Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
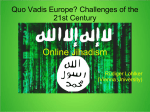
Voices Clinic www.voicesclinic.co.uk Introduction Distressing voices (auditory hallucinations) are experienced by approximately 70% of patients with a diagnosis of schizophrenia and can have devastating effects due to high levels of distress, depression, impaired social functioning, delayed recovery and an increased risk of suicide. Distressing voices are also common in patients with other diagnoses. The National Institute for Health and Care Excellence (NICE) recommend Cognitive Behaviour Therapy for Psychosis (CBTp) for the treatment of distressing voices (NICE, 2014). However, it is widely acknowledged that there are gaps in the provision of psychological therapies with only 10% of those who could benefit from CBT receiving it (Schizophrenia Commission, 2012). The Voices Clinic is designed to cross diagnostic and service boundaries to improve access to innovative evidence-based therapies for distressing voices while continuing to research their effectiveness. The clinic is available to an increasing number of patients across our assessment and treatment services who hear distressing voices. All patients accepted into the clinic are offered high-quality evidence-based therapies for voices that are consistent with NICE guidelines. The therapies are tailored to individual need and include therapies based on the principles of Cognitive Behavioural Therapy (CBT) and Mindfulness, offered in both individual and group formats. Although psychological therapy is helpful for many people who hear distressing voices, not everyone benefits (Thomas, Hayward et al, 2014). The Voices Clinic seeks to improve our understanding of voice-hearing experiences and enhance the effectiveness of the therapy that we offer. Patients Which therapies are available? On average, patients have heard voices for around 16 years at the time of the initial assessment. About half of the patients referred to the clinic were female, and half male. The Voices Clinic offers two therapies within a stepped-care model referred to as Levels 1 and 2. If a patient remains distressed by voices after the brief therapy, they are offered a Level 2 therapy. The most commonly self-reported diagnoses of patients are: • Schizophrenia (28%) • Borderline Personality Disorder (BPD)/Emotionally-Unstable Personality Disorder (EUPD) (13%) • Schizoaffective Disorder (6%) • Other e.g Post-traumatic Stress Disorder (PTSD)/Complex Trauma or Depression (6%). • Mixed (34%) • Unknown (3%) • No diagnosis (7%) Level 2: Referrals/ retention Level 1: Brief individual therapy – a four session individual therapy using the principles of Coping Strategy Enhancement (CSE; Tarrier et al., 1993) is offered to all patients. The therapy seeks to identify and systematically implement coping strategies from the patient’s existing repertoire of strategies. • 157 referrals accepted in the two years since opening the clinic. • 121 patients completed a baseline assessment. • 119 patients (98% of those who completed a baseline assessment) were offered Level 1 Therapy - indicating a high level of appropriate referrals. • 107 patients (90% of those offered Level 1 therapy) attended at least one Level 1 therapy session. • 79 patients (74% of those who attended at least one Level 1 therapy session) completed or are still receiving Level 1 therapy. • 30 patients (45% of those who completed Level 1 therapy) completed or are still receiving Level 2 therapy. Group Person-based Cognitive Therapy (PBCT) – a 12-session therapy that integrates cognitive behaviour therapy for psychosis (CBTp) (exploring and challenging beliefs about self and voices) with a mindfulness-based approach (Chadwick et al, 2016). Patients who are not able to attend Group PBCT are offered individual Relating Therapy over eight sessions as an alternative. Outcomes Data has been analysed for 64 patients who have completed Level 1 therapy and 25 patients who have completed Level 2 therapy. Comparison of their baseline scores and post-therapy scores indicated that high proportions of patients have shown statistically significant improvements (see Table 1). The differences between the means are also presented in Table 1. Although the degree of clinical change varies by outcome, the amount of change in Voice Related Distress following Level 2 is clinically significant. Table 1: Proportions of patients showing an improvement & differences between the baseline and the Level 1/Level 2 mean outcome scores Count Referral pathways Flow diagram of referral and therapy pathways in Voices Clinic Level 1 compared to baseline Proportion improved Level 2 compared to baseline Proportion improved Outcomes N Recovery (CHOICE) Mental Wellbeing (SWEMWBS) Voice Frequency (PSYRATS) Anxiety (DASS) Voice Related Distress (PSYRATS) Depression (DASS) 64 63% 57% 55% 53% 52% 45% +0.6* +0.3 -0.7* -1.3* -1.6* -1.1* 75% 84% 58% 48% 75% 64% +1.5* +3.6* -1.3* -0.9 -4.0* -2.6* Difference between means 25 Difference between means Note: * indicates a p-value <0.05 from a t-test comparing baseline scores to the post-therapy score; CHOICE = Choice of outcome in CBT for psychoses; SWEMWBS = short Warwick Edinburgh Mental Wellbeing Scale; DASS = Depression, Anxiety & Distress Scale; PSYRATS = Psychotic Symptoms Rating Scale. ATS assessment Feedback from patients Suspected distressing voices Yes No Usual ATS care Referral to Voices Clinic Feedback from individual patients suggests that the Voices Clinic: Inappropriate referrals Voices Clinic Assessment Many patients referred to the Voices Clinic have never attended talking therapy or report not having anybody to talk to about hearing voices. The brief Level 1 therapy was designed to provide an opportunity for patients to talk about these experiences. Patients’ feedback indicates that attending individual therapy not only helped them to talk to a therapist, but also prepared them for sharing experiences with other patients in group therapy at Level 2. Offer to all patients “Therapy was quite good and made me feel alive”. “Made me feel someone actually believed me.” • normalises voice-hearing • promotes personal control over voices • increases confidence to challenge negative content of voices Level 1 therapy • impacts the quality of what voices are saying “I felt relieved. I wasn’t ridiculed. I didn’t feel so lonely.” • provides practical guidance on achieving goals • allows experiences to be shared in a non-judgemental way • positively impacts personal & work life • encourages taking an active role in ensuring one’s own wellbeing Discharge from Voices Clinic “The group made me realise that I’m still a valuable member of society.” • helps individuals to practice mindful acceptance of voices • helps to increase the understanding of voices Research Network & Clinic Studies “I felt listened to. I didn’t feel judged.” “It helped me look at things differently. Helped me to set goals. Helped me to deal with the voice differently and to manage it better.” Review Level 2 therapy (group) Level 2 therapy (individual) Review Review Discharge from Voices Clinic Recent innovations Further information An app has been developed to support patients both during and when they leave the Voices Clinic. The ‘Choices’ app facilitates the continued use of coping strategies, mindfulness and assertive responding, and can be individualised to reflect the specific learning of individual patients. If you require further information please contact Dr Mark Hayward, Clinic Director. e-mail: [email protected] Tel: 01273 242034 Mobile: 07770 331160 Address: Research & Development, Sussex Education Centre, Sussex Partnership NHS Foundation Trust, Mill View Hospital Site, Nevill Avenue, BN3 7HZ. The Voices Clinic has been made available to patients within Lewes Prison and Early Intervention in Psychosis Services. As these services cannot offer group therapy, they are piloting a four-session individual CBT therapy at Level 2 that focuses upon appraisals of self and voices. Key References Chadwick, P., Strauss, C., Jones, A-M., Kingdon, D., Ellett, L., Dannahy,L., Hayward, M. (2016) Group mindfulness-based intervention for distressing voices: A pragmatic randomised controlled trial Schizophrenia Research. 10.1016/j.schres.2016.04.001 NICE (2014). Psychosis and schizophrenia in adults: Treatment and management (Clinical guidelines, CG178). London, UK. The Schizophrenia Commission (2012). The Abandoned Illness: a report from the Schizophrenia Commission. London; Rethink Mental Illness. Tarrier, N., Beckett, R., Harwood, S., Baker, A., Yusupoff, L. & Ugarteburu, I. (1993). A trial of two cognitive-behavioural methods of treating drug-resistant symptoms in schizophrenic outpatients. I: Outcome. British Journal of Psychiatry, 162, 524–532. Thomas, N. Hayward, M. Peters, E. van der Gaag, M. Bentall, R.P. Jenner, J. et al (2014). Psychological Therapies for Auditory Hallucinations (Voices): Current Status and Key Directions for Future Research. Schizophrenia Bulletin, 40 (suppl. 4), S202-S212. If you would like to refer a patient to the Voices Clinic then please speak to the patient then send their details to [email protected] Dedicated to Research www.sussexpartnership.nhs.uk/research