Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Pharmaceutical industry wikipedia , lookup
Discovery and development of direct thrombin inhibitors wikipedia , lookup
Clinical trial wikipedia , lookup
Prescription costs wikipedia , lookup
Adherence (medicine) wikipedia , lookup
Drug interaction wikipedia , lookup
Drug-eluting stent wikipedia , lookup
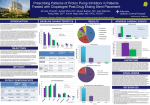
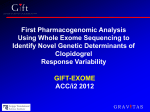
JACC: CARDIOVASCULAR INTERVENTIONS VOL. 6, NO. 12, 2013 ª 2013 BY THE AMERICAN COLLEGE OF CARDIOLOGY FOUNDATION PUBLISHED BY ELSEVIER INC. ISSN 1936-8798/$36.00 http://dx.doi.org/10.1016/j.jcin.2013.06.014 Concomitant Administration of Clopidogrel With Statins or Calcium-Channel Blockers Insights From the TRITON–TIMI 38 (Trial to Assess Improvement in Therapeutic Outcomes by Optimizing Platelet Inhibition With Prasugrel– Thrombolysis In Myocardial Infarction 38) Oluseyi Ojeifo, MD,* Stephen D. Wiviott, MD,y Elliott M. Antman, MD,y Sabina A. Murphy, MPH,y Jacob A. Udell, MD,z Eric R. Bates, MD,x Jessica L. Mega, MD, MPH,y Marc S. Sabatine, MD, MPH,y Michelle L. O’Donoghue, MD, MPHy Boston, Massachusetts; Toronto, Ontario, Canada; and Ann Arbor, Michigan Objectives This study sought to evaluate the clinical relevance of potential clopidogrel drug–drug interactions. Background Some studies have demonstrated that statins and calcium-channel blockers (CCBs) may attenuate the pharmacodynamic effects of clopidogrel. Methods The TRITON–TIMI 38 (Trial to Assess Improvement in Therapeutic Outcomes by Optimizing Platelet Inhibition With Prasugrel–Thrombolysis in Myocardial Infarction 38) enrolled 13,608 patients with an acute coronary syndrome (ACS) and planned percutaneous coronary intervention (PCI), and randomized them to clopidogrel or prasugrel. Use of a statin or CCB was left to the discretion of the treating physician. A multivariable Cox model with propensity score was employed to evaluate the association between statin or CCB use and clinical outcomes. Results Of the 6,795 subjects assigned to clopidogrel, 4,794 (70.6%) were on a CYP3A4-metabolized statin, and 966 (14.2%) were on a CCB at randomization. The risk of cardiovascular (CV) death, myocardial infarction (MI), or stroke was similar regardless of baseline use of statins (adjusted hazard ratio [HR]: 1.02, 95% confidence interval [CI]: 0.85 to 1.22) or CCBs (adjusted HR: 1.16; 95% CI: 0.94 to 1.43) in clopidogrel-treated patients. Further, the combined use of a CCB and atorvastatin 80 mg daily (adjusted HR: 0.82; 95% CI: 0.37 to 1.84), or a CCB, statin, and proton pump inhibitor (adjusted HR: 1.04; 95% CI: 0.70 to 1.54) were not associated with an increased risk of CV death, MI, or stroke. The use of statins or CCBs did not modify the relative efficacy of prasugrel versus clopidogrel for the primary endpoint (p for interaction ¼ 0.43, 0.55, respectively). Conclusions In patients with ACS undergoing PCI, the use of statins or CCBs was not associated with an increased risk of CV events in clopidogrel-treated patients. Consistent results were observed when the drugs were administered alone, together, or in combination with proton pump inhibitors. (J Am Coll Cardiol Intv 2013;6:1275–81) ª 2013 by the American College of Cardiology Foundation From the *Department of Medicine, Massachusetts General Hospital, Boston, Massachusetts; yTIMI Study Group, Cardiovascular Division, Brigham and Women’s Hospital, Boston, Massachusetts; zDivision of Cardiology, Women’s College Hospital, University of Toronto, Toronto, Ontario, Canada; and the xDepartment of Internal Medicine, University of Michigan, Ann Arbor, Michigan. Dr. Wiviott is a consultant for Angelmed, Eisai, Aegerion, Janssen Pharmaceuticals, St. Jude Medical, and Xoma; and has received research funding from Merck & Co., Eisai, AstraZeneca, and Eli Lilly and Company/Daichi Sankyo. Dr. Antman has received research funding from Eli Lilly and Company and Daiichi Sankyo. Ms. Murphy has received research funding from Eli Lilly and Company. Dr. Bates is on the advisory boards of Daichi Sankyo, AstraZeneca, Eli Lilly and Company, and Sanofi-aventis. Dr. Mega has received research funding from Jannsen Pharmaceuticals, Bayer HealthCare, AstraZeneca, Eli Lilly and Company, Daiichi Sankyo, Bristol-Myers Squibb, and Sanofiaventis; and is a consultant for Boehringer Ingelheim and Janssen Pharmaceuticals. Dr. Sabatine has received research funding through Brigham and Women’s Hospital from Abbott Laboratories, Amgen, AstraZeneca, AstraZeneca/Bristol-Myers Squibb Alliance, Critical Diagnostics, Daiichi-Sankyo, Eisai, Genzyme, GlaxoSmithKline, Intarcia, Merck, Roche Diagnostics, Sanofi-aventis, and Takeda; and is a consultant for Aegerion, Amgen, AstraZeneca/Bristol-Myers Squibb Alliance, Intarcia, Pfizer, Sanofi-aventis, and Vertex. Dr. O’Donoghue has received research funding from GlaxoSmithKline and AstraZeneca and is a consultant for Aegerion. All other authors have reported that 1276 Ojeifo et al. Clopidogrel and Drug Interactions Statins and calcium-channel blockers (CCBs) are frequently co-administered with clopidogrel after an acute coronary syndrome (ACS). Because clopidogrel requires hepatic metabolism via the cytochrome P450 (CYP) enzyme system to form its active metabolite, there exists concern that certain drugs, such as statins or CCBs, that are metabolized by or inhibit isoenzymes along this pathway, can interfere with the clinical efficacy of clopidogrel. See page 1282 These concerns are supported by studies that have demonstrated that atorvastatin (1–3) or CCBs (4–6) can attenuate the pharmacodynamic effects of clopidogrel in vitro; however, the results from pharmacodynamic studies remain mixed (7) and the clinical implications of these findings remain unclear. We therefore assessed whether statins or CCBs interfere with the clinical efficacy of clopidogrel in a large trial population of patients with ACS undergoing percutaneous coronary intervention (PCI). FurAbbreviations and Acronyms ther, we assessed the relative efficacy and safety of prasugrel ACS = acute coronary versus clopidogrel in those syndrome subjects who were treated with CCB = calcium-channel statins or CCBs. blocker CI = confidence interval CV = cardiovascular Methods HR = hazard ratio The TRITON–TIMI 38 (Trial to Assess Improvement in TherPCI = percutaneous coronary apeutic Outcomes by Optimizintervention ing Platelet Inhibition With Prasugrel–Thrombolysis in Myocardial Infarction 38) study was a double-blind, phase 3 trial that enrolled 13,608 patients with moderate-to-high-risk ACS undergoing planned PCI, and randomized them to prasugrel (60-mg loading dose, 10 mg a day maintenance dose) or clopidogrel (300-mg loading dose, 75 mg a day maintenance dose) for a median duration of 14.5 months (8). The primary endpoint of the TRITON–TIMI 38 trial was the composite of cardiovascular (CV) death, nonfatal myocardial infarction (MI), or nonfatal stroke. Relevant exclusions to participation in the trial included an increased risk of bleeding, a history of anemia, thrombocytopenia, or pathological intracranial findings. Statin or CCB use. The decision to treat with a statin or CCB was left to the discretion of the treating physician. The names (brand name or generic), doses, and start and stop MI = myocardial infarction they have no relationships relevant to the contents of this paper to disclose. The TRITON–TIMI 38 trial was sponsored by Daiichi Sankyo and Eli Lilly and Company. The current analysis received no sources of external funding. The TIMI JACC: CARDIOVASCULAR INTERVENTIONS, VOL. 6, NO. 12, 2013 DECEMBER 2013:1275–81 dates of concomitant medications were captured on the case report forms at patient visits. For the current analysis, we defined statin use as all statins that were known to be metabolized by the CYP3A4 enzyme system, including atorvastatin, simvastatin, cerivastatin, and lovastatin. On the basis of prior pharmacodynamic studies (1–3), we also examined atorvastatin use individually in a sensitivity analysis. CCB use was defined as any of the following subtypes that are metabolized by or inhibit the CYP3A4 isoenzyme, including diltiazem, verapamil, nifedipine, felodipine, amlodipine, nisoldipine, isradipine, nimodipine, nicardipine, lercanidipine, nitrendipine, bepridil, lacidipine, barnidipine, and azelnidipine. All primary efficacy and key safety endpoints were adjudicated by an independent clinical events committee who were unaware of the assigned treatment; however, the use of concomitant medications including CCBs and statins was not concealed. For the current analysis, stent thrombosis was defined according to the Academic Research Consortium (ARC) definite or probable definitions (9). Statistical analysis. Baseline characteristics are presented as medians (interquartile ranges) for continuous variables and frequencies for categorical variables. Comparisons for baseline characteristics were made with Wilcoxon rank sum tests for continuous variables and chi-square tests for categorical variables. Multivariable Cox proportional hazards model was used to examine the independent association between use of a statin and/or CCB and the risk of adverse outcomes for patients on clopidogrel. Using logistic regression modeling with a forward selection algorithm (p for inclusion < 0.20), propensity scores were developed to account for the clinician’s decision to treat with a statin or CCB. The final variables included in each propensity score and multivariable models are included in the Online Appendix. Because patients could start or stop medications during the course of study, we conducted sensitivity analyses that were restricted to those subjects on a concomitant medication of interest both at randomization and at the end of the study. All efficacy analyses comparing prasugrel with clopidogrel were conducted according to the intention-to-treat principle. Rates of endpoints are expressed as Kaplan-Meier estimates at 450 days. All tests were 2-sided with a significance value of p < 0.05. Analyses were performed with Stata version 9.2 (Stata Corp., College Station, Texas). Results Of the 13,608 patients enrolled in the TRITON–TIMI 38 trial, 9,580 (70.4%) were recorded to be taking Study Group has an independent copy of the trial database and conducted the current analysis. Manuscript received April 29, 2013; accepted June 21, 2013. Ojeifo et al. Clopidogrel and Drug Interactions JACC: CARDIOVASCULAR INTERVENTIONS, VOL. 6, NO. 12, 2013 DECEMBER 2013:1275–81 1277 Table 1. Baseline Characteristics Stratified by Use of a CYP3A4-Metabolized Statin or CCB CCB at Randomization (n ¼ 1,972) No CCB at Randomization (n ¼ 11,636) p Value Statin at Randomization (n ¼ 9,580) No Statin at Randomization (n ¼ 4,028) p Value Age 75 yrs 19.2 Male 70.7 12.3 <0.001 12.2 16.0 <0.001 74.7 <0.001 74.8 72.5 White race 91.4 <0.001 92.7 0.054 91.9 94.0 <0.001 30.6 34.2 <0.001 Region North America 40.9 30.1 <0.001 South America 2.4 4.2 4.4 2.8 Western Europe 20.8 27.0 24.7 29.6 Eastern Europe 15.2 26.0 24.7 23.7 Rest of the World 20.7 12.7 15.7 9.7 28.7 (25.7–32.2) 27.7 (25.1–30.9) <0.001 27.8 (25.2–31.2) 27.6 (24.9–30.8) Current tobacco use 30.8 39.4 <0.001 38.4 37.6 0.38 Hypertension 82.4 61.2 <0.001 64.6 63.3 0.15 BMI, kg/m2 <0.001 Hypercholesterolemia 64.6 54.2 <0.001 59.1 47.6 <0.001 Diabetes mellitus 31.5 21.7 <0.001 24.1 20.7 <0.001 Peptic ulcer disease 6.3 5.9 0.48 6.2 5.5 0.11 Carotid or vertebral arterial disease 4.7 2.6 <0.001 2.8 3.1 0.36 History stroke or TIA 6.2 3.4 <0.001 3.8 3.9 0.65 History of peripheral arterial disease 8.8 4.6 <0.001 5.4 4.9 0.32 Prior MI 23.9 16.9 <0.001 19.1 15.0 <0.001 Prior CABG 12.2 6.9 <0.0001 8.2 6.3 <0.001 Creatinine clearance <60 ml/min/m2 15.2 10.4 <0.001 10.3 13.2 <0.001 Index diagnosis of NSTEMI or UA 85.2 72.1 <0.001 75.2 71.2 <0.001 ACEI/ARB at randomization 68.3 54.1 <0.001 60.8 45.0 <0.001 Beta-blocker at randomization 70.7 74.5 <0.001 77.5 65.5 <0.001 Aspirin at randomization 97.3 96.6 0.12 97.6 94.6 <0.001 Randomized to prasugrel 51.0 49.9 0.36 50.0 50.3 0.70 Values are % or median (interquartile range). ACEI ¼ angiotensin-converting enzyme inhibitor; ARB ¼ angiotensin receptor blocker; BMI ¼ body mass index; CABG ¼ coronary artery bypass graft surgery; CCB ¼ calcium-channel blocker; MI ¼ myocardial infarction; NSTEMI ¼ non–ST-segment elevation myocardial infarction; PCI ¼ percutaneous coronary intervention; TIA ¼ transient ischemic attack; UA ¼ unstable angina. a CYP3A4-metabolized statin, and 1,972 (14.5%) were recorded to be taking a CCB at the time of randomization. The baseline characteristics for patients who were or were not taking statins or CCBs are shown in Table 1. The frequency of use of the different types of CYP3A4-metabolized statins and CCBs is included in Online Tables 1 and 2. Patients on a CYP3A4-metabolized statin were more likely to be younger, male, and have an index diagnosis of a non– ST-segment elevation ACS compared with patients not on a statin (Table 1). Subjects treated with a statin were more likely to have a history of hyperlipidemia, diabetes mellitus, and prior MI or coronary artery bypass graft surgery, but were less likely to have a reduced creatinine clearance (Table 1). Patients treated with a CCB were more likely to be older, female, and have additional risk factors including hypertension, hyperlipidemia, diabetes, prior MI, family history of CAD, cerebrovascular disease, peripheral arterial disease, and congestive heart failure. Statins and clinical outcomes. For patients randomized to clopidogrel, the Kaplan-Meier rate of the primary endpoint through long-term follow-up was similar for patients who were (11.9%) or were not (12.4%) on a CYP3A4-metabolized statin (unadjusted hazard ratio [HR]: 0.94; 95% confidence interval [CI]: 0.81 to 1.10; p ¼ 0.43) (Fig. 1). After multivariable adjustment including the propensity to be treated with a statin, there remained no significant association between statin use and the risk of CV death, MI, or stroke for patients on clopidogrel (adjusted HR: 1.02; 95% CI: 0.85 to 1.22; p ¼ 0.83) (Table 2). Similarly, statin use was also not associated with an increased risk of CV death or MI (adjusted HR: 1.02; 95% CI: 0.85 to 1.23; p ¼ 0.84) (Table 2). Because patients could start or stop a statin during the course of follow-up, we examined those clopidogrel-treated patients who were recorded to be consistently taking a CYP3A4-metabolized statin both at randomization and at the end of the study (n ¼ 3,841, 56.5%). The consistent use of statins was not associated with an increased risk of CV death, MI, or stroke (adjusted HR: 0.96; 95% CI: 0.74 to 1.25; p ¼ 0.78) or CV death or MI (adjusted HR: 0.95; 95% 1278 Ojeifo et al. Clopidogrel and Drug Interactions Figure 1. Risk of CV Events for Clopidogrel-Treated Patients With or Without a Statin Unadjusted Kaplan-Meier curves for risk of cardiovascular (CV) death, myocardial infarction (MI), or stroke for clopidogrel-treated patients who were (blue line) or were not (red line) on a CYP3A4-metabolized statin at randomization. The risk of CV events was similar for clopidogrel-treated patients regardless of background use of a statin. CI: 0.72 to 1.24; p ¼ 0.70), as compared with those patients not consistently on a statin. As a sensitivity analysis, we examined the association between the use of atorvastatin and the risk of CV events for patients on clopidogrel, because some studies have only shown a pharmacodynamic interaction with clopidogrel for this particular statin type. When atorvastatin was examined individually, its use was also not associated with an increased risk of CV death or MI (HR: 1.07; 95% CI: 0.92 to 1.25; p ¼ 0.39) or stent thrombosis (HR: 0.99; 95% CI: 0.69 to 1.40; p ¼ 0.93) in clopidogrel-treated patients. The efficacy of prasugrel versus clopidogrel was similar for patients who were (HR: 0.79; 95% CI: 0.70 to 0.90) or were not (HR: 0.86; 95% CI: 0.72 to 1.04) on a statin (p for interaction ¼ 0.43) (Fig. 2). Prasugrel significantly reduced the risk of stent thrombosis by 48% to 60% for patients who were (HR: 0.52; 95% CI: 0.37 to 0.74) or were not (HR: 0.40; 95% CI: 0.24 to 0.66) on a statin (p for interaction ¼ 0.39). CCBs and clinical outcomes. Before multivariable adjustment, patients on a CCB had a higher risk of CV death, MI, or stroke through long-term follow-up, regardless of whether they were on clopidogrel or prasugrel. For patients randomized to clopidogrel, the rate of the primary endpoint throughout long-term follow-up was 15.7% for patients on a CCB versus 11.5% for those not a CCB (unadjusted HR: 1.38; 95% CI: 1.15 to 1.65; p ¼ 0.001). However, after adjusting for baseline differences and the propensity to treat with a CCB, use of a CCB was no longer associated with an increased risk of CV death, MI, or stroke in clopidogrel-treated patients (adjusted JACC: CARDIOVASCULAR INTERVENTIONS, VOL. 6, NO. 12, 2013 DECEMBER 2013:1275–81 HR: 1.16; 95% CI: 0.94 to 1.43; p ¼ 0.18) or CV death or MI (adjusted HR: 1.17; 95% CI: 0.93 to 1.45; p ¼ 0.17) (Table 2). For those clopidogrel-treated patients who were recorded to be taking a CCB both at the start and end of the study (n ¼ 582, 10.5%), the consistent use of CCBs was not associated with an increased risk of CV death, MI, or stroke (adjusted HR: 1.06; 95% CI: 0.80 to 1.40; p ¼ 0.71) or CV death or MI (adjusted HR: 1.02; 95% CI: 0.77 to 1.37; p ¼ 0.87). Patients on a CCB had a comparable reduction in CV death, MI, or stroke with prasugrel versus clopidogrel (HR: 0.87; 95% CI: 0.68 to 1.10), as compared with those patients not on a CCB (HR: 0.80; 95% CI: 0.71 to 0.90, p for interaction ¼ 0.55) (Fig. 2). Prasugrel also significantly reduced the risk of stent thrombosis for patients who were (HR: 0.30; 95% CI: 0.16 to 0.58) or were not (HR: 0.53; 95% CI: 0.39 to 0.74) on a CCB (p for interaction ¼ 0.13). Concomitant use of multiple CYP450-metabolized medications. In the event that a clinical threshold effect may exist for the pharmacodynamic effects of clopidogrel, we examined CV risk in those patients who were treated simultaneously with 2 or more medications that have been hypothesized to interfere with the conversion of clopidogrel to its active metabolite. In clopidogrel-treated patients, 694 individuals were simultaneously on a CYP3A4-metabolized statin and a CCB at randomization. Within this group of patients on 2 CYP3A4metabolized medications, there remained no significant association between combined drug use and the risk of CV death, MI, or stroke (adjusted HR: 1.19; 95% CI: 0.93 to 1.51), as compared with those patients not on either a statin or CCB. Similarly, there was not an increased risk of CV death, MI, or stroke for those patients simultaneously on atorvastatin 80 mg daily and a CCB (adjusted HR: 0.82; 95% CI: 0.37 to 1.84). Only 236 clopidogrel-treated subjects were on a combination of a CCB, statin, and a proton pump inhibitor at randomization. Within this group of subjects, the concomitant use of 3 drugs that could interfere with the hepatic metabolism of clopidogrel was not associated with an increased risk of CV death, MI, or stroke (adjusted HR: 1.04; 95% CI: 0.70 to 1.54) when compared with patients on none of these medications. Discussion In a large population of patients with ACS, we found that the use of statins, CCBs, or a combination of both these medications did not appear to interfere with the clinical efficacy of clopidogrel. These findings are clinically relevant in light of prior pharmacodynamic studies that have shown conflicting results as to whether statins or CCBs may attenuate the acute antiplatelet effects of clopidogrel (1–6). Therefore, Ojeifo et al. Clopidogrel and Drug Interactions JACC: CARDIOVASCULAR INTERVENTIONS, VOL. 6, NO. 12, 2013 DECEMBER 2013:1275–81 1279 Table 2. Kaplan-Meier Event Rates Through Long-Term Follow-Up Stratified by the Use of a Statin or CCB at Randomization for Patients Treated With Clopidogrel Statin CCB Treated Not Treated Adjusted HR (95% CI) Treated vs. Nontreated* Treated Not Treated Adjusted HR (95% CI) Treated vs. Nontreated CV death, MI, or stroke 11.9% (542/4,794) 12.4% (239/2,001) 1.02 (0.85–1.22) 15.7% (142/966) 11.5% (639/5,829) 1.16 (0.94–1.43) CV death or MI 11.0% (503/4,794) 11.7% (225/2,001) 1.02 (0.85–1.23) 14.4% (131/966) 10.7% (597/5,829) 1.17 (0.93–1.45) Values are % (n/N). Adjusted hazard ratios (HRs) (95% confidence intervals [CI]) reflect the association between subjects treated with a CYP3A4-metabolized statin or calcium-channel blocker (CCB) use (as compared with those subjects not treated with a CYP3A4-metabolized statin or CCB) and the risk of clinical outcomes after adjusting for potential confounders and the propensity to treat with the drug. CV ¼ cardiovascular; MI ¼ myocardial infarction. this information provides important reassurance to clinicians that these classes of drugs can be safely combined. Both clopidogrel and prasugrel are pro-drugs that require biotransformation via the CYP enzyme system to form their active metabolites. Before undergoing hepatic metabolism, 85% of the clopidogrel pro-drug is converted to inactive esterases and therefore unable to undergo hepatic metabolism. By contrast, the metabolism of prasugrel appears to be more efficient because it involves a single CYP-dependent step, and the pro-drug is not shunted down a dead-end pathway (10). Although several CYP enzymes contribute to the 2-step metabolism of clopidogrel, it has been suggested that the greatest contribution is from the CYP3A4, CYP3A5, and CYP2C19 isoenzymes (11). Supporting the concept that CYP3A4 plays a key role in the conversion of clopidogrel to its active metabolite, CYP3A4 enzyme activity has been shown to be inversely correlated to the pharmacodynamic response to clopidogrel (12). Although the relative contribution of different CYP450 isoenzymes to the metabolism of clopidogrel remains unclear, 1 in vitro study using human microsomes containing CYP3A4 and CYP3A5 suggested that these 2 isoenzymes are primarily responsible for the conversion of clopidogrel to its active metabolite (13). A second study demonstrated that the CYP2C19 isoenzyme contributes substantially to both bio-oxidative steps, whereas CYP3A4 is integral to the second bio-oxidative step (11). Lipophilic statins, including atorvastatin, simvastatin, and lovastatin, are metabolized by CYP3A4 and therefore compete with clopidogrel for its substrate. In ex vivo experiments, when clopidogrel and atorvastatin were exposed in equimolar amounts to human microsomes containing CYP3A4, clopidogrel metabolism was inhibited by >90% (13). Further, studies have shown that atorvastatin may attenuate the antiplatelet effects of clopidogrel (1,2). These results were subsequently validated by a prospective randomized trial that showed an interaction between atorvastatin and a 300-mg (but not a 600-mg) loading dose of clopidogrel as assessed by lighttransmission aggregometry (3). By contrast, several studies have since been unable to demonstrate a definitive interaction between these classes of drugs (7). These discrepancies might in part be explained by marked differences in study designs, population size, clopidogrel dosing, platelet function testing methodology, and concomitant medications (7). To date, the clinical relevance of these findings has been evaluated in several observational studies that have failed to demonstrate that CYP3A4-metabolized statins interfere with the clinical efficacy of clopidogrel (14–19). Because of their common requirement for CYP3A4 metabolism, there exists similar concern that CCBs might Figure 2. Efficacy of Prasugrel Versus Clopidogrel for Patients on a Statin or CCB The relative efficacy of prasugrel versus clopidogrel for patients on a background of CYP3A4-metabolized statins or calcium-channel blockers (CCBs). Hazard ratios (HRs) (95% confidence interval [CI]) reflect the relative risk of CV death, MI, or stroke for patients treated with prasugrel as compared with those patients treated with clopidogrel. Abbreviations as in Figure 1. 1280 Ojeifo et al. Clopidogrel and Drug Interactions interact with clopidogrel. This concern is supported by several studies that have shown that CCBs attenuate the antiplatelet effects of clopidogrel (4–6). However, as with statins, some studies have failed to observe a pharmacodynamic interaction between these classes of drugs (20,21). To date, there exist limited data to determine whether use of a CCB increases CV risk in clopidogrel-treated patients. In a Danish registry of patients after MI, patients on a CCB were observed to have an increased risk of CV events regardless of whether or not they were treated with clopidogrel, thereby suggesting the increase in risk was likely explained by unidentified confounders (22). More recently, there was no evidence of an interaction between clopidogrel and CCB use in a post hoc analysis of 2,116 subjects in a randomized trial of 2 dosage regimens of clopidogrel postPCI (23) or in 1,608 subjects after placement of a drugeluting stent (21). In the current analysis of 13,608 subjects with ACS, we did not find that CYP3A4-metabolized statins, CCBs, or concomitant use of both medications attenuated the clinical efficacy of clopidogrel. Moreover, the combination of a proton pump inhibitor with 2 CYP3A4-metabolized drugs also did not demonstrate an increased risk of CV events. These data represent one of the largest study populations to address the question of a possible drug–drug interaction between these classes of drugs. Because the study population was drawn from a clinical trial database, we were able to carefully adjust for baseline differences and the propensity to treat with either a statin or CCB. Although patients on a CCB were found to be at increased risk of CV events, this excess in CV risk did not persist after multivariable adjustment in clopidogrel-treated patients; thereby highlighting that CCB use was associated with a higher-risk patient population rather than interfering with the efficacy of clopidogrel. Further, the relative efficacy of prasugrel versus clopidogrel was similar regardless of background use of statins or CCBs, again suggesting that the clinical efficacy of clopidogrel was not attenuated in patients prescribed CYP3A4-metabolized drugs. Therefore, despite the previously reported in vitro interaction that was observed in some studies between clopidogrel and CYP3A4-metabolized statins or CCBs, we did not observe concomitant use of these classes of drugs to be associated with an increased risk of CV events. These findings highlight that there is still more to learn regarding the relationship between platelet reactivity and clinical outcomes. Further, an ex vivo measure of platelet function may not reliably reflect the in vivo complexity of thrombosis, inflammation, and endothelial function. Although a pharmacodynamic interaction has been reported for some types of proton pump inhibitors when combined with clopidogrel (7), several outcome studies, including an analysis from the TRITON–TIMI 38 trial, did not confirm an increase in CV events when these drug classes are combined (24,25). If JACC: CARDIOVASCULAR INTERVENTIONS, VOL. 6, NO. 12, 2013 DECEMBER 2013:1275–81 a pharmacodynamic interaction indeed exists between clopidogrel and CCBs or statins, it is plausible that this interaction is too weak to translate into CV harm (26). However, we still observed no signal toward increased risk when multiple drugs that interfere with the CYP450 enzyme system were combined. Study limitations. Limitations to the current analysis include the fact that use of statins and CCBs were not randomized, thereby increasing the risk of confounding by indication or by other unassessed variables, and therefore, causality cannot be definitively determined. However, we performed extensive multivariable adjustment for baseline differences and included a propensity score to be treated with a statin or CCB in our models. The use of concomitant medications was captured at randomization and may have changed because statins and CCBs could have been started or stopped during the course of the trial. Because DNA samples were only available in a subset of the TRITON–TIMI 38 population, our study was insufficiently powered to determine whether an interaction might exist between CYP3A4metabolized medications and carriers of a reduced-function CYP2C19 allele. Although loss-of-function variants in the CYP3A4 gene exist, they are rare. Conclusions Overall, in patients with an ACS undergoing PCI, the clinical efficacy of clopidogrel did not appear to be significantly modified by concomitant CCB and/or statin use. Further, the use of statins and CCBs did not influence the relative efficacy or safety of prasugrel as compared with clopidogrel. Although only a randomized trial can definitively establish the clinical implications of combining statins or CCBs with clopidogrel, the results of this study do not support the need to avoid concomitant use of statins or CCBs in patients receiving clopidogrel. Reprint requests and correspondence: Dr. Michelle L. O’Donoghue, Cardiovascular Division, Brigham and Women’s Hospital, TIMI Study Group, 350 Longwood Avenue, 1st Floor, Boston, Massachusetts 02115. E-mail: [email protected]. REFERENCES 1. Lau WC, Waskell LA, Watkins PB, et al. Atorvastatin reduces the ability of clopidogrel to inhibit platelet aggregation: a new drug-drug interaction. Circulation 2003;107:32–7. 2. Neubauer H, Gunesdogan B, Hanefeld C, Spiecker M, Mugge A. Lipophilic statins interfere with the inhibitory effects of clopidogrel on platelet functionda flow cytometry study. Eur Heart J 2003;24:1744–9. 3. Lau WC, Neer CJ, Tait AR, Carville DG, Guyer KE, Bates ER. Higher doses of clopidogrel overcome the atorvastatin-clopidogrel drugdrug interaction (abstr). Circulation 2005;112:II295. 4. Siller-Matula JM, Lang I, Christ G, Jilma B. Calcium-channel blockers reduce the antiplatelet effect of clopidogrel. J Am Coll Cardiol 2008;52: 1557–63. Ojeifo et al. Clopidogrel and Drug Interactions JACC: CARDIOVASCULAR INTERVENTIONS, VOL. 6, NO. 12, 2013 DECEMBER 2013:1275–81 5. Gremmel T, Steiner S, Seidinger D, Koppensteiner R, Panzer S, Kopp CW. Calcium-channel blockers decrease clopidogrel-mediated platelet inhibition. Heart 2010;96:186–9. 6. Harmsze AM, Robijns K, van Werkum JW, et al. The use of amlodipine, but not of P-glycoprotein inhibiting calcium channel blockers is associated with clopidogrel poor-response. Thromb Haemost 2010;103: 920–5. 7. Bates ER, Lau WC, Angiolillo DJ. Clopidogrel-drug interactions. J Am Coll Cardiol 2011;57:1251–63. 8. Wiviott SD, Braunwald E, McCabe CH, et al. Prasugrel versus clopidogrel in patients with acute coronary syndromes. N Engl J Med 2007;357:2001–15. 9. Cutlip DE, Windecker S, Mehran R, et al. Clinical end points in coronary stent trials: a case for standardized definitions. Circulation 2007;115:2344–51. 10. Mega JL, Close SL, Wiviott SD, et al. Cytochrome P450 genetic polymorphisms and the response to prasugrel: relationship to pharmacokinetic, pharmacodynamic, and clinical outcomes. Circulation 2009; 119:2553–60. 11. Kazui M, Nishiya Y, Ishizuka T, et al. Identification of the human cytochrome P450 enzymes involved in the two oxidative steps in the bioactivation of clopidogrel to its pharmacologically active metabolite. Drug Metab Dispos 2010;38:92–9. 12. Lau WC, Gurbel PA, Watkins PB, et al. Contribution of hepatic cytochrome P450 3A4 metabolic activity to the phenomenon of clopidogrel resistance. Circulation 2004;109:166–71. 13. Clarke TA, Waskell LA. The metabolism of clopidogrel is catalyzed by human cytochrome P450 3A and is inhibited by atorvastatin. Drug Metab Dispos 2003;31:53–9. 14. Saw J, Steinhubl SR, Berger PB, et al. Lack of adverse clopidogrelatorvastatin clinical interaction from secondary analysis of a randomized, placebo-controlled clopidogrel trial. Circulation 2003;108:921–4. 15. Wienbergen H, Gitt AK, Schiele R, et al. Comparison of clinical benefits of clopidogrel therapy in patients with acute coronary syndromes taking atorvastatin versus other statin therapies. Am J Cardiol 2003;92:285–8. 16. Lim MJ, Spencer FA, Gore JM, et al. Impact of combined pharmacologic treatment with clopidogrel and a statin on outcomes of patients with non-ST-segment elevation acute coronary syndromes: perspectives from a large multinational registry. Eur Heart J 2005;26: 1063–9. 17. Mukherjee D, Kline-Rogers E, Fang J, Munir K, Eagle KA. Lack of clopidogrel-CYP3A4 statin interaction in patients with acute coronary syndrome. Heart 2005;91:23–6. 18. Brophy JM, Babapulle MN, Costa V, Rinfret S. A pharmacoepidemiology study of the interaction between atorvastatin and 1281 clopidogrel after percutaneous coronary intervention. Am Heart J 2006; 152:263–9. 19. Saw J, Brennan DM, Steinhubl SR, et al. Lack of evidence of a clopidogrel-statin interaction in the CHARISMA trial. J Am Coll Cardiol 2007;50:291–5. 20. Price MJ, Nayak KR, Barker CM, Kandzari DE, Teirstein PS. Predictors of heightened platelet reactivity despite dual-antiplatelet therapy in patients undergoing percutaneous coronary intervention. Am J Cardiol 2009;103:1339–43. 21. Sarafoff N, Neumann L, Morath T, et al. Lack of impact of calciumchannel blockers on the pharmacodynamic effect and the clinical efficacy of clopidogrel after drug-eluting stenting. Am Heart J 2011;161: 605–10. 22. Olesen JB, Gislason GH, Charlot MG, et al. Calcium-channel blockers do not alter the clinical efficacy of clopidogrel after myocardial infarction: a nationwide cohort study. J Am Coll Cardiol 2011;57: 409–17. 23. Good CW, Steinhubl SR, Brennan DM, Lincoff AM, Topol EJ, Berger PB. Is there a clinically significant interaction between calcium channel antagonists and clopidogrel?: results from the Clopidogrel for the Reduction of Events During Observation (CREDO) trial. Circ Cardiovasc Interv 2012;5:77–81. 24. O’Donoghue ML, Braunwald E, Antman EM, et al. Pharmacodynamic effect and clinical efficacy of clopidogrel and prasugrel with or without a proton-pump inhibitor: an analysis of two randomised trials. Lancet 2009;374:989–97. 25. Bhatt DL, Cryer BL, Contant CF, et al. Clopidogrel with or without omeprazole in coronary artery disease. N Engl J Med 2010;363: 1909–17. 26. O’Donoghue ML. CYP2C19 genotype and proton pump inhibitors in clopidogrel-treated patients: does it take two to tango? Circulation 2011;123:468–70. Key Words: clopidogrel - clopidogrel response variability - drug–drug interactions - drug metabolism prasugrel. APPENDIX For supplementary tables and expanded Methods section, please see the online version of this paper.