Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Pharmacokinetics wikipedia , lookup
Drug interaction wikipedia , lookup
Discovery and development of ACE inhibitors wikipedia , lookup
Discovery and development of beta-blockers wikipedia , lookup
Pharmacogenomics wikipedia , lookup
Prescription costs wikipedia , lookup
Adherence (medicine) wikipedia , lookup
Pharmaceutical industry wikipedia , lookup
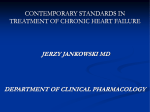
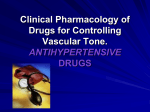
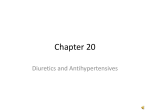
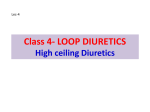
LOW-TO-MODERATE DOSE DIURETICS FOR FIRST-LINE AND COMBINED TREATMENT OF HYPERTENSION June 22, 2005 The ALLHAT Dissemination Committee And The National High Blood Pressure Education Program Prepared by: Curt D. Furberg, MD, PhD Department of Public Health Sciences Wake Forest University School of Medicine Winston-Salem, NC 27157-1063 Phone: (336) 716-3730; FAX: (336) 716-0395 E-mail: [email protected] Jeffrey Cutler, MD, MPH National Heart, Lung, and Blood Institute Project Office National Institutes of Health Bethesda, Md 20892-7936 Phone: (301) 435-0413; FAX: (301) 480-1773 E-mail: [email protected] Barry R. Davis, MD, PhD Coordinating Center for Clinical Trials University of Texas Houston Health Science Center, School of Public Health Houston, TX 77030 Phone: 713-500-9515; FAX: 713-500-9530 E-mail: [email protected] Jackson T. Wright, Jr., MD, PhD General Clinical Research Center University Hospitals of Cleveland Cleveland OH 44106-6041 Phone: (216) 844-5174; FAX (216) 844-1522 E-mail: [email protected] William Cushman, MD Preventive Medicine Memphis VAMC Memphis TN 38104-2193 Phone: (901) 577-7357; FAX: (901) 577-7457 E-mail: [email protected] -1- The purpose of this document is to provide information documenting the superior efficacy and safety of the use of low-to-moderate dose1 diuretics for the treatment of hypertension. The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure states (1): “Thiazide-type diuretics should be used as initial therapy for most patients with hypertension, either alone or in combination with 1 of the other classes (ACE inhibitors, ARBs, β-blockers, CCBs) demonstrated to be beneficial in randomized controlled outcome trials.” Historical Background Diuretics were introduced in the U.S. in the 1950’s. Two of the three subclasses, thiazide (including thiazide-like) diuretics and potassium-sparing diuretics, are FDA-approved for the indication of hypertension. IMS data on the use of the five major classes of antihypertensive drugs between 1978 and 2002 show interesting trends (Fig. 1). In the late 70s and early 80s, diuretics and betablockers were the main antihypertensives on the market. The use of diuretics peaked in the early 80s at about 60%. This market share dropped markedly over the next decade but has largely stayed at around 20% over the past 10 years. The beta-blockers (BBs) peaked at 30% during the early 80s and fell by half over the next decade. Their use increased moderately during the latter part of the 90s. The ACE inhibitors and calcium channel blockers (CCBs), introduced in the mid-80s, did very well and passed the diuretics in the early 90s (just as ALLHAT was being planned). Since the mid-90s, ACE inhibitors have seen a small increase, while the CCBs have dropped from approximately 35% to 25%. Recently, the use of angiotensin receptor blockers (ARBs) has grown rapidly. Fig. 1 Hypertension Treatment by Drug Class in the U.S. 1978-2002 60 % of Treated Patients on Medication 1. 50 Calcium Channel Blockers Beta Blockers Diuretics ACE Inhibitors ARBs Diuretics 40 30 ß-Blocker 20 ACE Inhibitors 10 CCBs ARBs 0 1978 1980 1982 1984 1986 1988 1990 1992 1994 1996 1998 2000 2002 Year IMS Health NDTI, 1978-2002 1 * For the purposes of this paper, the terms “low-dose” and “low-to-moderate dose” will both refer to 12.5mg - 25mg chlorthalidone or 25mg - 50mg hydrochlorothiazide. The term “lowdose” was used for this range in past studies; the term “low-to-moderate dose” is more accurately used for this range today. -2- 2. FDA-approved Diuretics Examples of available diuretic tablets or capsules (excluding the loop diuretics) according to PDR 2004 (used alone or in combination in large clinical outcome trials): a. THIAZIDE & RELATED DIURETICS • Chlorothiazide • Chlorthalidone • Hydrochlorothiazide • Indapamide b. COMBINATION DIURETIC AND OTHER ANTIHYPERTENSIVE DRUG • Combinations of thiazides and an ACE inhibitor, ARB, BB or CCB c. POTASSIUM-SPARING DIURETICS • triamterene • amiloride d. COMBINATION DIURETICS • Combinations of HCTZ and a potassium-sparing diuretic The JNC7 contains a more inclusive list of antihypertensive medications that are marketed in the United States (1, 2). 3. Diuretics and BP Lowering In their recent review of 354 trials of BP-lowering drugs, Law and co-workers (3) concluded that the major categories of drugs “gave similar BP reductions.” The mean placebo-adjusted reduction was 9.1 mm Hg (95% CI 8.8 to 9.3) systolic and 5.5 mm Hg (CI 5.4 to 5.7) diastolic at standard doses (“usual maintenance doses”)...” According to available scientific evidence, diuretics are as effective as other classes of antihypertensive drugs in lowering elevated BP compared to placebo. The BP results by treatment group in ALLHAT, an active controlled trial, showed that chlorthalidone (12.5-25 mg) as first-line therapy in a step-up treatment regimen was superior compared to amlodipine (2.5-10 mg) and lisinopril (10-40 mg/day) in lowering systolic BP and amlodipine was superior in lowering diastolic BP (Fig 2)(4). -3- Fig 2. ALLHAT - BP Results by Treatment Group and Annual Visit BP Results by Treatment Group Chlorthalidone Amlodipine Lisinopril 150 90 SBP DBP 85 mm Hg BP mm Hg BP 145 140 80 75 135 70 130 0 1 2 3 4 5 6 0 1 2 Years 3 Years 4 5 Compared to chlorthalidone: Compared to chlorthalidone: SBP significantly higher in the amlodipine group (~1 mm Hg) and the lisinopril group (~2 mm Hg). DBP significantly lower in the amlodipine group (~1 mm Hg). 6 As first-line drugs, thiazide diuretics are at least as effective in lowering elevated BP as two of the most commonly used antihypertensive drugs (amlodipine and lisinopril) in the U.S. Most patients who are hypertensive will require two or more antihypertensive medications to achieve their BP goals (1,2). 4. Diuretics and Event Reduction: Placebo-Controlled Trials Since the first VA Cooperative trial published in 1967, thiazide-type diuretics have been the basis of antihypertensive therapy in the majority of placebo-controlled outcome trials in which CVD events, including strokes, CHD, and HF have been reduced by BP lowering. (2) A comprehensive meta-analysis (5) of 18 placebo-controlled trials (one with a usual care control) reported through 1995 compared three regimens: high-doses diuretics (> 50 mg/day), low-to-moderate dose diuretics and beta-blockers. No large, long-term placebocontrolled clinical trials evaluating CCBs or ACE inhibitors in hypertension had been completed at that time. The risk reduction for stroke, coronary heart disease, congestive heart failure and all-cause mortality are shown in Figure 3. Compared to low-tomoderate dose diuretics, high-dose diuretics were more effective in lowering the risks of stroke and heart failure, but much less effective in reducing CHD risk. The likely explanation for the difference in effect on CHD is discussed below (section 5). Betablockers were as effective as low-to-moderate dose diuretics in reducing stroke and heart failure, but also less effective for CHD. -4- Risk reduction % Fig. 3 Meta-analysis: Event Reduction in Placebo-Controlled Trials Through 1995. 0 Stroke CHD Death CHF * -20 -40 -60 * * * * * * *p<0.05 -80 low dose diuretics high dose diuretics Betablockers * Psaty et al., JAMA 1997;277:739 Placebo-controlled trials of a variety of diuretics demonstrated that this class of drug is very effective in reducing the risk of cardiovascular complications. The risk-benefit balance favors low-dose over high-dose diuretics. An updated review published in the JAMA in May, 2003 used a new technique called network meta-analysis (6). This review included both placebo-controlled and actively controlled trials. The findings comparing low-to-moderate dose diuretics to placebo are remarkable (Fig.4). The variety of diuretics tested markedly reduced the risk of all cardiovascular complications - heart failure by 50%, stroke by 30%, combined cardiovascular (CV) events by 25% and CHD and CV mortality each by 20%. Fig 4. Network Meta-analysis - Major Outcomes: Low-Dose Diuretics vs. Placebo Outcome RR 95% CI p CHD 0.79 0.69-0.92 0.002 Heart failure 0.51 0.42-0.62 <0.001 Stroke 0.71 0.63-0.81 <0.001 CVD events 0.76 0.69-0.83 <0.001 CVD mortality 0.81 0.73-0.92 0.001 Total mortality 0.90 0.84-0.96 0.002 0.40 0.65 0.90 Low-dose diuretics better 1.15 1.40 Low-dose diuretics worse Psaty et al., JAMA 2003;289:2534-2544 -5- The findings from the network meta-analysis of the chlorthalidone trials and those of the non-chlorthalidone trials are shown in Fig 5. (7) Fig. 5. Comparisons of Low-Dose Chlorthalidone vs. Placebo (left panel) and Low-Dose “Non-Chlorthalidone” vs. Placebo (right panel) Clinical Effects of Diuretics by Type in Placebo-Controlled Trials Low-dose Chlorthalidone Other Thiazide Diuretics Direct Comparisons Direct Comparisons Outcome RR (95% CI) CHD 0.74 (0.58 - 0.95) CHD Stroke 0.64 (0.51 - 0.80) Stroke CHF 0.53 (0.39 - 0.73) CHF CVD events 0.70 (0.61 - 0.80) CVD events 0.76 (0.66 - 0.87) CVD mortality 0.80 (0.61 - 1.04) CVD mortality 0.79 (0.65 - 0.94) Total mortality 0.89 (0.75 - 1.06) Total mortality 0.91 (0.79 - 1.03) 0.40 0.60 Low-dose chlorthalidone better 0.80 1.00 1.20 Low-dose chlorthalidone worse Outcome RR (95% CI) 0.72 (0.54 - 0.95) 0.71 (0.60 - 0.85) No Data 0.40 0.60 0.80 Other thiazide diuretic better 1.00 1.20 Other thiazide diuretic worse Psaty et al., JAMA 2004;292:43-4 The health benefit of low-dose diuretics is substantial and applies to thiazide diuretics as a class. 5. Diuretics and Event Reduction: Active-Controlled Trials In the network meta-analysis (6), low-to-moderate dose diuretics were also compared to 5 other classes of antihypertensive drugs (Fig. 6). With 6 outcomes, there were a total of 30 comparisons and the conclusions are striking: “...none of the other first-line treatment strategies -- -blockers, ACE inhibitors, CCBs, α-blockers, and ARBs -- was significantly better than low-dose diuretics for any major cardiovascular disease outcome. In 8 of the 30 between-drug comparisons, however, low-dose diuretics were significantly better than other treatments for the prevention of cardiovascular disease health outcomes. Among nonsignificant, betweendrug comparisons, 13 favored low-dose diuretics, 5 favored other therapies, and 4 were indifferent.” (6) The asterisks placed after the specific outcomes in Figs. 6A-D indicate that the comparator drugs were significantly better than placebo for that outcome. -6- Fig. 6A. Low-Dose Diuretics vs. Beta-Blockers Outcome RR 95% CI p CHD 0.87 0.74-1.03 0.10 Heart failure* 0.83 0.68-1.01 0.07 Stroke* 0.90 0.76-1.06 0.20 CVD events* 0.89 0.80-0.98 0.02 CVD mortality* 0.93 0.81-1.07 0.34 Total mortality* 0.99 0.91-1.07 0.73 0.40 0.65 0.90 1.15 Low-dose diuretics better 1.40 Low-dose diuretics worse Fig. 6B. Low-Dose Diuretics vs. ACE Inhibitors Outcome RR 95% CI p CHD* 1.00 0.88-1.14 0.99 Heart failure* 0.88 0.80-0.96 0.01 Stroke* 0.86 0.77-0.97 0.01 CVD events* 0.94 0.89-1.00 0.04 CVD mortality* 0.93 0.85-1.02 0.13 Total mortality* 1.00 0.95-1.05 0.86 0.40 0.65 0.90 Low-dose diuretics better 1.15 1.40 Low-dose diuretics worse Fig. 6C. Low-Dose Diuretics vs. CCBs Outcome RR 95% CI p CHD 0.89 0.76-1.01 0.07 Heart failure* 0.74 0.67-0.81 <0.001 Stroke* 1.02 0.91-1.14 0.74 CVD events* 0.94 0.89-1.00 0.045 CVD mortality* 0.95 0.87-1.04 0.29 Total mortality* 1.03 0.98-1.08 0.30 0.40 0.65 0.90 Low-dose diuretics better -7- 1.15 1.40 Low-dose diuretics worse Fig. 6D. Low-Dose Diuretics vs. ARBs Outcome RR 95% CI p CHD 0.83 0.59-1.16 0.28 Heart failure* 0.88 0.66-1.16 0.36 Stroke* 1.20 0.93-1.55 0.16 CVD events* 1.00 0.85-1.18 0.98 CVD mortality* 1.07 0.85-1.36 0.55 Total mortality* 1.09 0.96-1.22 0.18 0.40 0.65 0.90 Low-dose diuretics better 1.15 1.40 Low-dose diuretics worse Fig. 6E. Low-Dose Diuretics vs. α-Blockers Outcome RR 95% CI p CHD 0.99 0.75-1.31 0.97 Heart failure 0.51 0.43-0.60 <0.001 Stroke 0.85 0.66-1.10 0.22 CVD events 0.84 0.75-0.93 0.001 CVD mortality 1.00 0.75-1.34 1.00 Total mortality 0.98 0.88-1.10 0.79 0.40 0.65 0.90 Low-dose diuretics better 1.15 1.40 Low-dose diuretics worse “This network meta-analysis provides compelling evidence that low-dose diuretics are the most effective first-line treatment for preventing the occurrence of cardiovascular disease morbidity and mortality.” 6. Diuretics and Event Reduction by Subgroup The prevalence, severity, and impact of hypertension are increased in Blacks, who also demonstrate somewhat reduced BP responses to monotherapy with β-blockers, ACE inhibitors, or ARBs compared with diuretics or CCBs. These differential responses are largely eliminated by drug combinations that include adequate doses of a diuretic.(1) Four subgroup analyses were pre-specified in the ALLHAT protocol. For age (< 65 and > 65), gender and diabetes status at baseline, there were no statistically significant interactions. Thus, the overall amlodipine/chlorthalidone and lisinopril/chlorthalidone -8- findings also applied to these subgroups. In contrast, statistically significant interactions were observed for two outcomes, stroke and combined CVD, when the data were analyzed by race, black vs. non-black (Fig. 7). Chlorthalidone was superior to lisinopril for the prevention of HF and combined CVD in non-blacks, and of stroke, HF, combined CHD, and combined CVD in blacks. Only part of the excess risk in blacks can be explained by a difference in achieved systolic BP. The chlorthalidone-lisinopril difference in mean systolic BP at 5 years was > 4 mm Hg for blacks and < 1 mm Hg for non-blacks. Fig. 7. Clinical Outcomes - Blacks and Non-Blacks, Lisinopril vs. Chlorthalidone Clinical Outcomes – Blacks and Non-Blacks Lisinopril/Chlorthalidone Blacks Non-Blacks NFMI + CHD Death 1.10 (0.94 - 1.28) 0.94 (0.85 - 1.05) All-Cause Mortality 1.06 (0.95 - 1.18) 0.97 (0.89 - 1.06) Combined CHD 1.15 (1.02 - 1.30) 1.01 (0.93 - 1.09) Combined CVD * 1.19 (1.09 - 1.30) 1.06 (1.00 - 1.13) Stroke * 1.40 (1.17 - 1.68) 1.00 (0.85 - 1.17) Heart Failure 1.32 (1.11 - 1.58) 1.15 (1.01 - 1.30) ESRD 1.29 (0.94 - 1.75) 0.93 (0.67 - 1.30) 0.50 Favors Lisinopril 1 2 Favors Chlorthalidone 0.50 Favors Lisinopril 1 2 Favors Chlorthalidone * p for interaction <.05 Diuretics are more effective than ACE inhibitors in reducing the risk of HF and combined CVD in non-black hypertensives and markedly more effective than ACE inhibitors in reducing systolic BP and the risk of stroke, HF and combined CVD and modestly more effective in reducing combined CHD in black hypertensives. 7. Adverse Events a. Hypokalemia Until the early 90s, thiazide diuretics were often prescribed in high doses, e.g., >50-100 mg/day of hydrochlorothiazide or chlorthalidone. Adverse drug reactions, for example hypokalemia, were more common with these dosages. Ventricular arrhythmias were also reported with high doses of diuretics. Siscovick et al. (8) documented in a lead article in the New England Journal of Medicine, a strong association between high doses of thiazide diuretics and primary cardiac arrest. The addition of potassium-sparing diuretics or lower doses of thiazide diuretics reduced the risk of cardiac arrest. This article contributed to the shift from higher to lower doses of diuretics in the mid-90s, and -9- it may explain the findings that overall high-dose diuretics were not associated with a reduced risk of CHD in the clinical trials. There are also other possible explanations. Hyperglycemia It has been known for decades that thiazide diuretics are associated with an increased risk of the development of diabetes. At lower doses of chlorthalidone (12.5-25 mg/day), this effect is modest. Fig. 8 shows mean fasting glucose levels among three subgroups of ALLHAT patients - non-diabetic, those with impaired fasting glucose (IFG) and diabetics by treatment. The mean levels at baseline were similar in all three subgroups. Among the non-diabetic participants, fasting glucose increased in all treatment groups (Fig. 8A), probably due to weight gain as well as aging. The increase was slightly higher (2-4 mg/dL) in the diuretic group. In the IFG group, increases were seen in both the chlorthalidone and amlodipine groups (Fig. 8B). No changes were observed in the lisinopril group. Among the diabetics, fasting glucose decrease was slower in the chlorthalidone group (Fig. 8C). At 4 years, there was no significant difference between the three groups. Fig. 8. Fasting Glucose Among Non-diabetics, Participants with IFG and Diabetics by Treatment Group A. Fasting Glucose Among Nondiabetic Participants Fasting Glucose (mg/dL) b. 140 130 120 110 * * 100 * * Chlor Amlod Lisin 90 80 Baseline 2 Years 4 Years Chlor 90.8 99.3 102.2 Amlod 90.7 96.3 99.5 Lisin 90.8 95.1 98.4 * p<.05 compared to chlorthalidone 1 - 10 - B. Fasting Glucose (mg/dL) Fasting Glucose Among Participants with IFG at Baseline 140.0 130.0 * 120.0 * * 110.0 100.0 Chlor Amlod Lisin 90.0 80.0 Baseline 2 Years 4 Years Chlor 116.0 129.7 129.2 Amlod 115.6 122.6 130.5 Lisin 116.2 115.8 116.7 * p<.05 compared to chlorthalidone 2 C. Fasting Glucose (mg/dL) Fasting Glucose Among Diabetic Participants 180.0 170.0 160.0 150.0 140.0 130.0 120.0 110.0 100.0 90.0 80.0 * * Chlor Amlod Lisin Baseline 2 Years 4 Years Chlor 169.0 170.6 163.8 Amlod 167.3 161.2 160.5 Lisin 168.3 161.2 159.0 * p<.05 compared to chlorthalidone 3 Thiazide diuretics have a modest diabetogenic effect. Metabolic ward studies in the U.S. and long-term clinical studies reported mainly from Europe suggest that the drug effect on fasting glucose is linked to the potassium level. Patients who maintain normal plasma and body levels of potassium rarely develop diabetes. Additionally, restoration of low potassium levels through supplementation or withdrawal of the diuretic often leads to normalization of the glucose level. Thus, drug-induced diabetes appears to be more reversible than “naturally occurring” diabetes; sustained weight loss will probably reverse any early Type 2 diabetes. - 11 - c. Outcomes by Diabetes Status Thiazide diuretics, β-blociers, ACE inhibitors, ARBs, and CCBs are beneficial in reducing CVD and stroke incidence in patients with diabetes.(1) Stratified analysis of the ALLHAT database by diabetes status - Lisinopril vs. chlorthalidone is shown in Fig. 9. Fig. 9. Outcomes by Diabetes Status - Lisinopril vs. Chlorthalidone Diabetics & Nondiabetics (History) Lisinopril/Chlorthalidone Relative Risk and 95% Confidence Intervals Nondiabetics Diabetics CHD 1.00 (0.87, 1.14) 0.99 (0.88, 1.11) Mortality 1.02 (0.91, 1.13) 1.00 (0.91, 1.09) Stroke 1.07 (0.90, 1.28) 1.23 (1.05, 1.44) Heart Failure 1.22 (1.05, 1.42) 1.20 (1.04, 1.38) Combined CVD 1.08 (1.00, 1.17) 1.12 (1.04, 1.19) ESRD 1.17 (0.87, 1.57) 1.05 (0.74, 1.48) 0.50 Favors Lisinopril 1 2 Favors Chlorthal 0.50 Favors Lisinopril 1 There is no difference in treatment group effect by baseline history of diabetes. 2 Favors Chlorthal 1 JAMA 2002;288:2981-2997 There is no evidence in ALLHAT that diuretics are less effective in diabetic than non-diabetic hypertensives during an average follow-up of approximately 5 years. d. Effect of incident diabetes and changes in fasting glucose on endpoints A recent paper from the SHEP study, in which mortality data were evaluated for those with diabetes at baseline, those who developed diabetes during the trial, and those who did not develop diabetes, indicated that: • • • Chlorthalidone based treatment of hypertension results in improved long-term outcomes. The diabetes related to chlorthalidone therapy has better prognosis than diabetes at baseline. The benefit of chlorthalidone-based therapy on long-term total and CV mortality is most pronounced in hypertensive patients with diabetes.(10) - 12 - In addition, unpublished ALLHAT data show that change in fasting glucose among those without baseline diabetes is not associated with CVD outcomes during the trial. 8. Diuretics and Drug Adherence It is often stated that drug adherence with diuretics is a major issue. The source of this claim is not known. It may be a carry-over from the time when high doses of thiazide diuretics (>50-100 mg) were used. With low-to-moderate dose diuretics (initial doses of 12.5 or 25 mg), drug adherence is comparable to that of other classes of antihypertensive drugs (2). The drug adherence data from ALLHAT are robust. 15,255 high-risk hypertensives were randomized to chlorthalidone and were followed for an average of almost 5 years. After 5 years, more than 80% of the patients stayed on chlorthalidone and/or a non-study diuretic (Fig. 10). Adherence was not different than with amlodipine, but adherence was better in the diuretic group than among those assigned to lisinopril. Fig. 10. ALLHAT - Drug Adherence by Treatment Group and Annual Visit Drug Adherence* by Treatment 100.0 80.0 60.0 % 40.0 20.0 0.0 1 Year 2 Years 3 Years 4 Years 5 Years Chlor 87.1 84.7 82.7 80.8 80.5 Aml 87.6 85.2 83.2 80.5 80.4 Lis 82.4 78.4 77.1 74.8 72.6 *Step 1 or equivalent treatment Long-term adherence to low-dose diuretics is as good as or better than for the other commonly used antihypertensive agents. - 13 - 9. Drug Cost The drug costs for thiazide diuretics to the patient (Costco, a large volume retailer) and the average wholesale prices (AWP) are much lower compared to branded Norvasc and generic lisinopril. Since chlorthalidone is approximately twice as potent as hydrochlorothiazide, 25 mg chlorthalidone is equivalent to 50 mg hydrochlorothiazide. (7) Chlorthalidone (25 mg) Hydrochlorothiazide (50 mg) Norvasc (10 mg) Zestril (40 mg) Generic Lisinopril (40 mg)** Patient cost / 30 tablets (Costco.com 6/22/2005)(11) $5.99 (MYL)* $5.79 (QUA) $60.47 (PFI) $52.49 (ZEN) $24.99 AWP / 100 tablets (Redbook 2004 – lowest)(12) $6.75 (Consol. Midland) $2.75 (Consol. Midland) $217.62 (PFI) $178.03 (ZEN) $77.00 (Major) *Manufacturer listed in parentheses. **Not available at Costco.com. Patient cost is from Drugstore.com, where the manufacturer is not available. Higher cost is justified if a drug offers added value. Chlorthalidone was unsurpassed as first-line therapy by amlodipine and lisinopril in terms of BP reduction and drug adherence over 5 years and compared favorably for reduction in risk of at least one major CV complication of hypertension. The cost of care is among the barriers that must be overcome to achieve goal BP.(1) 10. ALLHAT Recommendations Thiazide-type diuretics should be considered for nearly all patients with hypertension (2): Untreated patients Inadequately controlled patients on non-diuretic agent(s) 11. JNC 7 (2003) (1,2) “Thiazide-type diuretics should be used in drug treatment for most patients with hypertension, either alone or combined with other drugs from other classes.” (8,9) Most patients require two or more drugs to achieve BP control Almost half of the patients have a compelling indication. These include heart failure, post myocardial infarction, high CAD risk, diabetes, chronic kidney disease, and recurrent stroke prevention. - 14 - 12. References 1. Chobanian AV, Bakris GL, Black HR, Cushman WC, Green LA, Izzo Jr. JL, Jones DW, Materson BJ, Oparil S, Wright Jr. JT, Roccella EJ and the National High Blood Pressure Education Program Coordinating Committee. The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure. The JNC 7 Report. JAMA 2003;289:2560-2572. 2. Chobanian AV, Bakris GL, Black HR, Cushman WC, Green LA, Izzo Jr. JL, Jones DW, Materson BJ, Oparil S, Wright Jr. JT, Roccella EJ and the National High Blood Pressure Education Program Coordinating Committee. Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure. Hypertension 2003;42:1206-1252. 3. Law MR, Wald NJ, Morris R, Jordan RE. Value of low dose combination treatment with blood pressure lowering drugs: analysis of 354 randomised trials. BMJ 2003;326:1427-1434. 4. The ALLHAT Officers and Coordinating for the ALLHAT Collaborative Research Group. Major outcomes in high-risk hypertensive patients randomized to angiotensin-converting enzyme inhibitor or calcium channel blocker vs. diuretic. The ALLHAT and Lipid-Lowering Treatment to Prevent Heart Attack Trial (ALLHAT). JAMA 2002;288:2981-2997. 5. Psaty BM, Smith NL, Siscovick DS, Koepsell TD, Weiss NS, Heckbert SR, Lemitre RN, Wagner EH, Furberg CD. Health outcomes associated with antihypertensive therapies used as first-line agents. JAMA 1997;277:739-745. 6. Psaty BM, Lumley T, Furberg CD, Schellenbaum G, Pahor M, Alderman MH, Weiss NS. Health outcomes associated with various antihypertensive therapies used as firstline agents. A network meta-analysis. JAMA 2003;289:2534-2544. 7. Psaty BM, Lumley T, Furberg CD. Meta-analysis of health outcomes of chlorthalidone-based versus non-chlorthalidone-based low-dose diuretic therapies. [Research Letter]. JAMA 2004;292:43-44. 8. Siscovick DS, Raghunathan TE, Psaty BM, Koepsell TD, Wicklund KG, Lin X, Cobb L, Rautaharju PM, Copass MK, Wagner EH. Diuretic therapy for hypertension and the risk of primary cardiac arrest. N Engl J Med 1994;330;1852-1857. 9. Carter BL, Ernst ME, Cohen JD. Hydrochlorothiazide versus chlorthalidone. Evidence supporting their interchangeability. Hypertension 2004;43:4-9. 10. Kostis JB, Wilson AC, Freudenberger RS, Cosgrove NM, Pressel SL, Davis BR for the SHEP Collaborative Research Group. The Long-Term Effect of Diuretic-Based Therapy on Fatal Outcomes in Subjects with Isolated Systolic Hypertension With and Without Diabetes. Am J Cardiol 2005;95:29-35. 11. Costco.com, referenced June 22, 2005. 12. Drug Topics Red Book. Medical Economics Co., Inc., Montvale, NJ, 2004. - 15 -