Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Coronary artery disease wikipedia , lookup
Heart failure wikipedia , lookup
Electrocardiography wikipedia , lookup
Lutembacher's syndrome wikipedia , lookup
Quantium Medical Cardiac Output wikipedia , lookup
Myocardial infarction wikipedia , lookup
Cardiac surgery wikipedia , lookup
Atrial septal defect wikipedia , lookup
Dextro-Transposition of the great arteries wikipedia , lookup
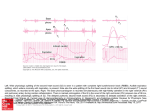
Postural Variation in Second Sound Splitting* I. C. MacKenzie;** M. E. Rosenberg;** G. Kroll, M.D.;? and M. Brandfonbrener, M.D.; Pbonocardiograms were obtained of 30 normal men in the supine and sitting positions. They demonstrated significantly greater S2 splitting and respiratory variation in S2 in the sitting position. However, several individuals showed wider splitting or greater variation while supine. Fixed splitting occurred in three subjects while supine and five others while sitting, but in no normal subject was splitting fixed in both positions. 1866, Potainl first described the normal inI ncrease in splitting of the second heart sound with inspiration. Unlike the first heart sound, which is composed of several components which do not correspond well temporally, to valve closure, the second sound has been well documented to be For editorial comment, see page 4 produced by both aortic and pulmonic closures. Boyer and C h i ~ h o l m Aygen ,~ and B r a ~ n w a l d and ,~ Castle and Jones4 found that both aortic and pulmonic closures vary with respiration. From 12 percent to 50 percent of the variation in splitting is accounted for by change of the Q-A2 interval. Splitting of the second heart sound has been found to vary in certain states. Shah and Slodki5 found that advancing age brought a gradual decrease in second sound splitting, and that hypertension correlated with a prolonged Q-At interval and reduced splitting. Right bundle branch block causes wide ~ p l i t t i n g ,but ~ respiratory variation is usually preserved. DePasquale and associates7 found that right ventricular failure was associated with fixed wide splitting and left-sided failure with reduced or paradoxic splitting. A patient with biventricular failure may demonstrate normal splitting with slight or paradoxic respiratory variation. Tests of cardiac function have been devised that utilize observation of the splitting of the second heart sound. Cobbs and co-workerss found that pulmonary embolism produced a wide fixed split, the degree of splitting increasing with the severity *From the Veterans Administration Research Hospital and Northwestern University hledical School, Chicago. "Medical student. +Assistant Professor of Medicine. $Professor of Medicine. Reprint requests: Dr. Brandfonbrener, 303 East Chicago Aoenue, Chicago 60611 of embolism. Differences in the respiratory variation of the Q-A2 and Q-P2 intervals may help differentiate chronic constrictive pericarditis from African cardiomy~pathy.~ In constrictive pericarditis there is inspiratory shortening of Q-A2 interval which causes inspiratory splitting, with a fixed Q-P2. In biventricular failure due to cardiomyopathy, Q-Aa is fixed while Q-P2 is either fixed or moves very little. Auscultation of the second heart sound is especially helpful in the diagnosis of congenital heart disease. It remains an important clinical means of differentiating the Eisenmenger form of atrial septa1 defect ( ASD ), from other causes of Eisenmenger's syndrome.1° In the former the splitting is more likely to be fixed. Both ASD and VSD cause wide splitting in proportion to the shunted blood flow7 but relatively fixed splitting occurs in ASD. Relatively Exed widely split S2 is a helpful sign when a significant shunt exists in children over five years of age. In ASD fixed splitting is associated with simultaneous delay in aortic and pulmonic closure. Breen and Rekatel1 pointed out that a child suspected of ASD must be auscultated in the sitting position as some normal children have fixed wide splitting in the supine position. Castle and associates12 also found that some children have fixed narrow splitting in the sitting position. Final cardiac evaluation must therefore be done supine, immediately after sitting and after sitting several minutes. A few studies have been done concerning the effect of posture on second sound splitting. ASD shows wide splitting in the supine and sitting positions. Standing has been found to decrease the wide splitting associated with pulmonary embolus.' Castle studied 116 children with respect to the effects of posture, heart rate, sex, age, height and weight on second sound splitting and found wider CHEST, VOL. 63, NO. 1, JANUARY, 1973 Downloaded From: http://journal.publications.chestnet.org/pdfaccess.ashx?url=/data/journals/chest/21552/ on 05/12/2017 POSTURAL VARIATION IN SECOND SOUND SPLITTING splitting and greater respiratory variation in the sitting versus supine position. After sitting five minutes, girls showed 7 msec wider splitting. No other variable significantly affected splitting. There have been no adequate studies showing the effect of posture on splitting of the second heart sound in adults. One study showed greater respiratory variation in splitting in the supine position13 than sitting, but most subjects in this study showed relatively fixed splitting, ie respiratory variation of less than 10 msec. This study investigated the effects of posture on second sound splitting in a population of normal men. Phonocardiograms were obtained from 33 men, between 22 and 25 years of age. Each had a normal cardiorespiratory system by history and clinical examination. No attempt was made to correlate age, height, weight, pulse, blood pressure or respiratory rate with splitting because of the fairly narrow distribution of these variables in these subiects. , , and because of previous studies showing slight or no differences produced by these factors.12-1.1 A Sanborn 4-channel photographic recorder was used to record responses from a Bowles high frequency chest microphone. Recordings were made at 75 or 100 mm per second. Respiratory motion was recorded from a pressure sensitive tambour attached to a blood pressure cuff around the subject's chest. Lead 2 of the ECG was simultaneously recorded. Each subiect rested several minutes in the s u ~ i n ewsition. A phonocardiogram, as described above, was then recorded from the second left intercostal space. The subject then sat up and a second recording was taken after sitting 30 seconds. A final recording was made after sitting five minutes. Three to five normal respiratory cycles were included in each recording and the average maximum and minimum splitting was obtained. Three of the original 33 recordings were discarded because of interference. Table l-Average Splitting Intervalr i n Supine and Sitting Position. (30 S u b j w u ) . Position Respiratory Phase* Average Difference Standard AGPC*' Deviation (msec) (msec) Supine Inspiratorg Expiratory Average variation 11.8 24.8 17.0 11.5 7.5 8.1 Sitting 30 seconds Inspiratory Expiratory Average variation 47.4 21.5 25.9 13.0 7.8 10.8 Sitting 5 minutes Inspiratory Expiratory Average variation 48.2 21.2 24.0 13.6 9.4 10.5 'Average of values for 3 to 5 respiratory cycles. 'AC =Aortic closure. PC = Pulmonic closure. variation in the sitting positions, although five had most variation while supine. Three of 30 showed fixed splitting (defined as respiratory variation less than 10 rnsec) while supine, and five others showed this after sitting five minutes. All of the subjects demonstrating "fixed splitting in some position showed respiratory variation greater than 12 msec in one of the other positions. . . Table 1 summarizes the average splitting intervals found in inspiration and expiration in each of these body positions. In the supine position, inspiratory splitting was 41.8 msec, standard deviation k 11.5, after sitting 30 seconds 47.4 msec +13.0, and after sitting five minutes 48.2 msec k13.6. Average expiratory splitting in the three positions was 24.8 msec k7.5; 21.5 msec 27.8; and 24.2 msec k 9 . 4 respectively. Splitting of S2 in the sitting position in inspiration is statistically significantly greater than that in the supine position (P<.01). Also, the respiratory variation in splitting is significantly greater in the sitting position than in the supine (P<.Ol). Subjects demonstrated variations in patterns of splitting. Seventeen of 30 had wide splitting in upright postures after both 30 seconds and five minutes, but three of 30 had widest splitting while supine. Twenty-one of 30 had greater respiratory The results of this study agree with the analysis of respiratory variation of S2 splitting by Castle and co-workers.12 One other publication concerning postural variation in adults showed contradictory results.13 Castle's study gave results similar to those reported here, for postural variation in children: 21 to 38 msec supine, 21 to 45 msec sitting 30 seconds, and 24 to 48 msec sitting five minutes. This suggests that the same factors causing respiratory variation in children occur in young adults. It is also apparent that a significant fraction of normal adults, as well as children, have fixed splitting in either supine or sitting positions. A well-known mechanism of respiratory variation in second sound splitting has been proposed from animal and human experiments. Inspiration causes decreased intrathoracic pressure, increased right ventricle filling and prolonged Q-P2. Pulmonary vascular capacity increases and left ventricular filling decreases, causing a shorter Q-A2. During expiration, the above sequence is reversed, causing longer Q-Az, shorter Q-P2 and decreased splitting. Other factors such as the differential pressures between the abdominal and thoracic cavities are less easy to quantitate but are probably quite significant. Besides different respiratory muscle action in CHEST, VOL. 63, NO. 1, JANUARY, 1973 Downloaded From: http://journal.publications.chestnet.org/pdfaccess.ashx?url=/data/journals/chest/21552/ on 05/12/2017 MAC KENZIE ET AL different b o d y positions, another mechanism m a y c a u s e m o r e variation i n splitting f o u n d in t h e sitting position. T h e m e a n central venous pressure (CVP) is less in t h e sitting position t h a n s u p i n e and the c a r d i a c o u t p u t l o ~ e r . ' ~ >Rl i~g h t h e a r t o u t p u t ( R O ) affects t h e Q-P2 interval. The plot of RO vs CVP on the Starling c u r v e is steeper a t lower filling pressures. Inspiratory a n d expiratory m o v e m e n t s causing t h e s a m e variation in CVP in the sitting position should c a u s e slightly g r e a t e r respiratory variation i n right-sided output in this position. T h i s should c a u s e greater variation i n t h e Q-P2 interval a n d second s o u n d splitting in t h e sitting position. The clinical implications of this s t u d y a r e t h a t if o n e encounters difficulty i n appreciating splitting of S2 w h e n t h e patient is supine, t h e n auscultation s h o u l d also be p e r f o r m e d w h e n the p a t i e n t is sitting. Exploring different areas a l o n g t h e LSB w i t h t h e stethoscope d i a p h r a g m is, of course, also helpful. If fixed or relatively fixed splitting is h e a r d either sitting o r lying, auscultation in t h e other position m a y clarify whether o r not the splitting is really fixed. 1 Potain PC: Note sur les dedonblements nonnaux des bruits du coeur. Bull Soc Med Hop Paris (Series 2 ) 3: 138168, 1866 2 Boyer SH, Chisholm AW: Physiologic splitting of the second heart sound. Circulation 18: 1010-1011, 1958 3 Aygen MM, Braunwald E : Splitting of the second heart sound in normal subjects and in patients with congenital heart disease. Circulation 25:328-345, 1962 4 Castle RF, Jones KL: The mechanism of respiratory variation in splitting of the second heart sound. Circulation 24: 180-184, 1961 5 Shah PM, Slodki hlD: The Q-11 interval. Circulation 29:551-561, 1964 6 Leatham A: The second heart sound, key to auscultation. Acta Cardiol 19:395-416, 1964 7 DePasquale NP, Burch GE, Phillips JH: The second heart sound. Am Heart J 76:419-431, 1968 8 Cobbs BW, Logue RB, Dorney ER: The second heart sound in pulmonary embolism and pulmonary hypertension. Am Heart J 71:843-844, 1966 9 Reid JV: The second heart sound in biventricr~larfailure due to African cardiomyopathy. An1 Heart J 68:38-40, 1964 10 Wood P: The Eisenmenger syndrome or pulnionary hypertension with reversed central shunt. Br \led J 2:701709,1958 11 Breen WJ, Rekate AC: Effect of posture on splitting of the semnd heart sound. JAhIA 173: 1326-1328, 1960 12 Castle RF, Hedden CA, Davis NP: Variables affecting splitting of the second heart sound in normal children. Pediatrics 43: 183-191, 1969 13 Jacono A, Bnonanno C, Perna N: Le modificazioni del secondo tono cardiaco indotte daile variazioni posturali. Minerva Cardioangiol 13:653-657, 1965 14 Harris A, Sutton G: Second heart sound in normal subjects. Br Heart J 30:739-742, 1968 15 Naimark KA, Wasserman K: The effect of posture on pulmonary capillary flow in man. J Clin Invest 41:949954, 1962 16 Mchlichael J, Sharpey-Shafer EP: Cardiac output in man by a direct Fick method. Br Heart J 6:33-40, 1944 Apropos of Productivity The Latin name of t h e mason-bees, Chalicodoma, means pebble-house. All these bees build their nests of calcareous clay mixed with sand and saliva; this sets the form of a hard mortar. T h e nests are rounded objects. Their outer surfaces are left rough like rustic architecture. Several bees may build close together so that their combined nests form a sort of comb and there may be cooperation between a number of bees putting a final coat of mortar around the finished structure. T h e inner walls of the nests are always smooth. They are filled with honey, sainfoin and broom flowers being favorite sources. Fabre calculated that collecting mud to build a cell and journeying to a sainfoin for honey involved journeying for 9%miles to complete and store one cell. T o provision all the cells and put on the final cover would mean flying for 275 miles. Andrews C: T h e Lives of Wasps and Bees, New York, American Elsevier, 1969 CHEST, VOL. 63, NO. 1, JANUARY, 1973 Downloaded From: http://journal.publications.chestnet.org/pdfaccess.ashx?url=/data/journals/chest/21552/ on 05/12/2017