pathways that influence signaling and gene response networks. The favorable anti-inflammatory steroid effects potentially may be separated from the less favorable immune suppressive and metabolic responses. (5) The existence of 46 steroid receptors in the human genome suggests a fine-tuning to the steroid story that is poorly understood. Current research with androstene analogues of the steroid nucleus show that the beneficial anti-inflammatory responses can be achieved without compromising immunity or disrupting energy and bone metabolism.(6) These steroid hormones may intervene in dysregulated immune states to restore the proper homeostatic balance synonymous with health. 1. Bates, Jason. Toward a Nonlinear Network Theory of Complex Disease. New England Complex Systems Institute. International Conference on Complex Systems, 2006; (ICCS 2006). 2. Kirkwood CD, Wagner J, Boniface K, Vaughan J, Michalski WP, Catto-Smith AG, Cameron DJ, Bishop RF. Mycobacterium avium subspecies paratuberculosis in children with early-onset Crohn’s disease. Inflammatory bowel diseases Epub 21 May 2009. 3. accepted for publication – (personal communication) 4. Understanding and Influencing Systems with Complex Causal and Influence Networks Workshop. Mt. Tamborine, Queensland, Australia. July 7-10, 2009. 5. Turk R, Cidlowski JA. Anti-inflammatory Action of Glucocorticoids – New Mechanisms for Old Drugs. N Engl J Med 2005;353:1711-23. 6. Reading C, Dowding C, Schramm B, Garsd A, Onizuka-Hanada N, Stickney D, Frincke J. Improvement in immune parameters and human immunodeficiency virus-1 viral response in individuals treated with 16alpha-bromoepiandrosterone (HE2000). Cllin Microbiol Infect 2006;12:1082-1088. 5