Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
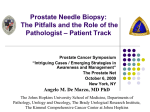
european urology 52 (2007) 1309–1322 available at www.sciencedirect.com journal homepage: www.europeanurology.com Review – Prostate Cancer Extended and Saturation Prostatic Biopsy in the Diagnosis and Characterisation of Prostate Cancer: A Critical Analysis of the Literature Vincenzo Scattoni a,*, Alexandre Zlotta b, Rodolfo Montironi c, Claude Schulman d, Patrizio Rigatti a, Francesco Montorsi a a Department of Urology, University Vita-Salute, Scientific Institute San Raffaele, Milan, Italy Division of Urology, Mount Sinai and Princess Margaret Hospitals, University of Toronto, Toronto, Ontario, Canada c Section of Pathological Anatomy, United Hospitals, Marche Polytechnic University, Ancona, Italy d Department of Urology, Erasme Hospital, University Clinics of Brussels, Brussels, Belgium b Article info Abstract Article history: Accepted August 3, 2007 Published online ahead of print on August 17, 2007 Objective: To review and critically analyse all the recent literature on the detection and characterisation of prostate cancer by means of extended and saturation protocols. Methods: A systematic review of the literature was performed by searching MedLine from January 1995 to April 2007. Electronic searches were limited to the English language, and the key words ‘‘prostate cancer,’’ ‘‘diagnosis,’’ ‘‘transrectal ultrasound (TRUS),’’ ‘‘prostate biopsy,’’ and ‘‘prognosis’’ were used. Results: The prostate biopsy technique has changed significantly since the original Hodge sextant biopsy protocol. Several types of local anaesthesia are now available, but periprostatic nerve block (PPNB) has proved to be the most effective method to reduce pain during TRUS biopsy. It remains controversial whether PPNB should be associated with other medications. The optimal extended protocol (sextant template with at least four additional cores) should include six standard sextant biopsies, with additional biopsies (up to 12 cores) taken more laterally (anterior horn) to the base and medially to the apex. Repeat biopsies should be based on saturation biopsies (number of cores 20) and should include the transition zone, especially in a patient with an initial negative biopsy. As a means of increasing accuracy of prostatic biopsy and reducing unnecessary prostate biopsy, colour and power Doppler imaging, with or without contrast enhancement, and elastography now can be successfully adopted, but their routine use is still controversial. Conclusion: Extended and saturation biopsy schemes should be performed at first and repeat biopsy, respectively. The widespread use of local anaesthesia makes the procedures more comfortable. Keywords: Diagnosis Prognosis Prostate biopsy Prostatic neoplasms Transrectal ultrasound Please visit www.eu-acme.org/ europeanurology to read and answer questions on-line. The EU-ACME credits will then be attributed automatically. # 2007 European Association of Urology. Published by Elsevier B.V. All rights reserved. * Corresponding author. Department of Urology, University Vita-Salute, Scientific Institute H San Raffaele, Via Olgettina 60, 20132 Milan, Italy. Tel. +39 02 2643 2311; Fax: +39 02 2643 2735. E-mail address: [email protected] (V. Scattoni). 0302-2838/$ – see back matter # 2007 European Association of Urology. Published by Elsevier B.V. All rights reserved. doi:10.1016/j.eururo.2007.08.006 1310 1. european urology 52 (2007) 1309–1322 Introduction Widespread use of serum prostate-specific antigen (PSA) has certainly increased prostate cancer detection and resulted in considerable stage migration [1]. Such results would not have been achieved without the contemporary refinements of the technique of prostate biopsy (PBx). After the initial introduction of the sextant PBx technique proposed by Hodge, little refinement of the technique was made until Stamey [2] suggested directing the biopsies more laterally. It is now recognised that even lateral sextant biopsies can miss up to 30% of cancers because more extended prostatic biopsy (EPBx) schemes result in higher cancer detection rates [3–7]. As defined by the National Comprehensive Cancer Network, an EPBx is essentially a sextant template with at least four additional cores from the lateral peripheral zone as well as biopsies directed to lesions found on palpation or imaging. At present, little controversy exists in the urologic community regarding the usefulness of EPBx compared with sextant biopsy in increasing the detection rate of prostate cancer. Data from both academic and community practices demonstrate a high cancer detection rate (42–44%) with a 12-core biopsy template in patients undergoing initial biopsy [8]. Nevertheless, prostate cancer detection is still an area currently fraught with many unanswered questions and significant controversy. Even if several different EPBx techniques have been recently presented, the optimal protocol needed to identify all patients with prostate cancer at the earliest stage possible for optimal treatment, outcome, and survival is still not known. Moreover, the significance of a Fig. 1 – Drawing shows the sites of injection of lidocaine to perform a periprostatic nerve block (PPNB). PBx has changed over the years. Today, a PBx is not only a method to diagnose prostate cancer, but it has become an informative method for an accurate morphologic characterisation of prostate cancer, including its volume and Gleason score. We have reviewed the available literature on this topic and compared the efficacy and safety of the different schemes with respect to the number of cores and sampling locations. A systematic review of the literature was performed by searching MedLine from January 1995 to April 2007. Electronic searches were limited to the English language, and the key words ‘‘prostate cancer,’’ ‘‘diagnosis,’’ ‘‘transrectal ultrasound (TRUS),’’ ‘‘prostate biopsy,’’ and ‘‘prognosis’’ were used. 2. Anaesthesia during transrectal prostate biopsy and antibiotic prophylaxis 2.1. Anaesthesia during TRUS Anaesthesia during TRUS PBx is now considered the gold standard; it is recommended by recently published guidelines, and we are close to the point in which absence of anaesthesia would be considered malpractice [9]. Intrarectal local anaesthesia (IRLA) with lidocaine gel (2%) has had controversial results compared with placebo [10,11]. In a recent meta-analysis [12], five studies involving 466 patients and comparing IRLA with placebo showed that IRLA was associated with pain reduction, but the effect size was not statistically significant. Moreover, in randomised studies, IRLA was reported to be inferior to periprostatic nerve block (PPNB) with lidocaine injection [13–20]. In several articles, it has been shown that PPNB was superior to IRLA in reducing pain during PBx in different randomised studies (Table 1). Even if the superiority of PPNB versus IRLA is evident, it remains unclear which dosage and PPNB technique should be used. As for the site and amount of anaesthetic infiltration, a study using a placebo and six groups of escalating doses of 1% lidocaine (2.5, 5, and 10 ml) infiltration revealed that the best pain relief was obtained with 10 ml lidocaine infiltrated solely at the neurovascular bundle region (single site) or to the neurovascular bundle and apical regions (double site). Therefore, the authors recommended singlesite, 10-ml infiltration in the region of the neurovascular bundle [21]. Various infiltration sites have been described, including the apex only [22,23], bilateral neurovascular bundle regions only (defined variously as Table 1 – Randomised studies comparing PPNB and IRLA Authors No. of patients Dose and type of drug No. of core biopsies Results * 23 (PPNB) vs. 27 (GEL) 20 ml lidocaine 1% (10 ml to junction of seminal vesicle and prostate + 5 ml into genitourinary diaphragm + 5 ml between rectal wall and prostate) vs. 10 ml 2% lidocaine jelly intrarectally 8 up to 15 (mean 12) Overall pain : 0.5 vs. 4.2 ( p < 0.0001); biopsy pain 0.5 vs. 4.2 ( p < 0.0001) * Pain evaluation: 10-point VAS: insertion of TRUS probe, anaesthetic instillation, biopsy, and overall pain procedure Adamakis et al. [14] 40 (sonographic gel) vs. 78 (GEL) vs. 80 (PPNB) 10 ml sonographic gel intrarectally vs. 10 ml 5% prilocaine-lidocaine cream (EMLA1) vs. 10 ml 2% lidocaine to junction of seminal vesicle and prostate 10-core biopsies Mean pain*: 5.1 vs. 4.8 vs. 2.5; statistically significant difference in group 3 and 1 ( p < 0.001) and in group 3 and 2 ( p < 0.001); no statistically significant difference in groups 1 and 2 ( p = 0.18) * Pain evaluation: 11-point VAS biopsy pain Lynn et al. [15] 30 (PPNB) vs. 27 (GEL) vs. 14 (gel-placebo) vs. 15 (placebo-injection) 10 ml 1% lignocaine periprostatic nerve plexus injection vs. 11 ml 2% lignocaine gel intrarectally vs. 10 ml gel-placebo rectally vs. 10 ml normal saline periprostatic nerve plexus injection Sextant prostate biopsies Mean pain*: 0.5 vs. 2.7 vs. 4.8 vs. 4.3; statistically significant difference in only group 1 ( p < 0.001) * Pain evaluation: 10 point-VAS Song et al. [16] 30 (GEL) vs. 30 (PPNB) vs. 30 (injection-placebo) 20 ml 2% lidocaine gel intrarectally vs. 5 ml 2% lidocaine to junction of seminal vesicle and prostate vs. 5 ml normal saline to junction of seminal vesicle and prostate 10-core biopsies Biopsy pain*: 5.5 vs. 3.6 vs. 5.8; statistically significant difference in group 2 vs. group 3 ( p < 0.0001) * Pain evaluation: 10-point VAS pain during biopsy Alavi et al. [17] 75 (PPNB) vs. 75 (GEL) 10 ml 1% injected into periprostatic nerve plexus vs. 10 ml 2% Turbojet lidocaine intrarectally 6–14 (average 6.8 vs. 6.6) Mean pain*: 2.4 vs. 3.7 ( p = 0.00002) * Pain evaluation: 11 point-VAS (Wayne State University-VAS) Stirling et al. [18] 50 (no anaesthetic) vs. 50 (PPNB) vs. 50 (GEL) No anaesthetic vs. 5 ml 1% lidocaine periprostatic injection vs. 10 ml 2% lidocaine gel intrarectally Minimum 8 (average 9.6 vs. 9.4 vs. 9.3) Mean pain*: 3.8 vs. 2.6 vs. 3.1 ( p < 0.05) * Entire procedure pain evaluation: 11-point VAS Rodriguez et al. [19] 43 (GEL) vs. 53 (PPNB) 10 ml 2% lidocaine gel intrarectally vs. 10 ml 1% lidocaine solution injected at the prostate apex 6–14 (mean 7 vs. 8) Mean pain*: 2.76 vs. 1.73* ( p = 0.001) Mean pain*: 2.26 vs. 1.62** ( p < 0.001) * Pain evaluation: *10-point VAS and **5-point VAS Öbek et al. [20] 75 (no anaesthetic) vs. 75 (PPNB) vs. 75 (GEL + PPND) vs. 75 tramadol No anaesthetic vs. 5 ml 2% lidocaine injection lateral to junction of seminal vesicle and prostate vs. 10 ml 2% lidocaine gel perianal/rectal + 5 ml 2% lidocaine periprostatic infiltration vs. tramadol 1.5 mg/kg e.v. 12-core biopsies Mean pain*: 4.6 vs. 2.57 vs. 2.03 vs. 3.11; statistically significant difference only between group 3 and group 4 ( p = 0.006). * Pain evaluation: 11-point VAS european urology 52 (2007) 1309–1322 Matlaga et al. [13] PPNB = periprostatic nerve block; IRLA = intrarectal local anaesthesia; GEL = intrarectal anaesthetic gel; VAS = visual analog pain scale; TRUS = transrectal ultrasound. 1311 1312 european urology 52 (2007) 1309–1322 basolateral, posterolateral, periprostatic nerve plexus, prostate-vesicular junction injections) [17, 24,25], apex, and neurovascular bundle [22,23], and three locations (base, mid, and apex) posterolaterally [26] and lateral to the tip of the seminal vesicles [27] (Fig. 1). Even if infiltration of the neurovascular bundle region seems essential for effective anaesthesia, apical infiltration alone has been reported to provide significant pain relief [22,23]. Recently, it has been demonstrated that the combination of PPNB and periapical local anaesthesia is not superior to PPNB alone in reducing pain during PBx [28]. The issue of whether PPNB should be associated with IRLA or oral medication has been recently discussed by some authors [20,29]. Öbek et al [20] have demonstrated that the combination of PPNB and IRLA was superior to PPNB alone and concluded that this combined local anaesthesia could be considered a new gold standard. Pendleton et al [29] recently reported that oral administration of 75 mg tramadol/650 mg acetaminophen 3 h before PPNB appears to provide more effective pain control than PPNB alone without causing any additional complications. There is no doubt that the introduction of PPNB has allowed EPBx to be performed easily in the office and, furthermore, the number of biopsies taken to be increased (from 10 to 18 or 20) without increasing the discomfort and pain of the patients. Despite the Fig. 2 – Histologic slide shows an intracapsular prostate cancer on the left side. The arrows show the directions of the biopsies. The classic Hodge biopsies as well as the Stamey biopsies (more lateral) are not in the optimal direction to detect the tumour that is localised very laterally in the subcapsular position. Only lateral biopsies are useful to detect the prostate cancer. LH = lateral horn, a site where the tumor is often situated; TZ = transition zone; T = prostate cancer. variability of location and dosage of infiltration, the PPNB is, nowadays, the most effective method to reduce pain during TRUS biopsy. It is controversial whether PPNB should be associated with IRLA or oral medication. 2.2. Antibiotic prophylaxis Although published guidelines recommend prophylaxis for patients undergoing TRUS PBx because of the risk of urosepsis, the choice of antibacterial agent and duration of dosing are not consistent with the published recommendations and vary widely among urologists [9]. The antimicrobial prophylaxis is started the day before the EPBx and, in some cases, continued for 2–5 d [9]. The incidence of infection complications seems to be lower with longer duration of therapy in some but not all studies [30–32]. Schaeffer et al [32] have recently reported that a longer course (3 d) of antimicrobial prophylaxis (ciprofloxacin extended-release 1000) might be more beneficial than a short course (1–d). 3. Initial prostatic biopsy: from sextant to extended and saturation biopsy Over the last few years, interest has increased in defining a more efficient biopsy scheme for detecting prostate cancer. Intuitively, adding more biopsies to prostatic areas not sampled by standard sextant schemes should increase the detection rate for prostate cancer. However, it is not clear whether the increased detection rate is simply due to the additional biopsies or to the location from which the cores are taken. Although biopsies of the transitional zone have been reported to add little to cancer detection [33–42], it would appear that the addition of far lateral biopsies improves the detection rate of adenocarcinoma (Fig. 2). Several researchers [6–8] have evaluated the diagnostic yield of lateral biopsies within an EPBx. It has been reported that laterally directed biopsies, which are aimed at sampling also the lateral horn, yield about a 25% increase in the ability to detect prostate cancer [4,7,35]. The apex and the base of the peripheral gland are the sites at which prostate cancer is most likely to be located and at which the biopsies should be directed, whereas the midline biopsies have been demonstrated to have the lowest probability of being positive [7,35]. Most of the studies have demonstrated that EPBx has proven to be significantly superior to the sextant protocol in cancer detection, without significant morbidity and without increasing the number of insignificant cancer european urology 52 (2007) 1309–1322 cases [36]. There is no doubt that the direction and number of biopsies performed determine the procedure’s sensitivity. For these reasons the EPBx that optimises the detection rate should include six standard sextant biopsies with additional biopsies weighted more laterally at the base (lateral horn) and medially to the apex. The necessity of biopsying single hypoechoic lesions seems to be no longer necessary because the visible lesion itself is as likely to be the source of cancer as the next adjacent area [37]. More recently, some investigators have advocated even more aggressive biopsy schemes with >10–12 cores up to a saturation biopsy (24 cores) and reported even higher cancer detection rates [7,35]. Despite the use of an extended protocol, an increase in sampling error can occur in some patients, especially those with large prostate glands. It is well known that prostate volume is one of the factors that may influence the prediction of cancer at first biopsy and that a significant inverse relationship exists between the cancer detection rate and prostate volume [38]. Recently, it has been demonstrated that a scheme with eight cores turned out to be appropriate in patients with prostates < 30 cc. On the other hand, in prostates > 50 cc, an extended procedure with >12–14 cores was considered mandatory, even if the authors were not able to define the exact number of cores [39]. In a study of 303 patients comparing, directly in the same patient, the 6-, 12-, 18- and 21-core protocols, it was shown that a 21-sample needle biopsy procedure increased the prostate cancer detection rate [7]. The authors have reported a prostate cancer detection improvement of about 25% and 11% when 12- versus 6-core and 21- versus 12-core protocols were compared, respectively. Interestingly, they have demonstrated that the improvement was most marked in patients with a prostate volume of >40 cc. Unfortunately, these results should be interpreted with caution because most of the patients had already undergone a previous prostatic biopsy. Recently, it was shown that 14-core biopsies are superior to 8-core biopsies for patients with prostate volumes of 30–40 cc. A core number > 14 may be needed to detect cancer for prostate volumes in excess of 40 cc [40]. In an EPBx that included lesion-directed biopsies plus a 14-core biopsy scheme, the difference in the cancer detection rates of the sextant and the 8-core biopsy schemes was larger in cases with prostate volumes < 50 cc than in those with prostate volumes > 50 cc, whereas the difference in the detection rates of 8-core and 14-core biopsies was smaller in patients 1313 with prostate volumes < 50 cc than in those with prostate volumes > 50 cc [41]. On the other hand, it has been demonstrated that the saturation technique as an initial PBx strategy does not improve cancer detection [42]. Jones et al [42] have suggested that further efforts at extended biopsy strategies beyond 10–12 cores are not appropriate as an initial biopsy strategy. In a recent systematic review, Eichler et al [43] have shown that there is no significant benefit in taking > 12 cores and that methods requiring 18 cores have a poor side-effect profile. Moreover, a transperineal (TP) 6-core biopsy has a detection rate similar to that of a 12-core biopsy in patients presenting with PSA levels > 10 ng/ml and abnormal digital rectal examination (DRE) findings [44]. In conclusion, it is now reasonable to consider a sampling with 12 cores of the peripheral gland as adequate even if limiting the number of cores to 12 in larger prostate is of concern. 4. The risk of over-diagnosis The issue of nonsignificant prostate cancer is becoming more and more important because one possible disadvantage of the initial EPBx could escalate the risk of detecting small, possibly lowgrade, and clinically insignificant cancers. Even if the definition of clinically insignificant prostate cancer is controversial and poorly defined, evidence in the literature suggests that EPBx has really contributed to the detection of more cancers of smaller volume and of little clinical relevance, with the potential for over-diagnosis or over-treatment. Nevertheless, the concern of over-detection must be weighed against the risk of missing clinically significant malignancy and cancer detection does not need necessarily a linked treatment because men with low-volume and low-grade diseases may also be managed expectantly. There is no doubt that the recent stage migration of prostate cancer has been witnessed by regular increases in the proportion of patients with moderately differentiated low-volume tumour and a significant decrease in the volume of the cancers removed at surgery [45]. Recently, Master et al [46] demonstrated that a greater number of biopsies were associated with smaller tumour volumes at radical prostatectomy. Boccon-Gibod et al [47] have reported that 30% of patients with microfocal prostate cancer on EPBx have the risk of having insignificant tumour and of being over-treated. Moreover, no parameter was able to identify on an individual basis the patients harbouring a prostate 1314 european urology 52 (2007) 1309–1322 cancer potentially amenable to surveillance with delayed therapy. Nevertheless, using an initial EPBx, Siu et al [36] have demonstrated that it is possible not only to enhance tumour detection but also to ultimately lead to the finding of clinically significant disease. Similarly, Singh et al [6] have shown no apparent significant association between the increased number of cores and the finding of smaller and clinically insignificant cancer. Meng et al [48] have recently demonstrated that performing more extensive biopsies does not significantly increase the number of lower-risk tumours identified. They have reported that there are no differences in disease characteristics and biochemical-free survival among men with a biopsy number between 6 and 17. Unfortunately, some methodologic flaws, such as a short median follow-up of just 2.2 yr, diminish the value of their results. Even if the authors concluded that increasing the number of cores does not affect the detection of lower-risk tumours, the usefulness of improved and earlier identification of cancers in altering the natural history remains uncertain. Thus, even if the use of EPBx is recommended, the risk of detecting insignificant tumour should not be neglected. Nevertheless, saturation biopsies/rebiopsies, which are now used as part of active surveillance protocols, have recently proved to provide helpful information about quantitative and qualitative histology to predict the clinical significance of prostate cancer [49,50]. 20% [51]. Djavan et al [51] reported cancer detection rates on subsequent sets of biopsies one, two, three, and four of 22%, 10%, 5%, and 4%, respectively, in men with total serum PSA level of 4–10 ng/ml. Recently, different researchers have demonstrated that saturation biopsy techniques aimed at greatly increasing the number of samples and varying the distribution of biopsy sites may provide a higher cancer detection rate (Table 2). The detection rate of prostate cancer ranged from 17% to 41%, and the likelihood of clinically insignificant cancers was not significantly increased compared with initial or repeat biopsy [52–58]. Saturation biopsies have a safe profile and are particularly useful in larger-volume prostates. Borboroglu et al [52] used an extensive TR saturation technique to obtain an average of 22.5 cores/patient and reported a cancer detection rate of 30%. A larger series with a different TR saturation biopsy scheme was reported by Stewart et al [53], who reported a cancer detection rate of 34%. Recently, Walz et al [57] reported a high prostate cancer detection rate of 41% with a 24-core protocol. Similarly to the initial biopsy protocol, it has been proven that more time and effort should be spent on lateral biopsies, which increase the cancer detection rate, whereas parasagittal biopsy provides a low yield on repeat PBx [56]. Although saturation biopsy is becoming more often the preferred repeat biopsy scheme, as yet no clear criteria indicate when to perform a rebiopsy in patients with persistently elevated levels of PSA. 6. 5. Repeat biopsy: from extended to saturation biopsy The management of patients with persistently elevated levels of PSA in whom a first set of prostate biopsies has been negative for cancer is a daily problem for urologists. The cancer detection rate on repeat not-extended biopsy ranges between 10% and Transrectal versus TP The TP PBx is unusual, especially in the United States, even if some institutions in European and Asian countries perform TP PBx exclusively. Theoretically, the direction of the TP biopsies might be better than the transrectal (TR) route because they sample longitudinally the peripheral zone of the prostate. Initially the TP route was demonstrated to Table 2 – Comparison of saturation biopsy studies in patients undergoing rebiopsy Author Year No. of patients Mean/median PSA, ng/ml Borboroglu et al. [52] Stewart et al. [53] Fleshner et al. [54] Rabets et al. [55] Patel et al. [56] Pinkstaff et al. [58] Walts et al. [57] 2000 2001 2002 2004 2004 2005 2006 57 224 37 116 100 210 161 8.6 8.7 22.4 9.2 9.4 13.6 9.4 PSA = prostate-specific antigen. No. of cores 22.5 23 32–38 22.8 20–24 21.2 24.2 Cancer detection rate 30% 34% 13.5% 29% 25% 37% 41% european urology 52 (2007) 1309–1322 be less accurate than the TR approach in identifying all the hypoechoic lesions [59]. Subsequently, the same group of authors [60] also reported that TP-guided sextant biopsies were less accurate than TRUS-guided sextant biopsies in detecting prostate cancer. In a simulation experiment, Vis et al [61] have shown that the two approaches did not differ in prostate cancer detection. Emiliozzi et al [62] were the first to compare in vivo the two different approaches, and they have shown that the sextant TP biopsy seems superior to TR biopsy in detecting prostate cancer. The same authors [62] and Takenaka et al [63] have subsequently reported that the 12-core TP PBx is superior to 6-core biopsy and have shown that the number of cores may have a greater impact on cancer detection than the route of the PBx. In the last few years, the concept of extended biopsies has been equally applied to the TP approach, with results similar to those achieved with the TR approach in patients underoig rebiopsy procedures. The demonstration that the two approaches were equivalent in cancer detection was obtained only from reports of some Japanese urologists who had performed TR and TP biopsies in the same patients. Watanabe et al [64] compared 6-core TR and 6-core TP biopsies, and Kawakami et al [65] compared 12-core TR and 14-core TP biopsies. Both studies have shown that the overall cancer detection rate did not differ for the two approaches when the same number of cores were used, even if the two approaches combined were better than a single approach. 7. The role of nomograms Detection of prostate cancer detection can be improved either with a better sampling of prostate cancer or by improving the indication for a PBx. The notion that combined input of multiple predictors usually exceeds that of most informative single variables has led to the development of artificial neural networks or nomograms to predict the probability of having cancer. Artificial neural networks have limited clinical applicability, and they have proven to be less accurate than nomograms in predicting the outcome of an initial biopsy [66]. Recently, different authors have reported nomograms based on extended biopsy protocol [66,67]. Chun et al [68] developed a useful nomogram based on a cohort of 2900 men exposed to 10 biopsy cores. Predictors included age, DRE, PSA, percent free PSA, and sampling density (ie, ratio of gland volume and the number of planned biopsy cores), which were 1315 included in multivariable logistic regression models predicting presence of prostate cancer. The nomogram was 77% accurate and also allowed the definition of the ideal ratio between gland volume and the number of planned biopsy cores that would yield the ideal biopsy rate. Within the repeat biopsy setting, a novel nomogram including only patients undergoing extended biopsy schemes at final repeat biopsy has been reported with an accuracy of 77%, which exceeded the accuracies of previously published nomograms [69]. Therefore, nomograms represent a valid methodologic approach for detection of prostate cancer both at initial and repeat biopsy, if correct criteria are met. The availability of such high-quality predictive models should encourage the clinician to adopt these tools in everyday clinical practice. 8. Improving cancer detection by means of Doppler imaging Standard grey-scale TRUS technology has limited specificity and sensitivity for prostate cancer detection because of its inability to detect isoechoic neoplasms. To increase its accuracy and utility, researchers have investigated a number of alternatives, including colour Doppler TRUS (CDUS), power Doppler imaging (PDI) with and without intravenous contrast administration, and, recently, elastography [65]. Increased microvascularity accompanies cancer growth, and neovascularity may be detectable by CDUS and PDI because of abnormal blood flow patterns in larger feeding vessels. Some studies have shown that CDUS did not add significant information to grey-scale TRUS in detecting early stages of prostate cancer, whereas others have demonstrated varying degrees of benefit [70,71]. Overall, the sensitivity of CDUS for the diagnosis of prostate cancer ranged between 49% and 87%, and specificity ranged between 38% and 93% [71]. PDI is considered the next generation of colour Doppler imaging because it has the advantage of increased sensitivity for detecting small, low-flow blood vessels. Halpern et al [72] have shown that PDI may be useful for targeted biopsies when the number of biopsy passes must be limited but that there is no substantial advantage of PDI over CDUS. Remzi et al [73] have recently reported that PDI has a high negative predictive value and may help to reduce the number of unnecessary biopsies because a normal power Doppler TRUS signal might exclude the presence of a prostate cancer. 1316 european urology 52 (2007) 1309–1322 Contrast-enhanced colour Doppler (CECD) is an ultrasound-based technology for imaging of the prostate that is used after intravenous administration of gas-encapsulated microbubbles. This methodology allows for better prostate cancer visualisation and for targeted biopsies to isoechoic areas that generally become hypervascular after contrast infusion. Halpern et al [74] have reported significantly improved sensitivity, from 38% to 65%, for detecting prostate cancer with preserved specificity at approximately 80%. Recently, different authors have demonstrated that targeted biopsy with CECD detects a number of tumours equal to that of systematic biopsies with less than half the number of cores [74–76]. Unfortunately, the poor discrimination of benign from malignant tissue, which is due to the CECD ultrasound signal arising from areas of benign disease such as benign prostatic hyperplasia, has diminished the specificity of this technology. Recently, it has been reported that short-term oral therapy with a 5a-reductase inhibitor combined with dutasteride may improve prostate cancer detection if used with CECD ultrasound [77]. Despite these promising results, CECD has not yet gained popularity because of its low specificity, complexity, and high cost. Some investigators [70] reported the use of sonography with manual compression of the prostate gland with the TR probe to generate elastograms. The basis for improved detection of cancer is that the elasticity of the neoplastic tissue is less compared with normal prostate tissue. The limited amount of data available on the ability of elastography to detect prostate cancer show that a targeted biopsy detects as many cancers as a systematic biopsy with less than half the number of biopsy cores, but more clinical trails are needed to determine the exact role of this advantage for TRUS [70]. 9. Gleason concordance on EPBx Different studies have demonstrated that the ability to predict the final Gleason score by means of standard sextant biopsy is quite poor with a concordance rate between the biopsy and prostatectomy Gleason scores of only 28–48% [78]. On average, the Gleason score is under-graded in 43% of cases (Table 3). The use of EPBx has been beneficial in the pretreatment decision-making process because an increased number of biopsies increase the Gleason concordance. San Francisco et al [79] reported an improvement in the concordance rate from 63% to 72%. Mian et al [80] reported that the rate of upgrading to a worsening risk category was significantly reduced with EPBx. Numao et al [81] recently reported that a 26-core systematic biopsy can more accurately predict the presence of Gleason pattern 4/5 on surgical specimen compared with transrectal 12-core PBx. Table 3 – Grade of discordance, biopsy upgrading and downgrading with not-extended and extended protocols according to different authors Authors Year No. of cores taken Grade of discordance San Francisco et al. [79] 2003 9 10 37% 24% 12% 10% 25% 14% King et al. [78] 2004 6 10 38% 37% 25% 12% 12% 25% Emiliozzi et al. [94] 2004 6 12 51% 30% 11% 6% 39% 24% Coogan et al. [95] 2005 6 8 10 58.9 60 42.5 19.6% 23% 11% 39.2% 36.9% 31.5% Mian et al. [80] 2006 6 12 52% 32% 41% 17% NR NR Numao et al. [81] 2006 TP 14 TR 12 3D 26 15% 17% 7.7% NR NR 2% 51% 48% 26% Elabbady et al. [5] 2006 6 12 50% 24.8% NR NR NR = not reported; TP = transperineal; TR = transrectal; 3D = three-dimensional. Biopsy upgrading Biopsy downgrading european urology 52 (2007) 1309–1322 King et al distinguished between any upgrading and significant upgrading (Gleason sum increases either from 6 to 7 or from 7 to 8) and suggested that significant upgrading represents a clinically meaningful entity. Different authors [81–83] have demonstrated that, with more EPBx, the risk of significant upgrading decreases because of higher sampling density and more accurate pathologic biopsy evaluation. The two largest published cohorts [86,87] showed a rate of overall Gleason sum upgrading of 29.3% and 32.6% and a rate of significant upgrading of 32% and 28.2%, respectively. Because significant Gleason sum upgrading between biopsy and final pathology may have an impact on treatment decision-making, predictive nomograms have been developed as prognostic models capable of predicting the probability of significant upgrading [84,85]. 10. Quantitative histology on EPBx The amount of tumour in prostate needles can be expressed by the number of positive cores or by the amount of tumour per core. This parameter is an extremely important pathologic parameter and a predictor of a lethal phenotype of prostate cancer or a clinically insignificant cancer (Tables 4 and 5) [86,87]. The extent of involvement of needle cores by prostatic adenocarcinoma has been shown to correlate (albeit not perfectly) with the Gleason Table 4 – Prostate biopsy reporting Parameters that should be reported 1. Number and total length of the cores (exclude those <1 cm and those without epithelial component) 2. Number of cores with cancer (percentage of cores involved) 3. Longest single length of tumour (report also the location) 4. Total tumour length in all cores 5. Mean tumour length in all cores (reported as a percentage): total tumour length divided by total length of cores multiplied by 100 (ie, overall percentage of cancer in all biopsies) 6. Number of cores with perineural invasion (extent: focal, multifocal) and calibre of nerve bundles 7. Number of cores with vascular invasion 8. Composite (global) Gleason score for all cores for the patient 9. Number and location of cores with atypical glands, suspicious for cancer 10. HGPIN (extent; focality: focal or multifocal; number of cores involved; laterality: unilateral or bilateral) Each core (slide) is reported individually (see the example below): 1. Prostate biopsy of 1.4 cm occupied for 7 mm (50% of the core length) by acinar adenocarcinoma, Gleason score 3 + 3 = 6. Perineural invasion is present. 2. Prostate biopsy of 1.3 cm with normal prostate tissue HGPIN = high-grade prostatic intraepithelial neoplasia. 1317 score, pathologic stage, surgical margins, but, especially, with tumour volume [88]. As the number of positive cores and the amount of tumour per core increase, the larger the tumour volume is likely to be. The extent of needle core involvement, including bilateral involvement, has also been shown to predict biochemical recurrence, postprostatectomy progression, and radiation therapy failure in univariate analysis and often in multivariate analysis [89,90]. It is a parameter included in some recent nomograms created to predict pathologic stage and seminal vesicle invasion after radical prostatectomy and radiation therapy failure. Although the correlation for high tumour burden in needle biopsies is directly proportional to the likelihood of an adverse outcome, low tumour burden in needle biopsies is not necessarily an indicator of low-volume and low-stage cancer in the prostatectomy specimen. For instance, an apparently favourable report with only one or two cores positive for cancer or a limited extent of <3 mm of cancer does not act as a guarantee for either organ-confined prostate cancer or insignificant cancer after radical prostatectomy [91]. As with the other parameters, a combination of the extent of involvement of needle cores with the Gleason score, location of the tumour, and serum PSA levels increases the prognostic and predictive power of this parameter [91]. In one study [91], the percentage of cancer in biopsies from the base correlated with extraprostatic extension. In other studies, a Gleason score of 7–9 cancer in the midprostate or base biopsies correlated with the risk of seminal vesicle invasion and lymph node metastasis, and a tumour volume of >50% in base biopsies correlated with a prediction of extraprostatic extension at the neurovascular bundle and posterior lateral region [92]. Moreover, the amount of cancer in apex biopsies has been shown to correlate with apical margin positivity [93]. The number and percentage of positive biopsy cores have also proven to improve the ability to predict lymph node invasion in patients undergoing radical prostatectomy and extended pelvic lymph node dissection (Table 6) [86]. There is lack of consensus in the literature with regards to the best method of reporting the extent of tumour involvement. It is recommended that the report should provide the number of involved cores. Typically, small foci are reported as <1% or <5%, and so forth, of needle core biopsies, and linear length is reported in increments of 0.5 mm. The correlation, as alluded to before with prognosis, is with greater involvement of the cores, and studies have shown various cut-off values (33%, 34–50%, and 51–100%, 1318 european urology 52 (2007) 1309–1322 Table 5 – Preoperative parameters predicting the presence of insignificant prostate cancer according to different authors Authors Origin of cohort % of IPCa Biopsy protocol Preoperative parameters predicting the presence of IPCa Epstein et al. [96] United States 26% Sextant Gleason sum 6 Adenocarcinoma present in fewer than 3 of 6 cores No more than 50% malignant involvement in each positive biopsy core PSA density < 0.15 ng/ml/g Goto et al. [97] United States 10% Sextant Quantitative analysis of the extent of cancer PSA, PSA density, and grade Carter et al. [98] United States 17% Sextant PSA density Quantitative histology (number of cores involved with cancer and percentage of cancer within the core) Epstein et al. [99] United States 30% Sextant Needle biopsy findings Free/total PSA levels Kattan et al. [100] United States 20% 6 Nomograms incorporating pretreatment variables (clinical stage, Gleason grade, PSA, and the amount of cancer in a systematic biopsy specimen) Ochiai et al. [101] United States 22% Extended (10–11 cores) Combination of tumour length < 2 mm, Gleason score 3 + 4, and prostate volume > 50 cc Augustin et al. [102] Europe 6% Sextant PSA density Percent of cancer per biopsy Chun et al. [68] Europe 6% 6 Preoperative nomograms (predictor variables: PSA, clinical stage, biopsy Gleason scores, core cancer length, and percent of positive biopsy cores) Miyake et al. [103] Japan 14% 8 Gleason score < 7 Percent positive biopsy core < 15% IPCa = insignificant prostate cancer defined as tumour < 0.5 cc and no Gleason 4 and 5 at final pathology; PSA = prostate-specific antigen. or 20%, 21–55% and >56%, etc) to be of significance [93]. Because literal translation of these findings to clinical cases would be difficult and not really necessary, reporting the percentage of cancer involvement in increments of 5% or 10% is appropriate. 11. Table 6 – Importance of knowing the specific location of the biopsy and the location of cancer 1. Tumour involvement of base biopsies may influence bladder-neck–sparing radical prostatectomy. 2. Extensive cancer in base biopsies correlates with extraprostatic extension. 3. Dominant side of prostate biopsy correlates with ipsilateral positivity of surgical margins and extraprostatic extension. 4. Knowledge of location of cancer may help target additional tissue or block sampling in cases with no apparent cancer in radical prostatectomy sections. 5. Knowledge of biopsy site helps recognise potential diagnostic pitfalls (eg, seminal vesicle epithelium or central zone epithelium, seen most frequently in base biopsies and the rare Cowper’s glands in apex biopsies). 6. Knowledge of biopsy site and location of cancer allows detailed correlation with digital rectal examination and imaging studies. 7. Laterality is useful in planning of nerve-sparing radical prostatectomy. 8. Map distribution of prostate cancer is useful for planning the field of radiation therapy (eg, in brachytherapy). Conclusions Despite years of research, the exact number of biopsies to be taken to (1) detect significant prostate cancers, (2) predict the actual tumour volume, and (3) rule out insignificant prostate cancer is still largely unknown. Despite development of PDI, CDUS, and CECD, which allow performance of targeted biopsies, the current trend is to use, more and more often, EPBx (10- to 12-core biopsy without the transition zone) as the initial biopsy strategy. Moreover, the inability to better determine who needs to undergo biopsy and the reliance on Gleason score are the two main factors that contribute to the dependence on a greater number of biopsies. In men with persistent suspicion of prostate cancer after several negative biopsies, more extensive protocols (>12 cores) up to saturation biopsy represent a necessary diagnostic procedure that has proven to have a safe profile. The issue of whether an increase in number of biopsy cores taken results in the european urology 52 (2007) 1309–1322 detection of more tumours with a lower-risk feature remains controversial. [15] Conflicts of interest [16] The authors have nothing to disclose. References [1] Derweesh IH, Kupelian PA, Zippe C, et al. Continuing trends in pathological stage migration in radical prostatectomy specimens. Urol Oncol 2004;22:300–6. [2] Stamey TA. Making the most out of six systematic sextant biopsies. Urology 1995;45:2–12. [3] Presti Jr JC. Prostate biopsy: how many cores are enough? Urol Oncol 2003;21:135–40. [4] Meng MV, Franks JH, Presti Jr JC, Shinohara K. The utility of apical anterior horn biopsies in prostate cancer detection. Urol Oncol 2003;21:361–5. [5] Elabbady AA, Khedr MM. Extended 12-core prostate biopsy increases both the detection of prostate cancer and the accuracy of Gleason score. Eur Urol 2006;49:49–53. [6] Singh H, Canto EI, Shariat SF, et al. Improved detection of clinically significant, curable prostate cancer with systematic 12-core biopsy. J Urol 2004;171:1089–92. [7] De la Taille A, Antiphon P, Salomon L, et al. Prospective evaluation of a 21-sample needle biopsy procedure designed to improve the prostate cancer detection rate. Urology 2003;61:1181–6. [8] Presti Jr JC, O’Dowd GJ, Miller MC, Mattu R, Veltri RW. Extended peripheral zone biopsy schemes increase cancer detection rates and minimize variance in prostate specific antigen and age related cancer rates: results of a community multi-practice study. J Urol 2003;169:125–9. [9] Bertaccini A, Fandella A, Prayer-Galetti T, et al. Systematic development of clinical practice guidelines for prostate biopsies: a 3-year Italian project. Anticancer Res 2007;27:659–66. [10] Autorino R, De Sio M, Di Lorenzo G, et al. How to decrease pain during transrectal ultrasound guided prostate biopsy: a look at the literature. J Urol 2005;174:2091–7. [11] Raber M, Scattoni V, Roscigno M, Rigatti P, Montorsi F. Perianal and intrarectal anaesthesia for transrectal biopsy of the prostate: a prospective randomized study comparing lidocaine-prilocaine cream and placebo. BJU Int 2005;96:1264–7. [12] Tiong HY, Liew LC, Samuel M, Consigliere D, Esuvaranathan K. A meta-analysis of local anesthesia for transrectal ultrasound-guided biopsy of the prostate. Prostate Cancer Prostatic Dis 2007;10:127–36. [13] Matlaga BR, Lovato JF, Hall MC. Randomized prospective trial of a novel local anesthetic technique for extensive prostate biopsy. Urology 2003;61:972–6. [14] Adamakis I, Mitropoulos D, Haritopoulos K, Alamanis C, Stravodimos K, Giannopoulos A. Pain during transrectal ultrasonography guided prostate biopsy: a randomized prospective trial comparing periprostatic infiltration [17] [18] [19] [20] [21] [22] [23] [24] [25] [26] [27] [28] 1319 with lidocaine with the intrarectal instillation of lidocaine-prilocaine cream. World J Urol 2004;22:281–4. Lynn NN, Collins GN, Brown SC, O’Reilly PH. Periprostatic nerve block gives better analgesia for prostatic biopsy. BJU Int 2002;90:424–6. Song SH, Kim JK, Song K, Ahn H, Kim CS. Effectiveness of local anaesthesia techniques in patients undergoing transrectal ultrasound-guided prostate biopsy: a prospective randomized study. Int J Urol 2006;13:707–10. Alavi AS, Soloway MS, Vaidya A, Lynne CM, Gheiler EL. Local anesthesia for ultrasound guided prostate biopsy: a prospective randomized trial comparing 2 methods. J Urol 2001;166:1343–5. Stirling BN, Shockley KF, Carothers GG, Maatman TJ. Comparison of local anesthesia techniques during transrectal ultrasound-guided biopsies. Urology 2002;60:89– 92. Rodriguez A, Kyriakou G, Leray E, Lobel B, Guillé F. Prospective study comparing two methods of anaesthesia for prostate biopsies: apex periprostatic nerve block versus intrarectal lidocaine gel: review of the literature. Eur Urol 2003;44:195–200. Öbek C, Ozkan B, Tunc B, Can G, Yalcin V, Solok V. Comparison of 3 different methods of anesthesia before transrectal prostate biopsy: a prospective randomized trial. J Urol 2004;172:502–5. Ozden E, Yaman O, Gogus C, Ozgencil E, Soygur T. The optimum doses of and injection locations for periprostatic nerve blockade for transrectal ultrasound guided biopsy of the prostate: a prospective, randomized, placebo controlled study. J Urol 2003;170:2319–22. Schostak M, Christoph F, Muller M, et al. Optimizing local anesthesia during 10-core biopsy of the prostate. Urology 2002;60:253–7. Seymour H, Perry MJ, Lee-Elliot C, Dundas D, Patel U. Pain after transrectal ultrasonography-guided prostate biopsy: the advantages of periprostatic local anaesthesia. BJU Int 2001;88:540–4. von Knobloch R, Weber J, Varga Z, Feiber H, Heidenreich A, Hofmann R. Bilateral fine-needle administered local anaesthetic nerve block for pain control during TRUSguided multi-core prostate biopsy: a prospective randomised trial. Eur Urol 2002;41:508–14. Addla SK, Adeyoju AA, Wemyss-Holden GD, Neilson D. Local anaesthetic for transrectal ultrasound-guided prostate biopsy: a prospective, randomized, double blind, placebo-controlled study. Eur Urol 2003;43:441–3. Leibovici D, Zisman A, Siegel YI, Sella A, Kleinmann J, Lindner A. Local anesthesia for prostate biopsy by periprostatic lidocaine injection: a double-blind placebo controlled study. J Urol 2002;167:563–5. Wu CL, Carter HB, Naqibuddin M, Fleisher LA. Effect of local anesthetics on patient recovery after transrectal biopsy. Urology 2001;57:925–9. Cevik I, Dillioglugil O, Zisman A, Akdas A. Combined ‘‘periprostatic and periapical’’ local anesthesia is not superior to ‘‘periprostatic’’ anesthesia alone in reducing pain during Tru-Cut prostate biopsy. Urology 2006;68: 1215–9. 1320 european urology 52 (2007) 1309–1322 [29] Pendleton J, Costa J, Wludyka P, Carvin DM, Rosser CJ. Combination of oral tramadol, acetaminophen and 1% lidocaine induced periprostatic nerve block for pain control during transrectal ultrasound guided biopsy of the prostate: a prospective, randomized, controlled trial. J Urol 2006;176:1372–5. [30] Janoff DM, Skarecky DW, McLaren CE, Ahlering TE. Prostate needle biopsy infection after four or six dose ciprofloxacin. Can J Urol 2000;7:1066–9. [31] Sabbagh R, McCormack M, Peloquin F, et al. A prospective randomized trial of 1-day versus 3-day antibiotic prophylaxis for transrectal ultrasound guided prostate biopsy. Can J Urol 2004;11:2216–9. [32] Schaeffer AJ, Montorsi F, Scattoni V, et al. Comparison of a 3-day with a 1-day regimen of an extended-release formulation of ciprofloxacin as antimicrobial prophylaxis for patients undergoing transrectal needle biopsy of the prostate. BJU Int 2007;100:51–7. [33] Pelzer AE, Bektic J, Berger AP, et al. Are transition zone biopsies still necessary to improve prostate cancer detection? Results from the Tyrol screening project. Eur Urol 2005;48:916–21. [34] Peyromaure M, Ravery V, Boccon-Gibod L. The role of the biopsy of the transitional zone and of the seminal vesicles in the diagnosis and staging of prostate cancer. Eur Urol Suppl 2002;1(6):40–6. [35] Eskew LA, Bare RL, McCullough DL. Systematic 5 region prostate biopsy is superior to sextant method for diagnosing carcinoma of the prostate. J Urol 1997;157: 199–202. [36] Siu W, Dunn RL, Shah RB, Wei JT. Use of extended pattern technique for initial prostate biopsy. J Urol 2005;174:505–9. [37] Onur R, Littrup PJ, Pontes JE, Bianco Jr FJ. Contemporary impact of transrectal ultrasound lesions for prostate cancer detection. J Urol 2004;172:512–4. [38] Djavan B. Prostate biopsies and Vienna nomograms. Eur Urol Suppl 2006;5:500–10. [39] Ficarra V, Novella G, Novara G, et al. The potential impact of prostate volume in the planning of optimal number of cores in the systematic transperineal prostate biopsy. Eur Urol 2005;48:932–7. [40] Inahara M, Suzuki H, Kojima S, et al. Improved prostate cancer detection using systematic 14-core biopsy for large prostate glands with normal digital rectal examination findings. Urology 2006;68:815–9. [41] Damiano R, Autorino R, Perdona S, et al. Are extended biopsies really necessary to improve prostate cancer detection? Prostate Cancer Prostatic Dis 2003;6:250–5. [42] Jones JS, Patel A, Schoenfield L, Rabets JC, Zippe CD, Magi-Galluzzi C. Saturation technique does not improve cancer detection as an initial prostate biopsy strategy. J Urol 2006;175:485–8. [43] Eichler K, Hempel S, Wilby J, Myers L, Bachmann LM, Kleijnen J. Diagnostic value of systematic biopsy methods in the investigation of prostate cancer: a systematic review. J Urol 2006;175:1605–12. [44] Luciani LG, De Giorgi G, Valotto C, Zanin M, Bierti S, Zattoni F. Role of transperineal six-core prostate biopsy in patients with prostate-specific antigen level greater [45] [46] [47] [48] [49] [50] [51] [52] [53] [54] [55] [56] [57] [58] [59] [60] [61] than 10 ng/mL and abnormal digital rectal examination findings. Urology 2006;67:555–8. Cooperberg MR, Lubeck DP, Meng MV, Mehta SS, Carroll PR. The changing face of low-risk prostate cancer: trends in clinical presentation and primary management. J Clin Oncol 2004;22:2141–9. Master VA, Chi T, Simko JP, Weinberg V, Carroll PR. The independent impact of extended pattern biopsy on prostate cancer stage migration. J Urol 2005;174:1789–93. Boccon-Gibod LM, Dumonceau O, Toublanc M, Ravery V, Boccon-Gibod LA. Micro-focal prostate cancer: a comparison of biopsy and radical prostatectomy specimen features. Eur Urol 2005;48:895–9. Meng MV, Elkin EP, DuChane J, Carroll PR. Impact of increased number of biopsies on the nature of prostate cancer identified. J Urol 2006;176:63–8. Boccon-Gibod LM, de Longchamps NB, Toublanc M, Boccon-Gibod LA, Ravery V. Prostate saturation biopsy in the reevaluation of microfocal prostate cancer. J Urol 2006;176:961–3. Epstein JI, Sanderson H, Carter HB, Scharfstein DO. Utility of saturation biopsy to predict insignificant cancer at radical prostatectomy. Urology 2005;66:356–60. Djavan B, Remzi M, Marberger M. When and how a prostatic re-biopsy should be performed? Eur Urol Suppl 2002;1(6):52–9. Borboroglu PG, Comer SW, Riffenburgh RH, Amling CL. Extensive repeat transrectal ultrasound guided prostate biopsy in patients with previous benign sextant biopsies. J Urol 2000;163:158–62. Stewart CS, Leibovich BC, Weaver AL, Lieber MM. Prostate cancer diagnosis using a saturation needle biopsy technique after previous negative sextant biopsies. J Urol 2001;166:86–91. Fleshner N, Klotz L. Role of ‘‘saturation biopsy’’ in the detection of prostate cancer among difficult diagnostic cases. Urology 2002;60:93–7. Rabets JC, Jones JS, Patel A, Zippe CD. Prostate cancer detection with office based saturation biopsy in a repeat biopsy population. J Urol 2004;172:94–7. Patel AR, Jones JS, Rabets J, DeOreo G, Zippe CD. Parasagittal biopsies add minimal information in repeat saturation prostate biopsy. Urology 2004;63:87–9. Walz J, Graefen M, Chun FK, et al. High incidence of prostate cancer detected by saturation biopsy after previous negative biopsy series. Eur Urol 2006;50:498–505. Pinkstaff DM, Igel TC, Petrou SP, Broderick GA, Wehle MJ, Young PR. Systematic transperineal ultrasound-guided template biopsy of the prostate: three-year experience. Urology 2005;65:735–9. Terris MK, Hammerer PG, Nickas ME. Comparison of ultrasound imaging in patients undergoing transperineal and transrectal prostate ultrasound. Urology 1998;52:1070–2. Shinghal R, Terris MK. Limitations of transperineal ultrasound-guided prostate biopsies. Urology 1999;54:706–8. Vis AN, Boerma MO, Ciatto S, Hoedemaeker RF, Schroder FH, van der Kwast TH. Detection of prostate cancer: a comparative study of the diagnostic efficacy of sextant european urology 52 (2007) 1309–1322 [62] [63] [64] [65] [66] [67] [68] [69] [70] [71] [72] [73] [74] [75] [76] [77] transrectal versus sextant transperineal biopsy. Urology 2000;56:617–21. Emiliozzi P, Corsetti A, Tassi B, Federico G, Martini M, Pansadoro V. Best approach for prostate cancer detection: a prospective study on transperineal versus transrectal six-core prostate biopsy. Urology 2003;61:961–6. Takenaka A, Hara R, Hyodo Y, et al. Transperineal extended biopsy improves the clinically significant prostate cancer detection rate: a comparative study of 6 and 12 biopsy cores. Int J Urol 2006;13:10–4. Watanabe M, Hayashi T, Tsushima T, Irie S, Kaneshige T, Kumon H. Extensive biopsy using a combined transperineal and transrectal approach to improve prostate cancer detection. Int J Urol 2005;12:959–63. Kawakami S, Okuno T, Yonese J, et al. Optimal sampling sites for repeat prostate biopsy: a recursive partitioning analysis of three-dimensional 26-core systematic biopsy. Eur Urol 2007;51:675–83. Chun FK, Graefen M, Briganti A, et al. Initial biopsy outcome prediction—head-to-head comparison of a logistic regression-based nomogram versus artificial neural network. Eur Urol 2007;51:1236–43. Chun FK, Karakiewicz PI, Briganti A, et al. Prostate cancer nomograms: an update. Eur Urol 2006;50:914–26. Chun FK, Briganti A, Graefen M, et al. Development and external validation of an extended 10-core biopsy nomogram. Eur Urol 2007;52:436–45. Chun FK, Briganti A, Graefen M, et al. Development and external validation of an extended repeat biopsy nomogram. J Urol 2007;177:510–5. Pallwein L, Mitterberger M, Gradl J, et al. Value of contrast-enhanced ultrasound and elastography in imaging of prostate cancer. Curr Opin Urol 2007;17:39–47. Amiel GE, Slawin KM. Newer modalities of ultrasound imaging and treatment of the prostate. Urol Clin North Am 2006;33:329–37. Halpern EJ, Strup SE. Using gray-scale and color and power Doppler sonography to detect prostatic cancer. AJR Am J Roentgenol 2000;174:623–7. Remzi M, Dobrovits M, Reissigl A, et al., European Society for Oncological Urology (ESOU). Can power Doppler enhanced transrectal ultrasound guided biopsy improve prostate cancer detection on first and repeat prostate biopsy? Eur Urol 2004;46:451–6. Halpern EJ, Ramey JR, Strup SE, Frauscher F, McCue P, Gomella LG. Detection of prostate carcinoma with contrast-enhanced sonography using intermittent harmonic imaging. Cancer 2005;104:2373–83. Pelzer A, Bektic J, Berger AP, et al. Prostate cancer detection in men with prostate specific antigen 4 to 10 ng/ml using a combined approach of contrast enhanced color Doppler targeted and systematic biopsy. J Urol 2005;173:1926–9. Frauscher F, Klauser A, Volgger H, et al. Comparison of contrast enhanced color Doppler targeted biopsy with conventional systematic biopsy: impact on prostate cancer detection. J Urol 2002;167:1648–52. Mitterberger M, Pinggera G, Horninger W, et al. Dutasteride prior to contrast-enhanced colour Doppler ultrasound prostate biopsy increases prostate cancer [78] [79] [80] [81] [82] [83] [84] [85] [86] [87] [88] [89] [90] 1321 detection. Eur Urol. In press. doi:10.1016/j.eururo. 2007.02.031. King CR, McNeal JE, Gill H, Presti Jr JC. Extended prostate biopsy scheme improves reliability of Gleason grading: implications for radiotherapy patients. Int J Radiat Oncol Biol Phys 2004;59:386–91. San Francisco IF, DeWolf WC, Rosen S, Upton M, Olumi AF. Extended prostate needle biopsy improves concordance of Gleason grading between prostate needle biopsy and radical prostatectomy. J Urol 2003;169:136–40. Mian BM, Lehr DJ, Moore CK, et al. Role of prostate biopsy schemes in accurate prediction of Gleason scores. Urology 2006;67:379–83. Numao N, Kawakami S, Yokoyama M, et al. Improved accuracy in predicting the presence of Gleason pattern 4/ 5 prostate cancer by three-dimensional 26-core systematic biopsy. Eur Urol. In press. doi:10.1016/j.eururo.2007. 01.025. King CR, Patel DA, Terris MK. Prostate biopsy volume indices do not predict for significant Gleason upgrading. Am J Clin Oncol 2005;28:125–9. Freedland SJ, Kane CJ, Amling CL, Aronson WJ, Terris MK, Presti Jr JC. SEARCH Database Study Group. Upgrading and downgrading of prostate needle biopsy specimens: risk factors and clinical implications. Urology 2007;69:495–9. Chun FK, Briganti A, Shariat SF, et al. Significant upgrading affects a third of men diagnosed with prostate cancer: predictive nomogram and internal validation. BJU Int 2006;98:329–34. Chun FK, Steuber T, Erbersdobler A, et al. Development and internal validation of a nomogram predicting the probability of prostate cancer Gleason sum upgrading between biopsy and radical prostatectomy pathology. Eur Urol 2006;49:820–6. Briganti A, Chun FK, Hutterer GC, et al. Systematic assessment of the ability of the number and percentage of positive biopsy cores to predict pathologic stage and biochemical recurrence after radical prostatectomy. Eur Urol 2007;52:733–45. Briganti A, Karakiewicz PI, Chun FK, et al. Percentage of positive biopsy cores can improve the ability to predict lymph node invasion in patients undergoing radical prostatectomy and extended pelvic lymph node dissection. Eur Urol 2007;51:1573–81. Zhou M, Epstein JI. The reporting of prostate cancer on needle biopsy: prognostic and therapeutic implications and the utility of diagnostic markers. Pathology 2003;35:472–9. Freedland SJ, Aronson WJ, Terris MK, et al. The percentage of prostate needle biopsy cores with carcinoma from the more involved side of the biopsy as a predictor of prostate specific antigen recurrence after radical prostatectomy: results from the Shared Equal Access Regional Cancer Hospital (SEARCH) database. Cancer 2003;98:2344–50. Kestin LL, Goldstein NS, Vicini FA, Martinez AA. Percentage of positive biopsy cores as predictor of clinical outcome in prostate cancer treated with radiotherapy. J Urol 2002;168:1994–9. 1322 european urology 52 (2007) 1309–1322 [91] Ravery V, Szabo J, Toublanc M, et al. A single positive prostate biopsy in six does not predict a low-volume prostate tumour. Br J Urol 1996;77:724–8. [92] Naya Y, Slaton JW, Troncoso P, Okihara K, Babaian RJ. Tumor length and location of cancer on biopsy predict for side specific extraprostatic cancer extension. J Urol 2004;171:1093–7. [93] Amin MB, Boccon-Gibod L, Egevad L, et al. Prognostic and predictive factors and reporting of prostate carcinoma in prostate needle biopsy specimens. Scan J Urol Nephrol Suppl 2005;216:20–33. [94] Emiliozzi P, Maymone S, Paterno A, et al. Increased accuracy of biopsy Gleason score obtained by extended needle biopsy. J Urol 2004;172:2224–6. [95] Coogan CL, Latchamsetty KC, Greenfield J, Corman JM, Lynch B, Porter CR. Increasing the number of biopsy cores improves the concordance of biopsy Gleason score to prostatectomy Gleason score. BJU Int 2005;96: 324–7. [96] Epstein JI, Walsh PC, Carmichael M, Brendler CB. Pathologic and clinical findings to predict tumor extent of nonpalpable (stage T1c) prostate cancer. JAMA 1994;271: 368–74. [97] Goto Y, Ohori M, Arakawa A, Kattan MW, Wheeler TM, Scardino PT. Distinguishing clinically important from unimportant prostate cancers before treat- [98] [99] [100] [101] [102] [103] ment: value of systematic biopsies. J Urol 1996;156: 1059–63. Carter HB, Sauvageot J, Walsh PC, Epstein JI. Prospective evaluation of men with stage T1C adenocarcinoma of the prostate. J Urol 1997;157:2206–9. Epstein JI, Chan DW, Sokoll LJ, et al. Nonpalpable stage T1c prostate cancer: prediction of insignificant disease using free/total prostate specific antigen levels and needle biopsy findings. J Urol 1998;160:2407–11. Kattan MW, Eastham JA, Wheeler TM, et al. Counseling men with prostate cancer: a nomogram for predicting the presence of small, moderately differentiated, confined tumors. J Urol 2003;170:1792–7. Ochiai A, Troncoso P, Chen ME, Lloreta J, Babaian RJ. The relationship between tumor volume and the number of positive cores in men undergoing multisite extended biopsy: implication for expectant management. J Urol 2005;174:2164–8. Augustin H, Hammerer PG, Graefen M, et al. Insignificant prostate cancer in radical prostatectomy specimen: time trends and preoperative prediction. Eur Urol 2003;43: 455–60. Miyake H, Sakai I, Harada K, Hara I, Eto H. Prediction of potentially insignificant prostate cancer in men undergoing radical prostatectomy for clinically organ-confined disease. Int J Urol 2005;12:270–4.