Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
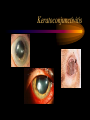
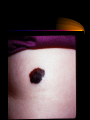
HEAD and NECK Dr Sham A. Cader Method Of Exam •Inspect the head for size •Feel for the skull for integrity and evenness •Evaluate the hair for texture and hair loss. •Inspect and palpate the scalp. Normal: •The head is symmetrical. Size varies with age and body stature. •Male pattern hair loss is common. •Minor undulations are normal for the skull. Author: A. Chandrasekhar Consultant: M. Massa Skin • Skin exam is not separate from the rest of the physical examination examine the patient in good lighting. • Inspect and palpate skin for the following: • Color: Contrast with color of mucous membrane. • Texture • Turgor: Lift a fold of skin and note the ease with which it moves (mobility) and the speed with which it returns into place • Moisture • Pigmentation • Lesions • Hair distribution • Warmth: Feel with back of your hand THE EYE • SYMPTOMS: • SUDDEN LOSS of VISION: Potential Causes • AMAUROSIS FUGAX: Temporary, monocular, ischemic blindness. Painless Caused buy ipsilateral Carotid stenosis or embolization of the retinal artery. • RETINAL DETACHMENT: Flashing lights, floating halos, and blurry vision before the blindness is indicative of retinal detachment. • UVEITIS: Inflammation of uveal tract -- iris, ciliary body, and choroid. Always painful.Associated with multiple diseases: connective tissue diseases, histoplasmosis, sarcoidosis, tuberculosis Uveitis GRADUAL LOSS of VISION • CATARACTS: Opacities of the lens, occurring with age. • GLAUCOMA: Increased intraocular pressure. It is the most common reason for loss of vision over age 50. • MACULAR DEGENERATION: Secondary to Diabetes, and expected to cause visual blindness. • Diabetic Retinopathy. • OPTIC NERVE COMPRESSION: Caused by an intracranial neoplasm, or pituitary adenoma. • OPTIC NEUROPATHY (Optic Neuritis): Multiple Sclerosis, and drugs such as Ethambutol, Methanol, can all cause optic neuritis and gradual blindness. • PRESBYOPIA: Gradual loss of ability of Accommodation for nearvision, occurring with age. • CORTICAL BLINDNESS: Infarct of the Occipital Lobe can lead to cortical blindness. Patient will have binocular blindness, but will retain the pupillary light reflex which is unaffected • DIPLOPIA: Double vision. • Monocular Diplopia: Should suggest corneal or lens problem. • Binocular Diplopia: Indicative of cranial nerve palsy or ocular muscle problems, or a brainstem problem. • Myasthenia Gravis (MG): Diplopia without pain is often the presenting complaint in MG EYE PAIN • The cornea is innervated by the Ophthalmic Nerve, CN V1. • Possible causes of eye pain • CNS problems affecting CN V1: Meningitis, cavernous sinus thrombosis, aneurysms, migraine • Adjacent structures: sinus problems • Eye problems / inflammations: Conjunctivitis, stye, chalazion • Photophobia: Eye pain upon exposure to light, indicative of • SCOTOMATA: Specific islands or spots of impaired vision; an impaired visual field. EYELIDS • PTOSIS: Droopy eyelids; failure of lids to open fully. Caused by failure of levator palpebrae, innervated by CN III, or failure of Tarsal Muscle, innervated by sympathetics. Some causes: Horner's Syndrome, Myasthenia Gravis, Encephalitis • LID LAG: Evidence of white sclera between the iris and upper lid margin. This is normally not found. It is a sign of Grave's Disease • STYE: Small abscess caused by infection of sebaceous glands of Zeis. • CHALAZION: Acute inflammation of the meibomian gland PTOSIS LID LAG STYE SCLERA • SCLERITIS: Inflammation of the sclera, visible as brown / red infiltrates in sclera on gross examination. Found in autoimmune and collagen vascular diseases, such as SLE, RA. • BLUE SCLERA: Pathognomonic of Osteogenesis Imperfecta. Results from very thin sclera in which the choroid shows through. • BROWN SCLERA: Found in disorder Alkaptonuria (metabolic disorder) • YELLOW SCLERA: Found in Jaundice. It should raise the question of liver disease or hemolytic anemia Scleritis EXOPHTHALMOS • Eyes jutting out past eyelids. A sign of Grave's disease, acromegaly, and cavernous sinus thrombosis CORNEA • KERATOCONJUNCTIVITIS (KERATITIS) SICCA: Found in Sjögren's Syndrome, resulting from autoantibodies against salivary glands resulting in no salivary secretion. • Classic triad of symptoms with Sjögren's Syndrome: • Keratitis Sicca (dry eyes) • Xerostomia (dry mouth) • Rheumatoid Arthritis Keratoconjunctivitis • INTERSTITIAL KERATITIS: A sign of congenital syphilis. • Hutchinson's Triad: Triad of interstitial keratitis, deafness, and notched teeth is classical evidence for congenital syphilis • ARCUS SENILIS: Gray band of opacity around the cornea. • KAYSER-FLEISCHER RINGS: Copper in Descemet's Membrane. • Circular bands of brownish pigment on lateral and medial margins of cornea. • Found in Wilson's Disease • PINGUECULAE: Small, yellowish elevations of the conjunctivae, which appear brown in Gaucher's disease. It is caused by hyaline degeneration of conjunctival tissue. • ANISOCORIA: Unequal pupils, caused by miosis or mydriasis of one pupil PUPILS • MARCUS GUNN PUPIL: A pupil that dilates (rather than constricts) as light swings toward it. • It indicates either severe macular disease or optic nerve disease in the affected eye. • PUPILLARY REFLEXES: • Absent Direct Reflex: Indicates a problem with the afferent branch (Trigeminal V1) of the reflex. • Absent Consensual Reflex: Indicates a problem with the efferent branch (CN III, Edinger-Westphal Nucleus) of the affected eye. • CONVERGENCE: Ability of eyes to focus inward and accommodate for near vision. • Impaired convergence is seen with Grave's Disease. • ARGYLL ROBERTSON PUPIL: Indicates a form of CNS Syphilis, Tabes Dorsalis. • Weak or absent direct pupillary reflex. • Normal response to accommodation. • Failure of pupillary dilation with painful stimulation or after atropine administration. • ADIE'S PUPIL: Similar to Argyll Robertson Pupil. • Weak or absent direct pupillary reflex. • Impaired or absent accommodation. • Eye appears larger than the other eye on inspection • MYDRIASIS: Abnormal dilation of pupil, can occur in Diabetes. • MIOSIS: Abnormal constriction of pupil, seen in Horner's syndrome. • HORNER'S SYNDROME: Lost sympathetics from the Superior Cervical Plexus. Ptosis, Miosis, Anhydrosis. • NYSTAGMUS: Nystagmus is normal when looking in the periphery for extended times. All other nystagmus is abnormal. • Causes: Labyrinthitis, MS, WernickeKorsakoff, Meniere's Disease THE EAR • TINNITUS: Ringing in ear. • VERTIGO: • Objective Vertigo: The earth is moving around you. • Subjective Vertigo: You are moving in space. NOSE and THROAT • EPISTAXIS: Bloody nose. • Transient Epistaxis: May occur with forceful nose-blowing, sneezing, nose-picking, facial trauma. • Recurrent Epistaxis: Differential diagnosis = hypertension, coagulopathies, renal failure, cirrhosis, hereditary hemorrhagic telangiectasia. • RHINOPHYMA: Severe acne rosacea found in association with skin hypertrophy and congestion of subcutaneous tissue, around the nose. Mouth • Inspect lips: angle of mouth for color and moisture • Teeth: Inspect the number condition of the teeth • Observe the gums for color swelling and tenderness • Inspect the roof of mouth for color architecture of hard palate Proceed with the exam by using a wooden tongue blade and penlight Parotid gland • Inspect the pre- and infra-auricular region, observing for symmetry. • Palpate the parotid gland Lacrimal gland • Have the patient close their eyes and observe the upper and outer aspect of the upper lid. • The lid is normally smooth and symmetrical. • Gently retract the upper lid and have the patient gaze to the opposite side. • The lacrimal gland is located under the lid near the outer angle. Submandibular gland • Observe the submandibular region. • Tilt the patient's head forward and gently roll your fingers over the inner surface of the mandible THROAT • SOAR THROAT: Infection mononucleosis, strep-throat (streptococcal pharyngitis). • HOARSENESS: Larynigitis, Laryngeal cancer, hypothyroidism, smoking ------> broncho-genic carcinoma • ABNORMAL TASTE: • Hypoguesia: Impaired ability to taste. Seen in URI's, glossitis, stomatitis. • Dysguesia: Unpleasant taste. Differential diagnosis: • Medications: metronidazole, Vitamin and mineral deficiencies: zinc depletion ,Chyronic hypercalcemia, hyperparathyroidism. • Viral hepatitis TONGUE • MACROGLOSSIA: Large tongue can occur with amyloidosis and acromegaly. • GLOSSITIS: Inflammation on sides, base, and underside of tongue. • Vitamin and mineral deficincies • Medications: metronidazole, phenytoin • Infections: candidiasis • Pernicious Anemia • Cytotoxic drugs, radiotherapy Tonsils Thyroid Gland Thyroid Gland • Inspect the neck for fullness over the thyroid region. • While standing behind the patient, affix the trachea on one side, gently tilt the head and roll the thyroid gland over the tracheal rings. • Repeat this procedure on the opposite side. • Ask the patient to swallow water, extend the neck gently and observe the mobility of the thyroid gland while swallowing. • Palpate the thyroid gland while swallowing, separately examining each lateral lobe and the isthmus • Some prefer to examine the thyroid from the front. • Evaluate Thyroid gland for consistency, tenderness, size and approximate weight • The Thyroid gland is palpable and rises along with thyroid and cricoid cartilage during swallowing, in persons with a slender neck. • It is soft and approximately weighs no more than 20 grams. • It is often not palpable with aging GOITER • Goiter refers to any enlargement of the thyroid gland. Because of the gland's location at the front of the neck, this condition becomes visually apparent • Diffuse goiter refers to a uniformly enlarged thyroid. It is associated with disease processes (for example, Hashimoto's and Grave' diseases) and is endemic to areas in the world where the diet is iodine deficient. In such areas, goiter can become quite large, appearing as a huge, bizarre growth hanging down from below the chin. Diffuse goiter is a consequence of stimulation of the thyroid to hypertrophy and hyperplasia • The cause of lumpy or nodular goiter is not well understood. Nodules raise concerns about thyroid cancer (see below), and those that are hot or autonomously functioning are of concern because they may eventually cause hyperthyroidism HYPOTHYROIDISM (Myxedema • Hypothyroidism refers to clinical status when thyroid hormone concentrations are below the euthyroid (eu- meaning normal) range. Symptoms may include goiter (enlarged thyroid), fatigue cold intolerance, weight gain, constipation, dry skin, puffy face, depression, and loss of hair. Severe manifestations may include hypothermia, seizures, stupor, and coma. Primary Hypothyroidism • In primary hypothyroidism, the disorder is at the site of the thyroid gland itself. Primary hypothyroidism may be acquired or congenital • The most common cause of acquired hypothyroidism is Hashimoto's thyroiditis. • Other causes of acquired hypothyroidism include thyroid ablation, antithyroid drugs administration, and iodine deficiency Secondary and tertiary hypothyroidism • Secondary and tertiary hypothyroidism are rare diseases. In secondary hypothyroidism, a pituitary lesion impairs production of TSH • In tertiary hypothyroidism, a lesion in the hypothalamus causes inadequate production of TRH. In the absence of adequate TRH stimulation, pituitary production of TSH is inhibited which, in turn, inhibits production of thyroid hormones by the thyroid. HYPERTHYROIDISM • Hyperthyroidism refers to clinical status in which thyroid hormone concentrations are above the euthyroid (eu meaning normal) range. Symptoms may include goiter, nervousness and irritability, heat intolerance, cardiac arrhythmias, tremors, exophthalmos (bulging eyes), and mental disturbances. • The most common cause of hyperthyroidism is Graves' disease • Graves' disease afflicts approximately 1 million patients in the United States • The disease is caused by autoantibodies directed against TSH receptors on the surface of thyroid cells toxic nodular goiter • In toxic nodular goiter, another hyperthyroid condition, discrete portions of the thyroid (nodules), for reasons that are not well understood, are no longer under normal feedback control and secrete excess amounts of thyroid hormone. This condition occurs more frequently in elderly patients and, in contrast to Graves' disease, is not accompanied by ophthalmopathy Lymph Nodes: Cervical • For palpation o fpreauricular nodes, roll your finger in front of the ear, against the maxilla Sub occipital lymph nodes • are palpable immediately behind the ear. Posterior cervical • Posterior cervical nodes are behind sternomastoid and in front of Trapezius. Sub maxillaryand Submental • Roll your fingers against inner surface of Mandible with patient's head gently tilted towards one side Deep cervical lymph nodes • should be palpated, one side at a time. Gently bend the patient's head forward and roll your fingers over the deeper muscles along the carotid arteries. Scalene nodes • roll your fingers gently behind the clavicles. Instruct the patient to cough or to bear down like they are having a bowel movement. Occasionally an enlarged lymph node may pop up External Ear • Inspect and feel the external ears. • Examine skin over External Ear • Note the size, color, position of ear lobes, contour and texture of the cartilage and soft tissue. • Note tenderness on movement of ear lobes • The cartilage is firm in texture and movable. Be aware of changes secondary to ear piercing effects based on culture and ethnic habits. Hearing • With eyes closed, the patient should be instructed to acknowledge hearing the gentle rubbing of the examiner's fingers approximately 3-4 inches away from his right and left ear. • A watch, which the examiner can hear at a specific distance from his ear, is placed next to the patient's ear. Ask him to note when the watch sound disappears. Note that the examiner has to have normal hearing to do this exam (in at least one ear). QUIZ Herpes Zoster