Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
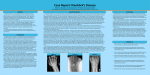
Wrist Pain Objectives: I. Recall anatomy of the wrist joint. II. Etiology of painful wrist. III. Diagnostic approach. IV. Ganglion V. De Quervian syndrome. VI. Keinbock,s disease. Wrist Joint: (radiocarpal) joint Articulation between the distal end of the radius and the articular disc above and the scaphoid , lunate, and triquetral bones below Type: Synovial condyloid joint. Ligaments: Anterior (palmar) and posterior (dorsal) ligaments strengthen the capsule. The median (ulnar collateral) ligament is attached to the styloid process of the ulna and to the triquetral bone. The lateral (Radial collateral ) ligament is attached to the styloid process of the radius and to the scaphoid bone Movements: Flexion. Extension. Abduction Adduction. Circumduction. BLOOD SUPPLY OF WRIST JOINT: Branches of the dorsal and palmar carpal arches. INNERVATION OF WRIST JOINT: Anterior interosseous and the deep branch of radial neve branch of the median nerve. Etiology of painful wrist: 1. NEUROLOGIC CAUSES OF PAIN 1. Carpal tunnel syndrome. 2. Pronator teres syndrome 3. Superficial radial neuropathy 4. Compression of the Ulnar Nerve at the Wrist (Guyon Canal Syndrome). 2. MUSCLO-JOINT RELATED CAUSES OF PAIN 1. Intersection syndrome 2. DeQuervain’s tenosynovitis. 3. Arthritis, eg, rheumatoid arthritis, osteoarthritis, reactive arthritis (Reiter’s syndrome), psoriatic arthritis, gout or pseudogout, septic arthritis. 4. Triangular fibrocartilage complex (TFCC) injury 3. VASCULAR CAUSES OF PAIN 1. Keinbock’s disease. 4. FRACTURES 1. Lunate fracture or dislocation, scaphoid fracture (snuffbox pain). 2. Colles (distal radius) fracture. Diagnostic approach: History. Physical Examination. a. Look: b. Feel: c. Move: d. Measure: e. Special tests: Provocative Testing • Neurological Examination. • LAB: If infection is suspected. •IMAGING X-rays A-P and lateral views are obtained routinely. Special views may be necessary to show a scaphoid fracture or carpal instability. Arthrography Defects in the triangular fibrocartilage, scapho-lunate ligaments or luno-triquetral ligaments can be identified by arthrography. Computed tomography CT is the ideal method for assessing congruity of the distal radio-ulnar joint. Magnetic resonance imaging MRI is particularly useful for detecting changes associated with scaphoid fractures, avascular necrosis of the lunate, occult dorsal ganglia and intra-osseous ganglia. Radionuclide scan A localized area of increased activity may reveal An occult scaphoid fracture or early osteoarthritis. Fluoroscopy Fluoroscopic examination may be needed to demonstrate some patterns of carpal instability Other methods: Aspiration or Arthroscopy Ganglion •The ganglion cyst is the most common swelling in the wrist. It arises from leakage of synovial fluid from a joint or tendon sheath and contains a glairy, viscous fluid. Although it can appear anywhere around the carpus, it usually develops on the dorsal surface of the scapho-lunate ligament • T • Not related to neural ganglion or ganglionic cell. • Women are more likely to be affected than men. • Ganglia are common among athletes he average size of these cysts is 2.0 cm. De Quervain syndrome Tenovaginitis syndrom (tenosynovitis) Common and well recognized condition characterized by pain over styloid process of radius and palpable nodule in the course of abductor pollicis longus and extensor pollicis brevis tendon. De Quervain's is more common in women It may be initiated by overuse but it also occurs spontaneously, particularly in middle-aged women, and sometimes during pregnancy Pathology: * The fibrous sheath of abductor pollicis longus & extensor pollicis brevis tendons are thickened where they cross the tip of radial styloid process *Tendons themselves appear NORMAL. Clinical features: - The condition is commonest in middle – aged women -Pain , local tenderness , swelling and difficulty gripping Diagnosis: Finkelstein's test: grasps the thumb (place it in the palm) and the hand is ulnar deviated sharply , If pain occurs along the distal radius then test is +ve and vice versa. Complications: May interfere mechanically with normal movement of thumb or lateral distal part of radial aspect. Treatment: The early case can be relieved by a corticosteroid injection into the tendon sheath, sometimes combined with splintage for symptoms relief. Resistant cases need an operation, which consists of slitting the thickened tendon sheath. Ischemic necrosis of the lunate bone, due to chronic stress or injury. ( traumatic softening ) More common in patients with abnormally short ulnas (at wrist). Young adult (usually affects the dominant wrist of men aged 20-40 years.) Ache and stiffness Localized tenderness over the lunate Grip strength is diminished Later stages wrist movement is limited and painful. Pathology: stage 1, ischemia without naked-eye or radiographic abnormality. stage 2, trabecular necrosis with reactive new bone formation and increased radiographic density, but little or no distortion of shape. stage 3, collapse of the bone. stage 4, disruption of radio-carpal congruence and secondary osteoarthritis Kienbock’s disea X - RAY Stage 2. (Left) This illustration shows that the lunate has hardened with more than one fracture line. (Right) The lunate is brighter than the surrounding bones, which indicates that the bone is dying. Stage 3. Both the illustration and x-ray image show that the lunate has begun to collapse and several bones in the wrist have shifted out of position. Stage 4. (Left) This illustration shows damage to several bones in the wrist. (Right) This CT scan also shows deterioration in the bones of the wrist Treatment stag e X-ray , MRI Tx 1 Normal x-ray, changes on MRI Cast for 3 months Vascularized bone graft 2 Lunate sclerosis on plain x-ray, fracture lines sometimes present without collaps Vascularized bone graft If negative ulnar variance: radial shortening If positive ulnar variance: radial dome osteotomy 3a Fragmentation of lunate; height preserved Proximal row carpectomy 3b Collapse of lunate, proximal migration of capitate, fixed scaphoid rotation Scapho-capitate fusion Scapho-trapeziumtrapezoid fusion Proximal row Reference