Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Rett syndrome wikipedia , lookup
Alcohol withdrawal syndrome wikipedia , lookup
Serotonin syndrome wikipedia , lookup
Williams syndrome wikipedia , lookup
Lesch–Nyhan syndrome wikipedia , lookup
Marfan syndrome wikipedia , lookup
Guillain–Barré syndrome wikipedia , lookup
Down syndrome wikipedia , lookup
Asperger syndrome wikipedia , lookup
Management of multiple sclerosis wikipedia , lookup
Wernicke–Korsakoff syndrome wikipedia , lookup
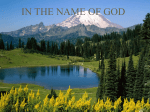
PRESCRIBING IN PRACTICE ■ The treatment challenges of restless legs syndrome SANJAY GANGADHARAN, LAUREN PERKINS, ANNA SAUERBIER AND K RAY CHAUDHURI Restless legs syndrome is a common disorder characterised by the uncontrollable urge to move the legs, particularly during inactivity or rest. Although the condition is common and has a high impact on quality of life, diagnosis and appropriate management remain a challenge in the primary care setting. R estless legs syndrome (RLS), also known as Willis-Ekbom disease, is a common sensorimotor disorder characterised by an uncontrollable urge to move certain parts of the body, in particular the lower limbs. It is initiated or aggravated during inactivity or rest and is mostly worse at night time. The condition spans several specialities including neurology (movement disorders), sleep disorders and neuropsychiatry, and patients may also present to haematology, nephrology or rheumatology. Thomas Willis first described RLS in the 17th century, although references to RLS exist in ancient Chinese and Greek literature as well. Karl Ekbom first used the term ‘restless legs syndrome’ in 1945.1,2 He noted the familial nature of RLS and its association with anaemia and pregnancy, the link with vitamin B12 deficiency (related to stomach surgery)2 and the association with pain. This is why RLS is also called Willis-Ekbom disease. More recently, the International RLS Study Group (IRLSSG) validated the IRLSSG criteria3 for diagnosing RLS and devised the IRLSSG rating scale (mild, moderate, severe, very severe), which is widely used in clinical trials.4 prescriber.co.uk Country No. of patients No. of practices Unadjusted prevalence (%) Adjusted prevalence (%) Denmark 1397 9 2.9 3.5 Germany 1360 5 2.1 2.4 Ireland 2628 19 3.2 4.6 Netherlands 2121 15 5.0 6.0 Spain 2047 10 3.9 4.6 UK 1011 4 2.8 4.6 Table 1. Prevalence of restless legs syndrome in primary care in western Europe5 Epidemiology A primary care study from Allen et al. investigated the prevalence rates of RLS across six countries in western Europe. Within the population of 10,564 patients screened, the prevalence of RLS in people of European descent ranged from 2.4–6 per cent (see Table 1).5 RLS affects about 2 per cent of school-aged children, 3 per cent of 30-year-olds and 20 per cent of people aged 80 and older.5-7 Women are more affected than men in a roughly 2:1 ratio, with nearly one in three pregnant women experiencing RLS during their third trimester.6 Multiple studies on the prevalence of RLS in non-European ethnic groups report much lower prevalence rates, ranging from 0.1–3.3 per cent, suggesting genetic, environmental or sociocultural factors in expressivity or reporting.4,8,9 However, a recent Korean and Argentinian study has reported a higher prevalence rate of RLS using validated methodology; the prevalence of RLS in Asian and Latin American populations therefore needs further research. RLS types RLS can be categorised into two types: either primary (idiopathic) or secondary. Prescriber September 2016 ❚ 15 Restless legs syndrome Primary RLS is the most common, with the cause known to be sporadic or, in a minority of cases, hereditary. Familial aggregation of RLS is well documented and the heritability is 54–83 per cent. Concordance among monozygotic twins is 50–80 per cent with variable symptom expression.10 Secondary RLS, however, is related to an underlying health condition and can be aggravated by certain medications. At least 20 medical conditions associated with RLS have been reported in medical literature. The most common medical conditions associated with RLS include renal failure/uraemia, depression and Parkinson’s disease (see Table 2). 11 Vitamin B12/folate deficiency is also a cause of secondary RLS and levels should be checked regularly in clinical practice. Diagnosis and assessment in primary care The IRLSSG updated the RLS diagnostic criteria in 2014.12 Diagnosis of RLS can be made if all of the following five essential criteria are met: • An urge to move the legs usually but not always accompanied by, or felt to be caused by, uncomfortable and unpleasant sensations in the legs • The urge to move the legs and any accompanying unpleasant sensations begin or worsen during periods of rest or inactivity, such as lying down or sitting • The urge to move the legs and any accompanying unpleasant sensations are partially or totally relieved by movement, such as walking or stretching, at least as long as the activity continues • The urge to move the legs and any accompanying unpleasant sensations during rest or inactivity only occur in the evening or night, or are worse in the evening or night than during the day. • The occurrence of the above features is not solely accounted for as symptoms primary to another medical or a behavioural condition, eg myalgia, venous stasis, leg oedema, arthritis, leg cramps, positional discomfort, habitual foot tapping. In fact, an even quicker way to screen for RLS in clinical practice is to use the following validated single question developed by Ferri et al: “When you try to relax in the evening or sleep at night, do you prescriber.co.uk l PRESCRIBING IN PRACTICE ■ Causes RLS group n=3319 (% patients) Control group n=3319 (% patients) Odds ratio* (95% CI) Depression 512 (15.4) 420 (12.7) 1.24 (1.07–1.44) Anxiety 275 (8.3) 241 (7.3) 1.09 (0.91–1.32) Diabetes mellitus 140 (4.2) 206 (6.2) 0.66 (0.52–0.82) Iron deficiency anaemia 127 (3.8) 159 (4.8) 0.77 (0.60–0.98) Hypothyroidism 55 (1.7) 59 (1.8) 0.91 (0.63–1.32) Pregnancy 42 (1.3) 51 (1.5) 0.84 (0.53–1.31) Parkinsonism 32 (1.0) 21 (0.6) 1.49 (0.85–2.61) Rheumatoid arthritis 27 (0.8) 30 (0.9) 0.95 (0.56–1.60) End-stage renal disease 17 (0.5) 4 (0.1) 4.76 (1.59–14.3) Fibromyalgia 10 (0.3) 8 (0.2) 1.26 (0.47–3.40) *Odds ratio represents the odds that an outcome will occur given a particular exposure Table 2. Reported causes and determinants of restless legs syndrome (RLS) in a UK study: occurrence in the two years before the index date (the date of RLS diagnosis in the RLS group)11 ever have unpleasant, restless feelings in your legs that can be relieved by walking or movement?” This question has 100 per cent sensitivity and 96.8 per cent specificity for the diagnosis of RLS.13 Management of RLS Lifestyle factors that have been shown to precipitate RLS, and therefore those to be avoided, include: a high caffeine intake,14 excessive alcohol in particular at night time,15 severe stress, shift work, poor sleep hygiene and intense physical activity near bedtime. Sleep hygiene (including regular bedtimes, a comfortable sleeping environment as well as adequate bedding, etc) and lifestyle changes should always be considered and tested before any pharmacological therapy is prescribed. An acute worsening of symptoms can be managed with hot or cold massage, physical activity such as stretching or walking, mental distraction and relaxation exercises.16 A key point to consider in the diagnosis of RLS is that the presence of RLS symptoms does not fully translate to a clinically significant disorder that warrants treatment; this was demonstrated in the REST study.17 It is the responsibility of the clinician to determine the RLS severity and subsequently advise on the correct course of treatment. The IRLSSG rating scale can be used to establish the severity of RLS, and subsequently the need for treatment12 as well as to monitor disease progression. A score of 1–10 represents mild, 11–20 moderate, 21–30 severe and 31–40 very severe disease. Although sudden remission of symptoms has been described; in most cases, primary RLS typically runs a chronic course with worsening of symptoms over time. However, in secondary RLS, treatment of the underlying pathology (such as systemic iron deficiency) can help achieve remission of symptoms.18 Only 10–15 per cent of patients with RLS have symptoms severe enough to be treated with medications.17. Dopamine agonists are the first-line treatment for RLS. In the UK, immediate-release (pramipexole and ropinirole) and transdermal (rotigotine) preparations are the only dopamine agonists licensed for treatment of RLS (see Table 3). However, prolonged-release pramipexole and ropinirole are usually administered as a single evening dose, whereas transdermal rotigotine patches have the advantage of a sustained release throughout the day. Prescriber September 2016 ❚ 17 Restless legs syndrome l PRESCRIBING IN PRACTICE ■ Diagnosis of RLS (IRLSSG criteria) Single screening question Investigations • Physical examination •B lood test: iron studies (serum ferritin), full blood count, serum vitamin B12/folic acid, serum glucose and HbA1c, urea and electrolytes, serum creatinine, thyroid function test (optional) • Exclude co-morbidities, pregnancy and related medications • Severe RLS, insomnia and periodic limb movements: consider sleep studies Establish the severity of RLS IRLSSG rating scale (mild, moderate, severe, very severe) Does the adult patient have primary or secondary RLS? Are their symptoms painful? Secondary RLS Primary RLS Mild to moderate: lifestyle changes, eg sleep hygiene Moderate to very severe: treatment needed (see Table 3) Painful RLS and neuropathic pain: alpha 2-delta ligands (pregabalin, gabapentin) and opioids Treatment of the underlying pathophysiology Figure 1. Management pathway for restless legs syndrome (RLS) following a diagnosis using the International RLS Study Group (IRLSSG) criteria Second-line treatment options for RLS include gabapentin, pregabalin, clonazepam and opiates (see Table 3); their use is usually guided by neurologists. Trenkwalder et al. demonstrated that prolonged-release oxycodone and naloxone (Targinact) was efficacious for short-term management of severe RLS in subjects in whom first-line therapy had failed.19 This drug combination is now licensed in the UK for patients suffering from RLS for at least six months, and in whom dopaminergic treatment has already failed. It would be most suitable for those patients with a painful variant of RLS who have not responded well to first-line therapies. Because of the high rates of augmentation (see below), levodopa is not typically recommended for daily treatment prescriber.co.uk in the UK. In individual cases, it might be useful as a rescue medication for patients with predictable RLS. Complexities of RLS treatment Augmentation is characterised by an overall increase in symptom severity while on treatment. This is mostly seen in patients treated with levodopa or dopamine agonists (highest rates with pramipexole and lowest with rotigotine).20 The predictors for augmentation include: low plasma ferritin levels, longer treatment duration, possibly a preceding tolerance to medication and previous episodes of augmentation.20 Early morning rebound is the reappearance of symptoms of RLS when the medication effects wear off. It is common in drugs with a shorter half-life, such as levodopa. Here, the practitioner should consider altering the time of treatment administration, increasing the drug dose or trying an alternative drug. Burden of RLS Moderate or severe RLS has a high impact on the health and wellbeing of individuals affected, their partners and the community. Recent studies have suggested that patients also suffer from nonmotor symptoms (NMS) such as depression, anxiety and sleep disturbances. These NMS are known to impact upon patients’ health-related quality of life (HRQoL), and therefore Professor Chaudhuri’s team are leading a project to further investigate these NMS, including the development of a questionnaire. The biopsychosocial and economic Prescriber September 2016 ❚ 19 ■ PRESCRIBING IN PRACTICE l Restless legs syndrome Medication Starting dose–maximal recommended dose (daily) Time to full effect of the therapeutic dose Half-life Side-effects Pramipexole 0.088mg–0.54mg (base) or 0.125mg–0.75mg (salt) At first dose 8–12 hours Augmentation, impulse control disorder, hypotension, dizziness, headache, somnolence Ropinirole 0.25mg–4mg 4–10 days 6 hours Same as pramipexole Rotigotine transdermal patch 1–3mg/24 hours 1 week 5–7 hours Skin irritation, low risk of augmentation, nausea, hypotension, dizziness, headache, nasal congestion Targinact (prolongedrelease oxycodone/ naloxone) 5mg/2.5mg– 60mg/30mg 1 week 1 hour Headache, somnolence, nausea, fatigue Levodopa 50mg–200mg At first dose 1.5–2 hours High rates of augmentation and loss of efficacy with rebound phenomena Pregabalin 25–300mg 3–6 days 10 hours Sleepiness, dizziness, headache and fluid retention Gabapentin 300mg–2700mg 3–6 days 5–7 hours Sleepiness, dizziness and fluid retention Carbamazepine 100mg–600mg 1–2 weeks 16–24 hours Fatigue, urticaria, vomiting, nausea, dizziness and leucopenia Clonazepam 0.5mg–2.0mg At first dose, effect mainly on sleep 30–40 hours High risk of sleepiness, dizziness, morning drug handover Tramadol 50mg–100mg At first dose 6 hours Dizziness, nausea, sweating, constipation and fatigue Oxycodone 2.5mg–25mg At first dose 4–5 hours Constipation, nausea and vomiting Ferrous sulfate 200mg three-times daily 2–3 weeks Licensed treatments Unlicensed treatments Constipation Table 3. Pharmacological treatment options for restless legs syndrome: recommended dosages, pharmacokinetics and possible side-effects. Adapted from Klingelhoefer et al.18 burden of RLS symptoms has also been shown to have a negative impact on the sufferer’s HRQoL.4 Poor HRQoL leads to decreased productivity, increased absenteeism and unemployment.21-23 Conclusion RLS is a common sensorimotor disorder with well-defined diagnostic criteria including a validated single screening question, as well as full IRLSSG criteria. Early diagnosis, accurate assessment of severity and appropriate management of the symptoms of RLS in the primary care setting remains 20 ❚ Prescriber September 2016 a challenge, due to the complexity and heterogeneity in the disease presentation. References 1. Ekbom KA. Asthenia crurum paraesthetica (irritable legs). Acta Med Scand 1944;118:197–207. 2. Ekbom KA. Restless legs syndrome. Neurology 1960;10:868–73. 3. Walter AS. Towards a better definition of restless legs syndrome. The International Restless Legs Syndrome Study Group (IRLSSG). Mov Disord 1995;5:634–42. 4. Allen RP, et al. Restless legs syndrome: diagnostic criteria, special considerations and epidemiology. Sleep Med 2003;4:101–19. 5. Allen RP, et al. Physician-diagnosed restless legs syndrome in a large sample of primary medical care patients in western Europe: prevalence and characteristics. Sleep Med 2010;1:31–7. 6. Berger K, et al. Sex and the risk of restless legs syndrome in the general population. Arch Intern Med 2004;164:196–202. 7. Picchietti D, et al. Restless legs syndrome: prevalence and impact in children and adolescents – the peds REST study. Paediatrics 2007;120:253–66. 8. Chen NH, et al. The prevalence of restless legs syndrome in Taiwanese adults. Psych Clin Neurosci 2010;64:170–8. prescriber.co.uk Restless legs syndrome 9. Shi Y, et al. The prevalence and risk factors for restless legs syndrome among Chinese adults in a rural community of Shanghai in China. PLoS One 2015;10:e0121215. 10. Winkelmann J, et al. Genetics of restless legs syndrome: state-of-the-art and future directions. Mov Disord 2007;22:449–58. 11. Van de Vijver D, et al. Epidemiology of restless legs syndrome as diagnosed in UK primary care. Sleep J 2004;5:435–40. 12. Allen RP, et al. Restless legs syndrome/ Willis-Ekbom disease diagnostic criteria: Updated International Restless Legs Syndrome Study Group (IRLSSG) consensus criteria. Sleep Med 2014;5:860–73. 13. Ferri R, et al. A single question for the rapid screening of RLS in clinical practice. Eur J Neurol 2007;14:1016–21. 14. Lutz EG. Restless legs, anxiety and caffeinism. J Clin Psychiatry 1978;39:693–8. 15. Aldrich MS, Shipley JE. Alcohol use and periodic limb movements of sleep. Alcohol Clin Exp Res 1993;17:192–6. 16. Russell M. Massage therapy and restless legs syndrome. J Bodywork Mov Ther 2007;11:146–50. 17. Hening W, et al. Impact, diagnosis and treatment of restless legs syndrome (RLS) in a primary care population: the REST (RLS epidemiology, symptoms, and treatment) primary care study. Sleep Med 2004;5:237–46. 18. Klingelhoefer L, et al. A current review of treatment strategies for restless legs syndrome (Willis-Ekbom disease). Clin Med 2014;14:520–4. 19. Trenkwalder C, et al. Prolonged release oxycodone-naloxone for treatment of severe restless legs syndrome after failure of previous treatment: a double-blind, randomised, placebo-controlled trial with an open-label extension. Lancet Neurol 2013;12:1141–50. 20. Garcia-Borreguero D, Williams AM. Dopaminergic augmentation of restless legs syndrome. Sleep Med Rev 2010;14:339–46. 21. Abetz L, et al. The reliability, validity and responsiveness of the international restless legs syndrome study group rating scale and subscales in a clinical-trial setting. Sleep Med 2006;7:340–9. 22. Salas RE, Kwan AB. The real burden of restless legs syndrome: clinical and economic outcomes. Am J Manag Care 2012;18:207–12. 23. Kaloo A, et al. The impact of RLS/WED on Quality of Life. Eur Neurol Rev 2013;8:97–104. Declaration of interests Sanjay Gangadharan, Lauren Perkins and Anna Sauerbier have no conflicts of interest. Professor Chaudhury has previously received an honorarium from Mundipharma. prescriber.co.uk Sanjay Gangadharan is an advanced trainee in the Department of Geriatric Medicine, John Hunter Hospital, University of Newcastle, Australia; Lauren Perkins is a senior research co-ordinator, King’s College Hospital NHS Foundation Trust; Anna Sauerbier is a clinical research fellow and K Ray l PRESCRIBING IN PRACTICE ■ Chaudhuri is professor of movement disorders at the National Parkinson Foundation International Centre of Excellence, King’s College London; and the Department of Basic and Clinical Neuroscience, The Maurice Wohl Clinical Neuroscience Institute, King’s College London