Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
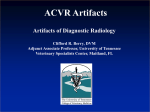
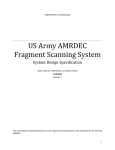
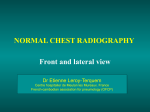
Chapter 2 General Screen Film Radiography and Its Limitations X-rays have been in use for over a century since the report of their discovery by Röentgen (1896). In the health and medical areas, x-rays have been used for both diagnosis and treatment of patients’ conditions. In diagnostic medical imaging (radiography), x-rays are used in a wide variety of examinations. Examples of medical imaging examinations can be found in Table 2.1. Table 2.1 Types of medical imaging examinations using x-rays as the energy source (Ballinger, 1991; Fauber, 2000; Gunn, 2002) general radiography – single projection images fluoroscopy – single projection imaging to display function or anatomical motion angiography – a rapid series of single projection images to capture motion of blood flow computed tomography (CT) – multiple projection imaging to display a cross-section of the anatomy bone mineral densitometry (BMD) – analysis of the bone strength. X-rays are electromagnetic (EM) radiation with characteristics of short wavelengths, very high frequencies and very high energy. High energy EM radiation exhibits characteristics of both waves and discrete bundles of energy called photons. X-ray photon energy is usually measured in kilo-electron volts (keV) and diagnostic x-ray energies are typically 10 to 150 keV. Such high energy EM radiation is ionising. Ionising radiation has potential harmful effects when it irradiates human tissue (Bushberg et al, 2002; Curry et al, 1990; Graham & Cloke, 2003). In diagnostic medical imaging, x-ray production and its attenuation in matter is well described by Bushberg et al, (2002), Bushong (2001), Curry et al (1990), Dowsett, Kenny & Johnston (1998), Graham & Cloke, (2003), Thompson et al (1994) and 5 Webb (1988). An important consideration for this project is that a heterogeneous intensity x-ray beam results from differential attenuation within the patient’s anatomy. The exit intensities of the x-ray photons will depend on the properties of the body within the irradiated area and the characteristics of the x-ray beam. The mechanisms that result in reduction of x-ray intensities are the types of interaction with matter, such as the photoelectric effect and Compton scatter. Exit intensity of the x-ray beam can be considered as a function of the probability that an x-ray photon will have an attenuating event. Properties of the body that affect attenuation are effective atomic number of the anatomical material, electron density of the anatomical material, and thickness of the anatomical area or the distance the x-ray photons travel through anatomy. As the effective atomic number of the tissue increases, the probability of an interaction of the x-ray photon with the anatomy increases; as electron density of the anatomy increases, the probability of an interaction of the x-ray photon with the anatomy increases; and as the x-ray photon’s path distance through the body increases, the probability of an interaction of the x-ray photon with the anatomy increases. The degree of attenuation is also affected by the energy of the photons of the entrance x-ray beam. As x-ray photon energy increases, the probability of an interaction of the x-ray photons with the anatomy decreases (Bushberg et al, 2002; Curry et al, 1990; Graham & Cloke, 2003). X-ray beams are comprised of photons of many different energies, and as such are polyenergetic. A characteristic of an x-ray beam that affects the rate of attenuation, and hence the exit intensity of the beam, is its effective energy. Effective energy of the x-ray beam can be considered as the weighted mean of the x-ray photon energies within the beam (Bushberg et al, 2002; Carlsson & Carlsson, 1984). A common means of measurement of the effective energy of the x-ray beam is the measurement of the half value thickness (HVT) of the material that is irradiated. The HVT is the thickness of the material irradiated that reduces the intensity of the exit x-ray beam to half of its entrance intensity. Common materials used for the measurement of effective energy of an x-ray beam are aluminium (Al) and copper (Cu). HVT, at diagnostic x-ray energies, is typically stated in millimetres of Al or Cu (Bushberg et al, 2002; Carlsson & Carlsson, 1984). 6 Attenuation of polyenergetic x-ray beams can then be considered as a function of their effective energy or HVT. As the effective energy of x-ray beams increases, the probability of interactions of the x-ray photons decreases. A higher effective energy x-ray beam will result in a higher exit intensity than when the effective energy of the entrance beam is lower. Subject contrast is the differences in exit intensities of the x-ray beam, within the irradiated field, that result from different rates of attenuation within the irradiated body. Large subject contrast results from large differences in attenuation rates. Large subject contrast will typically result from a low effective energy beam as well as large differences in attenuation (Bushong, 2001; Fauber, 2000; Gunn, 2002). Subject contrast produces differences in optical densities that can be visualised within the resulting image. Optical density differences are known as radiographic or image contrast. The degree of radiographic contrast depends on the subject contrast and also depends on factors within the image receptor (Fauber, 2000; Gunn, 2002; Thompson et al, 1994). 2.1 Filtration and Shaping of the X-ray Beam Polyenergetic x-ray beams used in medical imaging have a maximum photon energy, which corresponds to the peak kilovoltage (kVp) applied across the x-ray tube. The kVp is determined by the radiographer, depending upon the desired characteristics of the radiographic image. A polyenergetic x-ray beam produced within the x-ray tube anode has a low number of high energy photons and there are an increasing number of photons at each energy level as the photon energy decreases from the maximum energy. This is depicted graphically as the dashed line in Figure 2.1 (Curry et al, 1990). In Figure 2.1, the maximum photon energy is 150 keV which results from setting 150 kVp across the x-ray tube. 7 Figure 2.1 Typical energy spectrum of a 150kVp x-ray beam (Curry et al, 1990, p.33) Filtration is the removal of x-ray photons from the beam by attenuation when the beam is passed through a medium (Bushberg et al, 2002; Curry et al, 1990; Thompson et al, 1994). There are two types of general filtration: inherent and added filtration. X-ray photons are produced by interaction of an accelerated electron with a target atom. The atoms producing the x-ray photons are often at depth within the target. As the photons travel within the target itself, attenuation can occur. As the photons travel further through the x-ray tube, attenuation can again occur within the glass of the x-ray tube, within the cooling oil that surrounds the glass x-ray tube and within other parts of the x-ray tube housing and collimator. This is the process of inherent filtration. Lower energy photons have a high probability of attenuation. Photons with energies below 15 keV are fully attenuated by the x-ray tube’s inherent filtration (Bushberg et al, 2002; Curry et al, 1990; Graham & Cloke, 2003; Thompson et al, 1994). The solid line in Figure 2.1 depicts a typical shape of the x-ray spectrum following inherent filtration of the Bremsstrahlung and characteristic radiation. 8 Added filtration is the addition of other material in the path of the x-ray beam prior to the x-ray beam entering the patient’s anatomy. The prime purpose of added filtration is the further removal of low energy photons from the x-ray beam. The effect of added filtration on the shape of the x-ray spectrum can be seen in Figure 2.2 (Curry et al, 1990). Low energy photons, if allowed to enter the patient’s body, would have a high probability of being fully attenuated by the anatomy and hence increasing the absorbed dose to the patient without contributing to the image (Bushberg et al, 2002; Curry et al, 1990; Thompson et al, 1994). Figure 2.2 X-ray spectra at 90kVp with added filtration (filtered) and without added filtration (unfiltered) (Curry et al, 1990, p.89) Added filtration will remove more lower energy photons from the beam than higher energy photons. Added filtration assists in lowering the patient absorbed dose. Another effect of placing added filtration in the path of the x-ray beam is that of shifting the effective energy of the beam. In Figure 2.2 it can be seen that the addition of filtration to the beam has increased the effective energy of the beam. Added filtration can be any material that is placed in the path of the x-ray beam. It is usually measured in equivalent thickness of aluminium. When the prime purpose is 9 dose reduction, added filtration material is of uniform thickness across the entire x-ray field. Minimum amounts of added filtration are usually regulated by statutory authorities. In Australia, these standards are regulated by various state Acts and Regulations such as the New South Wales Radiation Control Act (NSW) (1990), the Radiation Control Regulation (NSW) (2003) and the Radiation Guidelines 6 (2004). Aluminium and copper are the most common added filtration material (Bushberg et al, 2002; Curry et al, 1990; Thompson et al, 1994). Typical thicknesses of added filtration material in diagnostic radiography are 2 – 3 mm of Al or 0.1 mm of Cu (Carlsson & Carlsson, 1996). The use of erbium filter material has been reported by Chakera et al (1982), Shrimpton et al (1988) and Cranage et al (1992). Other authors (Koedooder & Venema, 1986; MacDonald-Jankowski & Lawinski, 1992; Regano & Sutton, 1992; Sanborg et al, 1993; Tapiovaara et al, 1999; Villegran et al, 1978) have reported on the use of other filtration material in medical x-ray use such as samarium (Sm), gadolinium (Gd), holmium (Ho), ytterbium (Yb), tungsten (W), yttrium (Y), niobium (Nb) and other metals and materials. Different filter materials attenuate the x-ray beam in different manners and hence produce different dose rates to the patient. The prime purpose of many authors (Chakera et al, 1982; Kohn et al, 1988; MacDonald-Jankowski & Lawinski, 1992; Regano & Sutton, 1992; Sanborg et al, 1993; Shrimpton et al, 1988) has been to document the improved dose reduction when particular filter materials are placed in the x-ray beam. The choice of filtration material can have effects other than dose reduction in medical imaging. Kohn et al (1988) used five radiologists to compare image quality when different filter materials were used in the x-ray beam. The radiologists found no difference in image quality of skull images when Al, Cu and Y filter material were used. The radiologists preferred images of the hands when Al was the filter material used. Image contrast was reduced when Cu filter material was used in paediatric barium examinations (Hansson et al, 1997). In low kVp dental radiographic examinations reported by Shibuya et al (2000), filter materials of Al, Nb, Gd and a composite material of Cu, Al and tin were used. In this case, the composite material improved diagnostic performance over the other filter materials. 10 Williamson et al (1994) reported on the use of K-edge filtration materials, where the binding energy of the K-edge was within the diagnostic medical imaging range of energies, between 17 and 68keV. One of the conclusions drawn by Williamson et al (1994) was that reduced image contrast occurred when K-edge filters were used compared to when Al filters were used. 2.2 Film/Screen Radiography X-ray intensities that exit the body are recorded for viewing and storage. In general radiography, the x-ray image may be recorded using a variety of means. The type of general radiography is named after the recording media used. The types of general radiography are listed in Table 2.2. Table 2.2 Types of general radiography recording media (Bushberg et al, 2002; Bushong, 2001; Gunn, 2002) film/screen (F/S) radiography using film and intensifying screens digital radiography (DR) such as: computed radiography (CR) using photostimulable phosphors flat panel systems such as: direct radiography using photoconductor material with thin film transistors indirect radiography using intensifying screens and detectors. Material that fluoresces under irradiation from x-rays was first noted by Röentgen (1896). Intensifying screens for use with film as a joint recording medium were first designed by Thomas Edison (Thompson et al, 1994). The purpose of the intensifying screen is to convert the x-ray energy to light. The use of intensifying screens increases the efficiency of exposure of the film over exposure directly by the x-ray beam. The use of intensifying screens decreases the absorbed dose received by the patient compared to x-rays directly exposing the film. Films are typically exposed by 95 – 99% light and 1 – 5% x-ray photons when intensifying screens are used. A measure of the screen’s efficiency is its intensifying factor (IF). IF is a comparison of exposures with and without the use of intensifying screens to achieve the same 11 optical density on the film (Bushong, 2001; Curry et al, 1990; Fauber, 2000; Thompson et al, 1994 ). Many different fluorescent materials have been used in intensifying screens. Different materials fluoresce at different wavelengths of light. Examples of some fluorescent materials and their spectral emission used in intensifying screens are:• calcium tungstate (CaWO4) – blue light (peak response ≈ 420nm); • gadolinium oxysulphide: terbium activated (Gd2O2S:Tb) – green light (peak response ≈ 550nm); • lanthanum oxybromide: thulium activated (LaOBr:Tm) – blue light (peak response ≈ 380 to 420nm). (Bushberg et al, 2002; Curry et al, 1990; Graham, 2003) X-ray films are designed to be sensitive to the specific spectral emission of a given intensifying screen. Consequently, films and screens are matched for optimised efficiency of conversion of x-ray photons to optical densities on the film. The F/S combinations can exhibit different characteristics of conversion efficiency (speed), spatial resolution or detail visualised in the image. It is generally accepted that high speed F/S combinations will result in lower spatial resolution. The use of a higher spatial resolution and lower speed F/S combination will result in a high absorbed dose to the patient (Bushong, 2001; Fauber, 2000; Gunn, 2002; Thompson et al, 1994). Optical density (OD) is a logarithm of the ratio of the amount of incident light to the transmitted light through the x-ray film when viewing the image. OD measurements on x-ray film range between the base fog of the film, typically an OD of 0.2, to the maximum density of the film, Dmax, at a typical OD of 3.5 to 4. When the number of x-ray photons reaching the F/S is high, the OD is high. When there has been no x-ray exposure to the F/S, the OD measured is that of the base fog of the film. High speed F/S combinations require fewer x-ray photons to achieve the same OD as lower speed F/S combinations (Fauber, 2000; Gunn, 2002). 12 The OD at a specific point on the film is dependant upon several factors. These factors are the initial number of photons produced in the x-ray tube, loosely referred to as exposure; the amount of attenuation of the x-ray beam as it travels through the body; the F/S speed; and the film processing (Fauber, 2000; Gunn, 2002; Thompson et al, 1994). Another characteristic of F/S combinations is F/S latitude. Latitude is the range of relative exposures required to produce a range of OD. The range of OD is usually between values of 0.25 and 2.0. Figure 2.3 (Curry et al, 1990, p.159) shows plots of OD resulting from various exposures reaching the F/S. If a small range of exposures produces these ODs, the latitude is said to be narrow (Figure 2.3 a.). If a larger range of exposure produces the same ODs, the latitude is said to be wide or broad (Figure 2.3 b.). Figure 2.3 Characteristic curves showing: a. Narrow latitude; b. Wide latitude (Curry et al, 1990, p.159) The dynamic range of an x-ray film is equivalent to the film’s latitude. The range of OD on an x-ray film, typically 0.25 to 3.0, is equivalent to a dynamic range of 1:100 (Dowsett et al, 1998). The effective energy of the x-ray beam can also affect film latitude. An increase of effective energy of the beam, either through increasing the kVp or through the 13 addition of filtration to the beam, will increase the latitude (Bushberg et al, 2002; Curry et al, 1990; Fauber, 2000; Gunn, 2002). 2.3 Radiographic Contrast Radiographic contrast is a measure of the difference between the OD of one region in the image and the OD of another region. Radiographic contrast can be measured objectively through the use of densitometers, which measure OD at a point on the x-ray film. Measurement of two ODs at different points on a film will provide a measurement of radiographic contrast. Radiographic contrast can also be assessed subjectively. When an x-ray image comprises mainly areas of high OD (black) and low OD (white), it is referred to as exhibiting high radiographic contrast. When the image has a broad range of OD, typified by the highest OD not being black and lowest OD not being white, it is referred to as exhibiting low radiographic contrast or wide latitude. Radiographic contrast is directly proportional to the angle, γ, of the straight line regions of the characteristic curve of the F/S (Bushberg et al, 2002; Fauber, 2000; Gunn, 2002). Comparison of angles of the straight line of the F/S characteristic curves can be seen in Figure 2.3. Figure 2.3a has a high γ and high radiographic contrast, whereas Figure 2.3b has a low γ and low radiographic contrast. Figure 2.4 shows a comparison of high and low radiographic contrast images. The image in Figure 2.4a has an appearance of strong blacks and whites. It exhibits high radiographic contrast. The bones of the feet are better visualised in this image than in Figure 2.4b. Figure 2.4b exhibits low radiographic contrast. This image displays the soft tissue regions such as muscles better than Figure 2.4a (Bushong, 2001; Fauber, 2000; Gunn, 2002). 14 Figure 2.4 Radiographic images with: a. High radiographic contrast b. Low radiographic contrast Radiographic contrast within the image results from the variable attenuation of the x-ray beam and from the latitude. High radiographic contrast occurs when there are large differences in attenuation within the x-ray field and/or there is a narrow F/S latitude or dynamic range and/or there is a low effective x-ray beam energy. Low radiographic contrast or wide latitude occurs when there are small differences in attenuation within the x-ray field and/or there is a wide F/S latitude or dynamic range and/or there is a high effective x-ray beam energy. A low or high effective x-ray beam energy is set by radiographers as either a low or a high kVp setting. The amount of added filtration is usually constant within the x-ray tube and as such is not usually considered to have an effect on radiographic contrast (Bushong, 2001; Fauber, 2000; Gunn, 2002). It is a general principle in radiography to maximise radiographic contrast for most radiographic examinations. Bones are better visualised with high radiographic 15 contrast images. Soft tissue examinations and chest radiographic examinations are exceptions to this general rule. High latitude films and/or high kVp techniques are often used in the radiographic examination of the chest. Soft tissue such as muscle has inherent low attenuation differences and hence has low subject contrast within the tissue. Radiographic contrast is still maximised for soft tissue radiographic examinations. Low radiographic contrast images will result from imaging soft tissue anatomical regions (Bushong, 2001; Fauber, 2000; Gunn, 2002). Radiographic contrast within the image is optimised so as to display the desired anatomical area under examination. Optimisation is effected through the radiographer’s selection of appropriate exposure factors such as the kVp and F/S combination. 2.4 Limitations of Film/Screen Radiography The dynamic range of a medical imaging system is the system’s ability to record the signal and represent the anatomical detail. In general radiography, the signal is the radiation that exits the body. The dynamic range will depend upon attenuation characteristics of the body. In some instances the F/S recording devices may have a narrower dynamic range than that of the exit radiation (Dowsett et al, 1998). In F/S general radiography, radiographers must choose the desired contrast appearance of the radiographic image. Radiographers may produce a radiographic image with high contrast or a radiographic image with low contrast. Radiographers can not produce a single image that demonstrates both high and low radiographic contrast at the same time. Two radiographic exposures on two films must be made to achieve an examination that has both high and low radiographic contrast or wide latitude. X-ray photon intensities or exposures that exit the anatomy must fall on the linear region of the F/S characteristic curve. The linear region of the F/S characteristic curve is shown in Figure 2.3 and is typically between OD values of 0.5 to 2.0. The linear region of the F/S characteristic curve is effectively the dynamic range of the 16 F/S system. If x-ray exit intensities are outside this latitude or dynamic range, any change in exposure will not result in a proportional change of OD that could be visualised on the film. Many regions of the body have areas that have both very high and very low attenuation within a single x-ray field. Examples of such regions of the body are the chest, where the lungs have low attenuation and the thoracic spine has relatively high attenuation and the shoulder where peripheral regions have lower attenuation. Such anatomical areas have a high dynamic range of exit x-ray intensities. When a low effective energy (low kVp) x-ray beam is used, the difference in attenuation within these areas is accentuated, and a very high radiographic contrast image will result. If the exit beams that emerge from two or more regions are above the exposure required to produce the Dmax of the image these regions will appear black on the image. In this example, the exit intensities are above the dynamic range of the F/S system. A linear increase in exposure will not result in a corresponding linear increase in OD. No radiographic contrast difference between these regions will be visualised and as such these areas will be indistinguishable. Similarly, if two or more regions attenuate the beam so that no x-ray photons exit, the regions appear white and are indistinguishable. This occurs even if the anatomical regions have different levels of attenuation characteristics. Here the exit intensities are below the dynamic range of the F/S system. The usual solution to this problem in radiography is to increase the effective energy of the beam. Radiographers increase kVp to increase the so-called penetration of the beam. As kVp is increased there is a corresponding increase of the x-ray beam’s effective energy. As the effective energy of the x-ray beam is increased there is a decrease in attenuation of the beam and an increase in intensity of the exit beam. The dynamic range of the exit radiation is reduced. The advantage of this method is that latitude is increased and all anatomy is visualised in one image. The γ of the F/S system is decreased and the linear response region of the characteristic curve is increased. The disadvantage is that radiographic contrast will decrease across all anatomy visualised in the image. The general principle of maximising radiographic contrast has been upheld. An alternative method could be to undertake two radiographic exposures to optimise radiographic contrast across all anatomy within 17 the field of interest. This approach is not generally undertaken as it requires two exposures of ionising radiation and an increase in absorbed dose by the patient. There are many anatomical regions of the body where large attenuation differences occur or where there is a wide dynamic range within the x-ray field. Some examples are provided in Table 2.3. Table 2.3 Examples of regions where wide dynamic ranges exist within the anatomy (Ballinger, 1991) Anatomical Explanation of Wide Dynamic Range Region chest large attenuation differences between the air-filled lungs and the thoracic spine thoracic spine large anatomical thickness differences between the superior and inferior portions of the thoracic spine shoulder large anatomical thickness differences between the edges of the shoulder and the chest region within the image facial bone lateral image required to display both soft tissue and bony anatomy cervical spine lateral image required to display both the cervical vertebra and the cervico-thoracic junction – large attenuating differences between the cervical vertebra and the cervico-thoracic junction regions cervical spine lateral image required to display both soft tissue and bony anatomy thoraco-lumbar lateral image required to display both the thoracic and the lumbar spine spine hip / neck of cross-table lateral used – large attenuation differences between the femur pelvic region and the neck of femur within the image femur large anatomical thickness differences between the superior and inferior regions of the femur feet anatomical thickness differences between the tarsal region and the metatarsal/phalanges of the foot hands lateral image required to display both the metacarpals and the phalanges abdomen horizontal ray required to show air/fluid differences – attenuation differences are further increased when barium is introduced to outline the gut 18 2.5 Shaped Tissue Compensation Filters Filtration material that is non-uniform in thickness may be placed in the x-ray beam to compensate for the varying degrees of attenuation of the anatomy within the irradiated area (Bushong, 2001; Curry et al, 1990; Thompson et al, 1994). Curry et al (1990) describe the use of a wedge shaped filter material. Wedge shaped filters are occasionally used to obtain radiographic images of more uniform optical density when a part being examined diminishes greatly in thickness from one side of the x-ray field to the other. (Curry et al, 1990) According to Bushong (2001), one of the most difficult tasks facing the radiographer is to produce an image with a uniform optical density when examining a body part that varies greatly in thickness or tissue composition. Bushong recommends the use of a compensating filter when this occurs. A trough shaped filter is recommended for chest radiographic examinations and a wedge shaped filter for examinations of the feet. Thompson et al (1994) recommend the use of compensating filters when there are large differences in tissue density within the anatomical region and the goal is to visualise the entire structure without making additional exposures. They describe the use of wedge filters and trough filters. Figure 2.5 shows sectional planes through tissue compensation filters (TCFs) and their relationship to the x-ray beam and the anatomy. 19 Figure 2.5 Cross-sections through wedge and trough TCFs (Thompson et al, 1994) Other authors discuss various other uses and shapes of TCFs. Feczko et al (1983) used various shaped filters in horizontal-beam lateral decubitus radiograph examinations of barium filled abdomens. They (1983) performed 30 examinations, of which 28 showed marked quality improvement through the use of TCFs. The shapes of the TCFs used are shown in Figure 2.6. Crow, Guinto & Segura (1983) examined the use of TCFs to compensate for thinner anatomical regions when undertaking arch aortograms. TCFs have been reported to improve the quality of radiographs of the shoulder (Vezina, 1985). Gray, Hoffman & Peterson (1983) and Butler et al (1986) have reported on the use of TCF in radiographic examinations of the scoliotic spine. A single exposure was used to obtain excellent quality radiographs of the lower leg using a TCF (Petersen & Rohr, 1987). Marugg et al (1990) designed a holder to allow the use of multiple TCFs during one radiographic examination. 20 Figure 2.6 Cross-sections through tissue compensation filters used for horizontal-ray barium examinations (Feczko et al, 1983, p.849) TCFs have proved to be useful devices to assist in overcoming the F/S limitation where large subject attenuation differences exist within the irradiated field. The insertion of a varying thickness TCF into the x-ray beam attenuates the beam by different amounts within the field. There is an assumption that, prior to entering the anatomy, the x-ray beam is uniform in intensity across the field. Insertion of the TCF into the entrance beam alters the intensities across the field. The TCF modifies the intensities within the entrance beam so that the exit beam has a reduced dynamic range. The result is that the exit beam is more uniform or has a narrower dynamic range whilst still containing exit intensity differences so that OD differences exist within the image. TCF sizes and shapes are predetermined. Radiographers select the most appropriate size and shape for a particular radiographic examination and patient shape, from a limited range. Modification to the TCF size and shape can not be made easily. Goodsitt et al (1998) examined TCF use in mammography. Their object was to develop a range of TCF shapes to suit individual breast shapes. They concluded that three or four TCF shapes would be needed to match the contour shape of the 21 compressed breast for all mammography examinations. Mammography radiographers would then be able to select the most appropriate TCF shape for individual mammography examinations. The advantage of using a TCF in F/S radiography where there are anatomical regions with large attenuation differences within the x-ray field, is that all of the anatomy can be visualised with only one exposure of ionising radiation to the patient. Radiographers can select an appropriate kVp to optimise radiographic contrast without the concern of under- or over-exposing areas of anatomy within the x-ray field. Radiographic contrast is maximised over the entire image whilst still enabling all anatomy to be visualised. Radiographic image optimisation is generally within a radiographer’s autonomous duties, and the appropriate use of TCFs in the radiographic examination is part of image optimisation. Selection of the appropriately shaped TCF and precise placement of the TCF within the beam are judgement issues of the radiographer performing the radiographic examination. 2.6 Computed Radiography Computed radiography (CR), as an alternative to screen-film general radiography, is another means of image capture, storage and display in diagnostic radiography. The first CR system was announced by the Fuji Photo Film Company in 1981 (Schaetzing et al, 1990). Since then such systems have been manufactured and marketed by a number of different companies. There are many advantages and disadvantages between CR and F/S. These are discussed in detail in Chapter 4. Computed radiography uses photostimulable phosphors (PSPs) to capture a latent image on the imaging plate. PSPs are barium fluorohalides activated with europium (BaFX:Eu2+ where the halide X is typically bromine or iodine). X-ray photon energy ionises the Eu atoms and the free electrons become trapped in so called F-centres. During reading out of the image, a red laser scans and exposes the imaging plate. The photon energy of the red laser light is absorbed by the F-centres, allowing the trapped 22 electron to become mobile and reabsorbed by the Eu atoms. During this deexcitation, energy is released in the form of blue-green light. A picture element or pixel is a quantised value that represents a small area at location (x, y) in a digital image (Baxes, 1994; Jain, 1989). The intensity of the blue green light is recorded and converted to a pixel value. The resulting CR image is comprised of multiple rows and columns of pixels representing the x-ray photon intensities at locations (x, y) (Bushberg et al, 2002; Bushong, 2001; Dowsett et al, 1998; Weiser, 1997). One advantage of CR over F/S is the increased dynamic range of CR images (Balter, 1990; MacMahon & Vyborny, 1994; Schaetzing et al, 1990; Siebert, Shelton & Moore, 1996; Weiser, 1997). Dynamic range in CR is equivalent to F/S exposure latitude. Figure 2.7 (Bushberg et al, 2002) provides a comparison of the dynamic ranges of CR and typical F/S exposure latitude. CR is linear to x-ray exposure over a greater range of exposures than is F/S. CR has a resulting increased exposure latitude or dynamic range over F/S. A typical dynamic range of the imaging plate used in CR to capture the image is 1,000:1 (Vuylsteke & Schoeters, 1994). Radiographic contrast in F/S is limited by the exposure latitude. High radiographic contrast results when the exposure latitude is narrow. The greater dynamic range of CR allows x-ray photon exit intensities from high or low attenuating anatomical regions, which could fall outside the exposure latitude of F/S, to be recorded. In Figure 2.7, exposures of 0.01 and 0.1 would result in the same OD (white) using an F/S combination. Using these exposures in CR, differences in CR signal exist and OD differences can be visualised that would not be visualised using F/S. Viewers of CR images can take advantage of CR’s greater dynamic range through manipulation of the displayed brightness and contrast of the image. Look-up tables (LUTs) are means of controlling the displayed brightness and contrast of digital images (Artz, 1997; Baxes, 1994; Freedman & Artz, 1997b). The image pixel values are converted through the LUT to display values visualised on the computer monitor. CR images can be displayed with a broad or narrow displayed contrast. Narrow displayed contrast images are similar in appearance to a narrow radiographic contrast in F/S radiographic imaging. Broad displayed contrast images are similar in appearance to a wide radiographic contrast in F/S radiographic imaging. 23 Figure 2.7 Dynamic range of CR vs exposure latitude of F/S (Bushberg et al, 2002, p.296) Where there are anatomical regions with large attenuation differences within the x-ray field, the advantage of CR over F/S is that all of the anatomy can be visualised with one exposure of ionising radiation to the patient. The displayed CR image can then be adjusted to optimise the displayed brightness and contrast of individual anatomical regions within the image. 24