Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Physiology lec43 (3-5-2011)
Cont. Eye II
Last time we started talking about light and dark adaptation.
During light, pigment is decomposed, so the quantity of pigment will decrease
that will decrease the retinal sensitivity. (Because when there is too much light
too much stimulation there no need for the high sensitivity).
But when we enter a dark place that little amount of pigment is insufficient to
respond to this little amount of light so you can’t see clearly.
To overcome this problem there is formation of this pigments, the formation is
very fast in cones. So you can see after 1-5 mins but maximum after 20 mins you
can see clearly because after this time the rods will be working and they have too
much rhodopsin and they are large in number(100 millions).
<< Soo in dark adaptation retinal sensitivity increases very fast for the first 5 mins
then slowly until 20 mins when you will see clearly>>
*Light adaptation is the reverse; when we go out there is too much light and
sensitivity is high . so the pigment will decreases (the first decrease is due to
cones).
Now I am going to talk about fig. 50-8 on {slide 30}
Here we can see that the cones adaptation is faster and happens before the rods
adaptation.
*sensitivity is directly proportional to the amount of the pigment. More pigment
more sensitivity.
-- vitamin A deficiency
*pigment rhodopsin consists of (opsin and elevensis retinal)
elevensis retinal is a vitamin A derivative.
SOO deficiency in Vitamin A there is no elevensis retinal no rhodopsin
no pigment so no sensitivity.
So in this case u can’t see at night because there is no light and this case u
need big amount of pigment, but in light u can see very well because there is
enough light.
As we took previously color vision due to cones
Dark and night vision due to rods
There is 1 type of rods and 3 types of cones (primary cones)
Primary cones: blue, red, and green.
*All cones consists of pigments which is rhodopsin which consists of ( opsin and
elevensis retinal).
Elevensis retinal is the same in the 3 types of the cones but what differ is the
opsin .<red cone opsin sensitive to red colour)
How we can see different colors?
We can see (visible light) between 400-700 nm.
Light above violet ultra violet
Light below red infrared
- Now each cone is sensitive to certain wavelength spectrum (light
spectrum). {slide 34}
- blue cones >400-530 nm
- Green cones 450-620 nm
- Red cones 470-700 nm
- Rods have only one spectrum maximum 500 nm (as the doctor said)
*so whenever you see a light it will stimulate these cones .
Any color will be seen by stimulating 1, 2 ,3 of these cones but in different
percentage.
-For example to see the green color
The green cones should be stimulated 67%
The red cones should be stimulated 31%
The blue cones should be stimulated 36%
-Another example
Orange = 42% green + 99% red
Deficiency in any type of color cones color blindness
The most common is red color blindness protanope
Green color blindnessdeuteranope
Blue color blindness is very rare (autosomal recessive disease)
Color blindness is a genetic disorder pass along on the x chromosome
So to have color blindness , for females they should have the two x
chromosomes infected, so females are usually carriers .but for males they
are always affected.(XY)
** Let us talk about people with color blindness
-Some people think that a colored blind person can’t see the red color (for
example) but this is wrong because he can see it but not the same as a
normal person.
So when he see it and learn its name when he see it again he can say that
this is red even though he can’t see the real red!!
But the problem that they can’t differentiate these colors when mixed with
others (bad contrast) so they can’t pick the correct color.
Color Blindness Chart {slide 36}
It is used as a test for color blindness.
Here in the slides as you CAN’T see:
The left one in normal is 74, for red-green read it 21
The right one in normal is 42, for red read it 2, for green 4
This test depends on the differentiation between colors. So the person with
green color blindness will not differentiate the green dots.
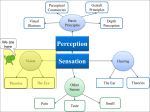
Neural organization of the retina {slide 37}
Signals moves from (rods and cones)horizontal cells then bipolar cells
amacrine cellsganglion cellsganglion axonsoptic nerve.
**all these cells respond to the light by graded potential except ganglion
cells always respond by action potential and some amacrine cells also by
action potential ( these two send the signals all the way to the brain). This is
very important because it increases the retinal sensitivinity.
Signal transmission in the retina {slide 39}
Transmission of signals in the retina is by electronic conduction (local
conduction).
Lateral inhibition {slide 40}
Occurs at two levels :1- horizontal cells
2- amacrine cells
It is important for sharpness and contrast.
As u can see in {slide 41}
When center part is excited the lateral part is inhibited, that will prevent
the lateral spread of light excitation on the retina.
It is the same with cones (blue, red, green) one cone inhibit the others so
that there will be contrast between these colors.
The ganglion cells {slides 43 44}
As you remember we said that neurons that come from receptors have
basal rate firing.
Same as ganglion cells it can increase rate of firing+ve
decrease rate of firing-ve
There are 3 types of ganglion cells
((as the doctor said they are not important))
1- W cells (40%) sensitive to directional movement.
2- X cells (55%) a- most frequent
b-small receptive field
c- good for color and sharp vision
3- Y cells (5%) a-least frequent
b-large receptive field
c-not for location but change in visual
field
** Excitation of ganglion cells
(the doctor mentioned )
1-spontanously active
2-they can increase and decrease firing rate
3-respond to contrast borders
Function of amacrine cells {slide 42}
1-respond to movement of the light
2-respond to onset of visual signal
The Eye III
Central neurophysiology of vision (neural pathway) L12
First the doctor read the objectives {slide 2}
*As we took that in all sensations what comes from the right side go to the
left side of the cerebral cortex and vice versa. In vision there is something
special <special crossing>.
Each retina in each eye consists of nasal part and temporal part, So what
comes from my right field of vision will not hit temporal part of the right
eye , instead it will hit the temporal part of the left eye and nasal part of
the right eye.
So the nasal field fibers will cross, but the temporal fibers will not.so that
the fibers that carry the same image go to the same side.
Visual Pathways to the brain {slide 3}
-
Axons of ganglion cells make the optic nerve
Nasal fibers will cross and make the optic chiasm
After crossing nasal and temporal fibers make optic track
Then fibers go to the superior collicolli in mid brain
Then go to supra chiasmatic nucleus of hypothalamus
Then to lateral geniculate body of thalamus
At last it will go to the occipital lobe (cerebral cortex) through optic
radiations.
Now I am going to talk about some of these steps
*there are 4 collicolli in the mid brain
2 superior for vision
2 inferior for hearing
There is tectal nucleus in each collicolli, that sends motor track (tecto spinal
track) . Function: movement of the head and neck.
For example when there is a flash light from my left side the tectum in
superior collicolli will send a command by the tecto spinal track to the head
and neck to turn to the left. And same by hearing a voice but the difference
that for hearing inferior collicolli is responsible not the superior one.
**Under the optic chiasm there is the pituitary gland , above the pituitary
there is hypothalamus .From this area the optic track go to the superior
chiasmatic nucleus of hypothalamus to tell this nucleus if there is light or
not.so this is used for biological clock; hormones are secreted in pulses (not
the same at all the time).for example cortisol secreted maximally in the
morning at 8 o’clock, so the information about the day and the night comes
by this method.
***the somatic sensations go to the ventro posterio lateral (ventro basal
complex) in the lateral geniculate body of the thalamus.
*** For hearing the sensation will go to the medial geniculate body of the
thalamus.
At last we are going to talk about cut in this system {slide 8}
1- Cut in optic nerveblind in one eye (anopsia)
2- Cut in optic chiasmcan’t see lateral sides only see in the center [tunnel
vision] (heteronymous hemianopsia)
3- Cut in optic track (homonymous hemianopsia)
4- The number of the optic radiations is so high so it is possible that group
of this optic radiation is cut , for example : superior left or superior right
or inferior left or inferior right. (quadrant anopsia)
5- Quadratic anopsia with macular sparing. The macula is due to the
fovea.(it wasn’t so clear I hope it will be clear in the next sheet).
Sorry for being late in writing this sheet, bs elbiochem kan elsabab :S
Done By : George Deeb
This sheet is dedicated to all my friends.