Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
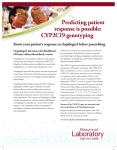
CARE OF NSTEMI PATIENTS LATEST GUIDELINES Rick Barney MD FACEP Emergency Medicine Beloit Memorial and University of Wisconsin New NSTEMI Guidelines by ACC/AHA Released August 6th 2007 www.americanheart.org NSTEMI Protocols not followed well STEMI- straight forward and well followed NSTEMI- no hospital agreement, under use of available treatment, no agreement even amongst cardiologists Following ACC/AHA Guidelines Significantly Reduces Risk of Mortality Incidence of in-hospital mortality was lower with adherence to ACC/AHA Guidelines Nonadherence to ACC/AHA Guidelines 3.7% (n = 9,889) 32.4%↓ (P < 0.001) Adherence to ACC/AHA Guidelines Bhatt DL, et al. JAMA. 2004;292(17):2096-2104. 2.5% (n = 8,037) NSTEMI- Definition Coronary symptoms with ST segment depression, or T wave inversions (new) and/or elevated biomarkers (Troponin preferred) Nitro Recommendation If new angina pattern, call 911 if one single nitro has not helped. Take 2nd and 3rd dose while waiting for EMS arrival If typical stable angina pattern, still recommend call for help if three nitro doses 5 minutes apart does not help. Aspirin and Pre-Hospital 12 lead ECG Aspirin should be given immediately to all patients who may have a coronary Syndrome. Only reason to not give is a true allergy. Strong recommendation for pre-hospital 12 lead analysis Positive Biomarkers are critical to ED Care Latest studies show patients with positive Troponins do best with early invasive management, Clopidogrel, anticoagulation, and glycoprotien II b III a inhibition. USE OF BETA BLOCKERS COMMIT Trial shows some risk in using IV Metoprolol. For NSTEMI-use IV if hyperdynamic, otherwise PO within 24 hours of arrival Morphine results in higher mortality for NSTEMI patients Due to blocking pain, yet ischemia still present Due to hypotension Due to decreased myocardial perfusion Many now use Fentanyl instead Early Invasive Management Improves Outcomes NSTEMI- thus high risk patients in general do better if treated aggressively in ED, then to cath lab in 4-24 hours. 18% death or MI reduction. Even studies on stabilization and later treatment are predicated on aggressive ED treatment In general, this includes Clopidogrel, anticoagulant, and Glycoprotein II B III A Inhibition 2007 Anti-platelet Guidelines Nothing new on Aspirin- continue to use Recommend Clopidogrel or II B III A OR Use both Clopidogrel and II B III A Using both makes more scientific sense as drugs work differently. Some patients are partial or non-responders to Clopidogrel. Anti-Platelet Therapy Clopidogrel is irreversible. Will delay CABG 3-5 days. Integrelin is reversible once infusion is shut off. Anti-platelet therapy is critical to success and is under- utilized Coordinated, standard approach at your institution is desirable. ISAR-REACT 2 study shows adding Glycoprotein IIBIIIA The Central Role of the Platelet in NSTE ACS Sites of Antithrombotic Drug Action Coagulation cascade Platelet cascade Intrinsic Pathway Platelet Activation Plasma clotting cascade LMWH Prothrombin Clopidogrel Activation of GP IIb-IIIa Other agonists ADP Factor Xa UFH AT III* Bivalirudin Agonist degranulation TxA2 ASA Platelet recruitment and aggregation Thrombin Fibrinogen cross links to form platelet-rich thrombus GP IIb-IIIa inhibitors Thrombolytics Fibrin Mesh Formation of mature thrombus *AT III = antithrombin III. Stein B, et al. J Am Coll Cardiol. 1989;14(4):813-836; DeJong MJ, et al. Crit Care Nurs Clin N Am. 1999;11(3):355371; White HD. Am J Cardiol. 1997;80(4A):2B-10B. The Role of the Platelet in Non-ST-segment Elevation Acute Coronary Syndrome (NSTE ACS) NSTE ACS is generally caused by partially occlusive, platelet-rich thrombus in a coronary artery Results from cross-linking of platelets by fibrinogen at platelet receptors GP IIb-IIIa at site of plaque rupture Unobstructed lumen GP IIb-IIIa Platelet Thrombus Fibrinogen Ruptured plaque Artery wall Van de Werf F. Thromb Haemost. 1997;78(1):210-213; Moser M, et al. J Cardiovasc Pharmacol. 2003;41(4): 586-592; Reprinted with permission from Davies MJ. Heart. 2000;83(3):361-366. © BMJ Publishing Group Ltd. 2005. The Thrombus in STEMI STEMI is generally caused by a completely occlusive fibrin-rich thrombus in a coronary artery Results from stabilization by fibrin mesh of a platelet aggregate at site of plaque rupture platelet RBC* fibrin mesh *RBC = red blood cell. GP IIb-IIIa inhibitors are not indicated for STEMI. Van de Werf F. Thromb Haemost. 1997;78(1):210-213; White HD. Am J Cardiol. 1997;80(4A):2B-10B; Davies MJ. Heart. 2000;83(3):361-366. Microembolization in Unstable Angina Courtesy of C. Michael Gibson, MS, MD, Director TIMI Data Coordinating Center, Brigham & Women’s Hospital, Associate Chief of Cardiology, Interventional Cardiologist, Beth Israel Deaconess Medical Center, Harvard Medical School. Variable Clopidogrel Response Response measured after elective coronary artery stent implantation At 5 Days UA Patients* (n = 32) At 4 Hours Healthy Volunteers† (n = 25) Nonresponders 16% Nonresponders 22% Responders 47% Responders 72% Low responders 12% Low responders 32% *Received an oral loading dose of 300 mg of clopidogrel followed by 75 mg daily; †Received a 450-mg loading dose of clopidogrel. The use of clopidogrel in this study was not consistent with applicable FDA-approved Prescribing Information. Gurbel PA, et al. Circulation. 2003;107(23):2908-2913; Lau WC, et al. Circulation. 2004;109(2):166-171. GP IIb-IIIa Inhibitors Are an ACC/AHA Guidelines IA Recommendation AT PRESENTAION HIGH-RISK FEATURES Signs of ischemia at rest > 20 minutes AND ST-segment depression and/or elevated cardiac biomarkers RECOMMENDED TREATMENT REGIMEN Aspirin (IA); clopidogrel if aspirin is contraindicated (IA) LMWH or UFH (IA) GP IIb-IIIa inhibitor (IA) Beta blocker (IB) Nitrates (IC) SEND FOR CATHETERIZATION & REVASCULARIZATION WITHIN 24-48 HOURS PCI or CABG SURGERY IF CORONARY ANATOMY IS SUITABLE (IA) CAUTIONARY INFORMATION No clopidogrel within 5-7 days prior to CABG surgery No enoxaparin within 24 hours prior to CABG surgery No abciximab, if PCI is not planned LEVELS OF EVIDENCE I. Evidence and/or agreement that treatment is effective IIa. Weight of evidence favors use IIb. Usefulness less well established III. Evidence and/or agreement that treatment is not effective Braunwald E, et al. J Am Coll Cardiol. 2002;40(7):1366-1374. LEVELS OF EVIDENCE RANK A. Based on large, randomized trials B. Based on smaller trials or careful analyses C. Based on expert consensus Changes in Cardiac Arrest Management Pharmacology No improvements evident based on science with drugs to improve outcome Epinephrine every 5 minutes No added benefit to Vasopressin Amiodarone and Lidocaine equal effectiveness Defibrillation Primary treatment for V-fib at 3 minutes and under Should be delayed until good CPR for 2 minutes if down time over 3 minutes Biphasic should be used AED’s good in 3 minutes, bad after One shock only with no pulse checks after Vascular Access Avoid ET drugs whenever possible Peripheral IV’s OK Central IV’s slightly better, but compression interruption frequent with placement Interosseous recommended when peripheral IV’s not obtainable Pathophysiology of V-Fib Arrest How Compressions move blood What about AED’s? Great in first 3 minutes. Must be in community. Deadly after this as delay to shock is over 30 seconds. Manual defib required after 3 minutes. Defibrillation No more stacked shocks Takes too long All shocks maximum energy. EMS probably should not use AED’s Biphasic increases efficacy Pulse Checks Deadly!! Only check pulses when rhythm appears to have converted thru CPR on ECG or signs of life ECC says check before shock delivered after 5 cycles of 30:2 CPR What about intubation? In first 6 minutes, not a priority (V-fib) ASAP in PEA and Asystole. Understand that positive pressure breaths decrease cardiac output. Some air exchange from CPR plus gasping. Once intubated, 1 second breaths,six per minute. NO MORE. Airway Combitube or ET equivalent RSA Mentality-view and see cords place ET, otherwise immediate Combitube first try. Protocol Dispatch instructs CCC If good CPR on EMS arrival, shock max X1 If no or poor CPR, immediate compressions Protocol OP airway Non-rebreather face mask @ 90+% 200 compressions IV access Epinephrine 1mg IVP Vasopressin 40 units IVP ASAP One shock, 3-5 seconds, no pulse checks. Protocol Begin second round of 200 compressions Amiodarone 300mg IVP Shock X1 at max joules No pulse checks, not off chest more than 5 seconds. Protocol Begin 3rd round of compressions Epinephrine 1mg IVP Shock X1 after 200 compressions Protocol During 4th round of compressions place definitive airway without halting compressions on first attempt. Protocol 200 compressions alternating epinephrine with antidysrhythmic drug and shock X1. Remain on scene and work until pulse or nonshockable rhythm. 48% Neuro-intact survivors!! 10% before new protocol QUESTIONS??