Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
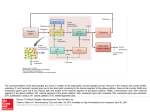
Motor Systems Motor Unit Motoneuron + muscle fibers it innervates Range in size from a few muscle fibers (e.g. extraocular muscles) To hundreds of fibers (e.g. digits) To thousands of fibers (e.g. trunk and major limb segments) Smaller motor units yield more refined control a motor “fovea” sarcomere Excitation of a Muscle Fiber • An action potential in an alpha motoneuron axon. • ACh is released by the axon terminal at the neuromuscular junction (synapse between motoneuron and muscle. • Nicotinic receptor channels open, Na+ enters and the membrane depolarizes (EPSP). • Voltage-gated Na+ channels open and an action potential is propagated down the muscle fiber. • Depolarization produces Ca2+ release from intracellular stores. Contraction of a Muscle Fiber • Ca2+ binds to tropinin. • Myosin binding sites are exposed. • Myosin heads bind actin. • Myosin cross-bridges pivot. • Myosin heads disengage at the expense (ATP-dependent). • Recycle as long as Ca2+ and ATP are present. Relaxation of a Muscle Fiber • As EPSPs end, membrane returns to resting potential. • Free Ca2+ is sequestered by metabolically driven pump. • Myosin binding sites covered. at rest α-motoneuron activation α-, γ-motoneuron co-activation Co-activation of α-motoneurons and γ-motoneurons Meissner’s Pacinian Merkel’s Ruffini’s Free nerve ending Monosynaptic stretch reflex Golgi tendon organ reflex somatosensory afferents motor afferents (Aδ) (C) Muscle Spindles (intrafusal fibers) respond to muscle length, or stretch insensitive to tension 1a afferents for dynamic spindles Group II afferents for postural spindles monosynatic stretch reflex (excitatory) Golgi Tendon Organs respond to muscle tension insensitive to muscle length, or stretch 1b afferents disynaptic reflex (inhibitory) Problem of Locomotion Degrees of freedom problem (Bernstein) Dozens of joints controlled by hundreds of muscles Muscles can contract in any combination, in any order, for any duration, and with any force. Possibilities are virtually limitless, making control of complex movements at the level of individual muscles impossible Reciprocal inhibition between motor units of antagonistic muscles Crossed extensor reflex oscillators = “legos” of movement CPGs = what you can build with legos Descending motor pathways Lateral and ventromedial pathways Pyramidal and extra-pyramidal systems Supplementary Motor Area (SMA) important for instituting motor programs activated prior to voluntary movement activated during mental rehearsal Premotor cortex sensory guided movement cooperatively with basal ganglia mirror neurons Pre-frontal cortex decisions for actions Cortex Globus Pallidus Thalamus and STN Rubrospinal tract Substantia Nigra Reticular Formation Red Nucleus (nucleus ruber) Cerebellum Reticulospinal tract Cortex cortex Thalamus and STN Rubrospinal tract cerebellum Substantia Nigra Pontine nuclei and Reticular Formation Red Nucleus (nucleus ruber) pontine nuclei Globus Pallidus Reticulospinal tract Cerebellum thalamus Cortex cortex Thalamus and STN Rubrospinal tract globus pallidus Substantia Nigra Pontine nuclei and Reticular Formation Red Nucleus (nucleus ruber) striatum Globus Pallidus Reticulospinal tract Cerebellum thalamus Cortex cortex Thalamus and STN Rubrospinal tract substantia nigra Substantia Nigra Pontine nuclei and Reticular Formation Red Nucleus (nucleus ruber) striatum Globus Pallidus Reticulospinal tract Cerebellum thalamus Cortex Globus Pallidus Thalamus and STN Rubrospinal tract Substantia Nigra Reticular Formation Red Nucleus (nucleus ruber) degenerate in Huntington’s disease Cerebellum Reticulospinal tract Cortex Globus Pallidus Thalamus and STN Rubrospinal tract Treatments: 1. l-DOPA to compensate for lost DA projections Substantia Nigra Reticular Formation Red Nucleus (nucleus ruber) degenerates in Parkinson’s disease Cerebellum 2. Deep brain stimulation of striato-pallidal projections 3. Surgical destruction of cells in medial pallidum Reticulospinal tract Subthalamus pedunculopontine nucleus (PPN) reticulospinal tractspinal CPGs ALS: Upper motoneuron disease Polio: Spinal motoneuron disease Apraxias: Frontal cortical damage