Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
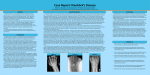
SCAHPO-LUNATE DISSOCIATION Introduction Scapho-lunate dissociation is the most common significant ligamentous injury of the wrist. The condition is also sometimes referred to as rotary subluxation of the scaphoid. It is an important injury to recognize as it may lead to chronic disability and pain if missed. Anatomy The scapholunate interosseous ligament Stability of the scapholunate joint is maintained primarily by the scapholunate interosseous ligament, in addition to many secondary stabilizers, including the volar carpal ligaments and the dorsal capsule. Scapholunate dissociation is a spectrum of rotational abnormalities that is dependent on the severity of the injury and the resulting involvement of ligamentous abnormalities, and is one of the most common forms of carpal instability. Mechanism ● It is caused by a fall on the outstretched hand, usually with forceful dorsiflexion. Greater degrees of force can result in frank carpal dislocation, (lunate or perilunate dislocation). ● This injury occurs with tears of the volar radiocarpal ligaments and the scapholunate interosseous ligament complex. ● In addition the scaphoid may then sublux by rotating vertically downwards toward the palmar surface. Classification Carpal instability patterns may be classified as static or dynamic, based on the presence or absence of radiographically detectable abnormalities on routine studies. Rupture of the scapholunate interosseous ligament alone typically results in dynamic scapholunate instability, requiring abnormal stress radiographs or motion studies to diagnose. Rupture of at least one additional secondary stabilizing ligaments is necessary for static scapholunate diastasis to occur, which then becomes evident on routine radiographic studies. Complications ● If not repaired there tends to be proximal migration of the capitate between the scaphoid and lunate, associated with early and severe degenerative arthritis, ultimately resulting in a condition known as “scapholunate advanced collapse” (SLAC) ● Chronic disabling wrist joint instability with pain. ● Commonly associated fractures include scaphoid and distal radius fractures. Clinical Features 1. Variable pain over the dorsal wrist, usually increased by dorsiflexion. 2. Swelling is variable, depending on the severity of the injury, but is usually minimal. 3. Tenderness: ● 4. Especially localized to the dorsum of the wrist over the joint, (just distal to the radius). Carpal instability: ● Stabilize radius with one hand and with the other push the volar tubercle of the scaphoid dorsally, pain, clicking and movement may be detected. Investigations Plain radiography: PA wrist radiographs showing a normal wrist (left) and a wrist with scapholunate dissociation, (right) confirmed by the wide gap between the lunate and the scaphoid (left and center arrows) and a signent ring sign of the scaphoid (right arrow) Radiological features include: 1. 2. There is widening of the scapholunate joint space in A-P views of the wrist. ● > 3 mm separation is abnormal, (the “Terry Thomas” sign) ● Initial views may be normal and if the injury is suspected “stress views” may be done. Stress views are taken with a clenched fist, in ulnar deviation, on an AP view. ● The dynamic changes on the stress views may be further appreciated by comparison with the opposite side. If there is an associated rotatory subluxation of the scaphoid, the scaphoid in the PA view will be seen end on with the cortex of the distal pole appearing as a dense ring shaped shadow over the distal scaphoid, (the “Signet Ring” sign.) ● 3. It tilts more palmar and appears shorter as it is viewed more on its end and a circular appearing cortex of bone becomes visible, producing the signet ring sign. Lateral views: Lateral x-ray of a normal left wrist showing the relationship of the scaphoid’s palmar angulation in relation to the capitate. ● The lateral view may show a misalignment of the scaphoid and lunate. The scaphoid is tilted anteriorly, (ie palmar) whilst the lunate is tilted dorsally, (this is known as dorsal intercalated segment instability or the “DISI” pattern) 1 ● Normally on the lateral the scaphoid lies at an angle of 30 - 60 degrees forward in relation to the capitate. In scapho-lunate dissociation with scaphoid subluxation the scaphoid is angled to the palmar surface more than 60 degrees (and up to 90 degrees) in relation to the axis of the capitate, i.e. the proximal pole displaces posteriorly and the distal pole displaces anteriorly (producing the signet ring sign on the A-P views). CT scan This can be done to confirm the diagnosis when clinical suspicion is high, despite inconclusive plain radiology. CT is also frequently done to more fully assess the carpal bones for associated occult injury. MRI ● MRI is also a further option for confirming the diagnosis and assessing for any associated occult carpal bone injury. MRI had the added advantage of being able to assess the ligamentous injury. Management 1. Analgesia as clinically indicated. 2. Backslab and elevation. 3. Orthopaedic referral: ● These injuries must be referred to the orthopedic unit for reduction, surgical repair of the disrupted ligament and internal fixation with a kirschner wire. References 1. Appley’s System of Orthopedics and Fractures, 8th ed 2001, p. 627-628. 2. Rosen’s Emergency Medicine, 5th ed 2002, p.541 3. Tintinalli J et al Emergency Medicine: a comprehensive study guide, 5th ed, p.1776 4. Scapholunate Dissociation in Learning Radiology Website: ● www.learningradiology.com/ Dr J Hayes Reviewed April 2013