Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
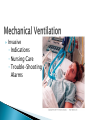
Respiratory System Function, Assessment, and Therapeutic Measures Upper Respiratory Symptoms Lower Respiratory Symptoms Exposures/Smoking Current Treatments Family History Where Is It? How Does It Feel? Aggravating and Alleviating Factors Timing Severity Useful Other Data Patient’s Perception Symmetry Dyspnea Use of Accessory Muscles Color Respiratory Rate and Rhythm Chest Shape Normal Breath Sounds Adventitious Sounds Compare Bilaterally Crackles—Coarse or Fine Wheezes Stridor Friction Rub Diminished Absent CBC ABGs D-Dimer C&S SaO2 Chest X-Ray VQ Scan PFTs Angiography Bronchoscopy Smoking Cessation ◦ ◦ ◦ ◦ ◦ Ask Advise Assess Assist Arrange Interventions ◦ Behavior Modification ◦ Counseling ◦ Setting Quit Date ◦ Nicotine Replacement ◦ Drug Therapy ◦ Hypnosis Deep Breathing and Coughing Breathing Exercises Positioning ◦ Fowler’s ◦ Semi-Fowler’s ◦ Good Lung Down Nasal Cannula A. C. B. D. Indications Chest Tube Insertion Drainage System Nursing Care Definition Indications Nursing Care ◦ ◦ ◦ ◦ Suctioning Cleaning Communication Teaching Invasive ◦ Indications ◦ Nursing Care ◦ Trouble-Shooting Alarms Nursing Care of Patients with Upper Respiratory Disorders Causes ◦ Trauma ◦ Hypertension ◦ Hemophilia ◦ Medications ◦ Recreational Drug Use (Cocaine) Positioning Direct Pressure Ice Nasal Packing Nasal Balloon Catheter Vasoconstrictive Agent Electrocautery Usually Benign Occur More Often with Allergies Treatment ◦ Control Allergies ◦ Surgery ◦ Avoid Aspirin Postop Symptoms ◦ Stuffy Nose ◦ Blocked Sinus Drainage ◦ Headaches Treatment ◦ Nasoseptoplasty Monitor Vital Signs/Bleeding Report Excess Swallowing Monitor Dressing Teach ◦ Avoid Activities That Increase Pressure ◦ Avoid Aspirin Inflammation ◦ Bacterial ◦ Allergic Signs of Sinus Mucosa and Symptoms ◦ Pain Over Affected Sinus ◦ Fever ◦ Nasal Discharge Decongestants Hot Packs Saline Irrigation Acetaminophen/ Ibuprofen Humidification Oral Fluids Positioning Antibiotics Surgical Drainage Rest Rhinitis Pharyngitis Laryngitis Tonsillitis Pathophysiology ◦ Primary Tumor of Mucosal Epithelium ◦ Metastasizes to Lungs, Liver, Lymph Nodes Etiology ◦ Associated with Smoking, Alcohol ◦ More Common in Men Hoarseness Change in Voice Pain Dyspnea Cough Dysphagia Airway Obstruction Laryngoscopy CT MRI Radiation Chemotherapy Laryngectomy Ineffective Airway Clearance Acute Pain Impaired Verbal Communication Imbalanced Nutrition Impaired Swallowing Grieving Disturbed Body Image Nursing Care of Patients with Lower Respiratory Tract Disorders Pathophysiology ◦ ◦ ◦ ◦ Acute Lung Infection Inflammation and Alveolar Damage Alveoli Filled with Exudate Reduced Surface Area for Gas Exchange Bacteria, Uusually Steptococcus pneumoniae Virus Fungus Aspiration Artificial Ventilation (VAP) Hypostasis Chemical Very Young Elderly Hospitalized Intubated Immunocompromised Chest Pain Fever, Chills Cough, Dyspnea Yellow, Rusty, or Blood-Tinged Sputum Crackles, Wheezes Malaise Pleurisy Pleural Effusion Atelectasis Spread of Infection Chest X-Ray Sputum Culture Blood Cultures Antibiotics - PO or IV Antiviral Medication (Zovirax) Bronchodilators Expectorants Oxygen Fluids Pathophysiology ◦ ◦ ◦ ◦ ◦ AFB Implant on Bronchioles or Alveoli Tubercle Formed Immune System Keeps in Check 5%-10% Infected Become Ill May Activate with Impaired Immunity Elderly Alcoholics Crowded Living Conditions New Immigrants HIV Cough Blood-Tinged Sputum Night Sweats Anorexia and Weight Loss Low-Grade Fever Dyspnea, Chest Pain (Late) PPD Skin Test Chest X-Ray Sputum Cultures QuatifFERON-TB Gold Combination of Drugs for 6 - 24 Months ◦ ◦ ◦ ◦ INH Rifampin Streptomycin Ethambutol Occasional Surgical Removal Isolation Impaired Gas Exchange Ineffective Airway Clearance Ineffective Breathing Pattern Activity Intolerance Monitor ◦ Lung Sounds, Respiratory Rate and Effort ◦ Dsypnea ◦ Mental Status ◦ SaO2, ABGs Position ◦ Fowler’s ◦ Good Lung Down Administer Oxygen Teach Breathing Exercises Discourage Smoking Monitor ◦ Lung Sounds ◦ Sputum Encourage ◦ Fluids ◦ Deep Breathing ◦ Coughing Administer Expectorants Turn q2h or Ambulate Suction prn Consider CPT or Mucus Clearance Device Monitor ◦ Respiratory Rate, Depth, Effort ◦ ABGs, SaO2 Determine/Treat Cause Position Teach Diaphragmatic Breathing Monitor Response to Activity ◦ Vital Signs ◦ SaO2 Use Portable O2 for Ambulation Allow Rest Between Activities Obtain Bedside Commode Increase Activity Slowly Refer to Pulmonary Rehabilitation Clean, Well-Ventilated Living Areas Isolation of Patients who have Active TB High-Efficiency Filtration Masks Gowns, Gloves, Goggles If Contact with Sputum Likely Combination of ◦ Chronic Bronchitis ◦ Emphysema ◦ Asthma Chronic Airflow Limitation Chronic Bronchitis Chronic Inflammation Low-Grade Infection Hypertrophied Mucous Glands in Bronchi Impaired Ciliary Function Ineffective Airway Clearance Destruction of Alveolar Walls Loss of Elastic Recoil Damage to Pulmonary Capillaries Air Trapping Impaired Gas Exchange Diagnosed After Ill 3 Months of Year for 2 Consecutive Years Emphysema Smoking Passive Smoke Exposure Pollutants Familial Predisposition α1AT Deficiency (Emphysema) Smoking!! Cough Sputum Production Dyspnea Prolonged Expiration Barrel Chest Activity Intolerance Wheezing, Crackles Chronic Cough Dyspnea Thick, Tenacious Sputum Increased Susceptibility to Infection Mucous Plugs Diminished Breath Sounds Dyspnea Progressive Activity Intolerance Cor Pulmonale Weight Loss Pneumothorax Respiratory Failure Chest X-Ray CT Scan ABGs CBC Spirometry Sputum Analysis Stop Smoking!! Oxygen 1-2 L/m Supportive Care Pulmonary Rehab Surgery Mechanical Ventilation End-of-Life Planning Medications ◦ Bronchodilators ◦ Corticosteroids ◦ Expectorants NMT/MDI Pathophysiology ◦ ◦ ◦ ◦ Inflammation of Bronchial Mucosa/ Bronchial Tree Spasm of Bronchial Smooth Muscles Air Trapping Reversible Smoking Allergens Infection Sinusitis Stress GERD Dyspnea Wheezing Cough Sputum Use of Accessory Muscles May Be Worse at Night Status Asthmaticus ◦ Severe, Sustained Asthma ◦ Worsening Hypoxemia ◦ Respiratory Alkalosis Progresses to Respiratory Acidosis ◦ May Be Life Threatening History and Physical Examination Spirometry ABGs Allergy Skin Testing Bronchodilators Adrenergic (Ventolin, Serevent) Leukotriene Inhibitors (Accolate, Singulair) Theophylline (Rare) Corticosteroids Inhaled, IV, PO Mast Cell Inhibitors (Exercise Induced) Antihistamines Oxygen PRN Pathophysiology ◦ Exocrine Gland Disorder ◦ Thick Tenacious Secretions ◦ Blocked Pancreatic Enzymes Etiology ◦ Heredity Thick Tenacious Sputum Frequent Respiratory Infections Finger Clubbing Malabsorption Fatty, Foul Smelling Stools Death From Antibiotic-resistant Infection Hydration Inhaled Mucolytic Medication Bronchodilators, Corticosteroids Expectorants Chest Physiotherapy Antibiotics Prevent Infection Pancreatic Enzyme Replacement (Pancrease, Viokase) Ibuprofen May Slow Lung Deterioration Lung Transplant Pathophysiology ◦ ◦ ◦ ◦ Blood Clot in Pulmonary Artery Ventilation-Perfusion Mismatch Impaired Gas Exchange Lung Infarction DVT Most Common Fat Emboli From Compound Fracture Amniotic Fluid Emboli During L&D Regular Ambulation Prompt Treatment of DVT In High-risk Patients ◦ Warfarin (Coumadin) ◦ Heparin Sudden Onset Dyspnea Tachycardia Tachypnea Cough Crackles Hemoptysis Small Cell Lung Cancer Large Cell Carcinoma Adenocarcinoma Squamous Cell Carcinoma Smoking ◦ Smokers 13× as Likely to Develop Cancer as Nonsmokers Environmental Tobacco Smoke Other Carcinogens ◦ Asbestos ◦ Arsenic ◦ Pollution None Until Late Productive Cough Recurrent Infection Dyspnea Hemoptysis Anorexia and Weight Loss Pain Wheezing/Stridor Pleural Effusion Superior Vena Cava Syndrome Ectopic Hormone Secretion ◦ ADH (SIADH) ◦ ACTH (Cushing’s Syndrome) Actelectasis Metastasis Chest X-Ray CT Scan Sputum Analysis Biopsy Additional Tests to Find Metastasis Stage (TNM System) Chemotherapy (Usually Palliative) Radiation (Usually Palliative) Pneumonectomy Lobectomy Resection VATS Transplant Monitor Respiratory Status Teach ◦ ◦ ◦ ◦ Routine Preop Teaching What to Expect Visit SICU Include Family Intensive Care Setting Monitor ◦ ◦ ◦ ◦ Vital Signs SaO2, ABGs Hemodynamic Parameters Lung Sounds Ventilator Chest Tubes