Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
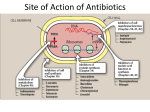
LEARNING OBJECTIVES • Describe the structural relationship of the penicillin molecule with antimicrobial activity. • Explain the mechanism of action of b-lactam antibiotics. • Describe the pharmacokinetic properties of penicillins. • Discuss primary therapeutic indications for penicillin G. • Explain the major side effects of penicillins. • Describe the indications for broad-spectrum penicillins. • List the penicillinase-resistant penicillins. • List the combinations of inhibitors of b-lactamase with Penicillins. CELL WALL SYNTHESIS INHIBITORS • • • • • • • • • INHIBITION OF CELL WALL SYNTHESIS: In contrast to mammalian cell, bacterial cell possesses a rigid outer layer, the cell wall; which completely surrounds the cell membrane. The cell wall consists of cross linkage of peptidoglycans, which forms much thicker layer in gram positive than gram negative bacteria. Bacteria possess high internal osmotic pressure than the mammalian body fluids The intact cell wall prevent movement of mammalian body fluids to inside the bacterium and is responsible for maintaining the shape of bacterium. If the cell wall has been damaged, movement of water into the cell will be followed by swelling, extrusion of the cellular contents through weak areas of the cell wall and cell lysis. Penicillin and cephalosporins are inhibitors of cell wall synthesis. The intact cell wall prevent movement of mammalian body fluids to inside the bacterium and is responsible for maintaining the shape of bacterium. If the cell wall has been damaged, movement of water into the cell will be followed by swelling, extrusion of the cellular contents through weak areas of the cell wall and cell lysis. Penicillin and cephalosporins are inhibitors of cell wall synthesis. CLASSIFICATION β LACTAM ANTIBIOTICS: • PENICILLINS • CEPHALOSPORINS • MONOBACTAMS • AZTREONAM • IMIPENEM OTHER COMPOUNDS: • VANCOMYCIN • BACITRACIN • FOSFOMYCIN PENICILLINS • Penicillins are highly effective antibiotics with high therapeutic index and wide margin of safety. • Penicillin is derived from mould penicillum crysogenum. • 6-amino penicillanic acid (6APA) basic nucleus of all penicillins is composed of thiazolidine ring fused to β lactam ring. An intact nucleus with side chain is essential for the antimicrobial action of penicillin. NATURAL: PENICILLIN- G PENICILLIN- V SEMISYNTHETIC PENICILLINS: ACID RESISTANT: AMPICILLIN AMOXICILLIN OXACILLIN CLOXACILLIN DICLOXACILLIN MECHANISM OF ACTION • Bacterial cell wall consist of complex cross linked polymer, peptidoglycan, consisting of polypeptides and polysaccharides. • Cross linking of polymers is catalyzed by the enzyme transpeptidase. • Penicillin binds with penicillin binding proteins (PBPs), these PBPs are the enzymes required for cross linking of polymers. • Penicillins block transpeptidation (cross-linking) during the final step of cell wall synthesis. • Cell wall synthesis inhibitors are highly effective against rapidly growing bacteria, they are less effective against mature bacteria. • Fluid moves through weak cell wall and to cellular swelling, extrusion of the cellular contents through weak areas of the cell wall and cell lysis. RESISTANCE ♦ Lack of peptidoglycan cell wall ♦ Impermeability of cell wall to penicillin ♦ Presence of enzyme Lactamase : ♦ Increased Lactamase activity ♦ Decreased permeability to drug ♦ Alteration in PBPs ANTIMICROBIAL SPECTRUM • Penicillin G & V are narrow spectrum penicillins, they are effective mainly against Gram-positive organisms, anaerobes and spirochetes. Penicillin G is also effective against meningococci & gonococci. Extended spectrum penicillins are also effective against Gram-negative bacilli. • • PHARMACOKINETICS • On oral administration penicillin G is inactivated in stomach by gastric acid, penicillin V is effective when given orally. Only 30% of Penicillin G is absorbed from gut therefore it is given I/M and I/V. Ampicillin, Amoxicillin, Cloxacillin, Oxacillin are absorbed from gut and are effective orally. Food interferes with absorption of most of acid resistant penicillins except amoxicillin, they should be given 30 minutes before or 2–3 hours after meals. Amoxicillin is rapidly & completely absorbed from gut. After absorption penicillins are widely distributed in the body, but penetration into the eye, prostate and CNS is poor. • • • • • • Normally penicillins do not cross BBB but in presence of meningitis adequate concentrations are found in CSF. • All penicillins crosses placenta, except Ticarcillin none of other penicillins is harmful to fetus, Ticarcillin is C/I in pregnancy. • Penicillins are the drugs of choice in susceptible infections during pregnancy. • 60% of plasma penicillin is bound to plasma proteins. Only small amounts of penicillins are metabolized they are mostly excreted unchanged in urine mainly by tubular secretion (80–85%). • Probenecid decreases tubular secretion of penicillins & prolongs the halflife & duration of action of penicillins. • Nafcillin is the penicillin that is excreted in bile, small amounts of ampicillin are also found in bile. • Procaine penicillin G and Benzathine penicillin G is given by deep I/M injection, serve as depot (Repository) forms. • Major purpose of repository forms is to maintain constant levels of penicillins for prolonged periods. • Repository forms are not suitable for acute infections; they are only used for prophylaxis of infections e.g. rheumatic fever. • Half-life of penicillin-G is 30 minutes, Ampicillin is about 1–1.5 hours, Amoxicillin is about 1.5–2 hours. • THERAPEUTIC USES • Benzyl penicillin is highly effective antimicrobial agent, against susceptible bacteria. • It is the drug of choice for infections caused by streptococci, meningococci, treponema pallidum, clostridia. • Benzathine penicillin is used for prophylaxis of rheumatic fever. • Methicillin, Oxacillin, Cloxacillin, Dicloxacillin are effective against βlactamase producing staphylococci. • Amoxicillin & Ampicillin with β-lactamase inhibitors (Clavulanic acid, tazobactum, sulbactum) are used for infections produced by β-lactamase producing staphylococci. • They are also effective against Gram Negative bacteria. • Amoxicillins are used for the treatment of UTI, sinusitis, pharyngitis, otitis media, pneumonia. • Carbenicillin, Ticarcillin, Azlocillin Pipercillin are effective against pseudomonas. • Penicillins are the drugs of choice for treatment of gonorrhea, syphilis, diphtheria, tetanus. Penicillin is used in prophylaxis of: • Rheumatic fever. • Subacute bacterial endocarditis. • Gonorrhea and syphilis. • Prior to surgery. • Recurrent lymphangitis. • • • Amoxicillins are used for the treatment of UTI, sinusitis, pharyngitis, otitis media, pneumonia. Carbenicillin, Ticarcillin, Azlocillin Pipercillin are effective against pseudomonas. Penicillins are the drugs of choice for treatment of gonorrhea, syphilis, diphtheria, tetanus. Penicillin is used in prophylaxis of: • Rheumatic fever. • Subacute bacterial endocarditis. • Gonorrhea and syphilis. • Prior to surgery. • Recurrent lymphangitis. SIDE EFFECTS • • • • • • HYPERSENSITIVITY (ALLERGIC) REACTIONS DIARRHEA NEUROTOXICITY CATION TOXICITY ACUTE INTERSTITIAL NEPHRITIS PLATELET DYSFUNCTION HYPERSENSITIVITY (ALLERGIC) REACTIONS: • It is the most important side effect of penicillins. reaction to some extent can be avoided by doing subcutaneous sensitivity test. • Penicilloic acid formed during metabolism reacts with proteins and activates immune reaction. • Hypersensitivity reactions range from urticaria to angioedema (marked swelling of lips, tongue and periorbital region) and anaphylaxis and are seen in nearly 5% of the patients receiving penicillins; severe anaphylactic reactions are seen in 0.005% of the patients receiving penicillins. HYPERSENSITIVITY (ALLERGIC) REACTIONS: • Frequency and severity of allergic reactions are governed by route of administration & type of penicillin derivative used. • Topical application is most likely to produce sensitization; most severe forms of allergic reactions are caused by parenteral administration of penicillins, but oral administration & even intradermal injection of minute amounts have produced serious allergic reactions. HYPERSENSITIVITY (ALLERGIC) REACTIONS: • Cross sensitivity among lactam antibiotics occur. • Ampicillin has highest incidence of skin rash and procaine penicillin has highest incidence of allergic reactions among the penicillins. • Maculopopular rash is commonly seen with ampicillin, this is extremely common in-patients with infectious mononucleosis. ACUTE HYPERSENSITIVITY REACTIONS: • Anaphylactic shock occur rapidly within 30 minutes of penicillin administration. It is characterized by urticaria, angioedema, bronchoconstriction & shock. • Death can occur if it is not treated immediately. • Epinephrine, corticosteroids and antihistamines are used to treat anaphylactic shock. DELAYED HYPERSENSITIVITY REACTIONS: • Take more than 2 days to develop, approximately 80 –90% of all allergic reactions occurring with penicillins are of this type. • These reactions are manifested by skin rashes (bullous eruptions), generally these are mild and reversible. • These can also be seen in oral cavity as acute glossitis, brown or black tongue, loss of buccal mucosa after topical use of penicillins in oral cavity or following systemic use of penicillins. • Allergic reactions to penicillins are relatively unpredictable. DELAYED HYPERSENSITIVITY REACTIONS: • Although patients who have experienced an allergic reaction to penicillin is considered allergic unless proved otherwise; challenge tests have shown that 75% of such individuals lose their sensitivity to penicillin with time. • On the other hand patients who have taken penicillins for prolonged periods without any problem may suddenly develop an allergic reaction ranging from mild to severe form. • Patients with personal or familial history of allergy to food, dust, pollens exhibit higher frequency of allergy than the normal individuals. DIARRHEA: • This occurs with agents that are incompletely absorbed from gut. To some extent diarrhea can be reduced by administrating drug ½ -1 hour before meals. NEUROTOXICITY: • This complication is commonly seen with procaine penicillin and is mainly due to procaine. It is also common when penicillins are given intrathecally, epileptic patients are at the risk. CATION TOXICITY: • Penicillins are usually administered as sodium and potassium salts, which may produce cation toxicity. • This can be avoided by using potent agents, which limit the dose of drug. • Sodium toxicity precipitates CCF, and potassium toxicity aggravate the cardiac arrhythmias. • Cation toxicity occur with Carbenicillin and Ticarcillin. METHICILLIN: • Large doses may produce acute interstitial nephritis. CARBENICILLIN AND TICARCILLIN: • They produce platelet dysfunction and may increase bleeding tendencies. Prolonged use of extended spectrum penicillins particularly by oral route can produce super-infections. Accidental I/V injection of repository preparation may result in severe neurovascular damage and pulmonary infarction. OTHER LACTAM DRUGS: MONOBACTAMS (AZTREONAM): • It is monocyclic lactam ring containing compound that is resistant to lactamase. • It is effective against gram negative bacilli including Pseudomonas aeroginosa. • It has no activity against gram positive and anaerobic bacteria. • It is a narrow spectrum antibiotic. MECHANISM OF ACTION: • Aztreonam binds with penicillin binding proteins and disrupt bacterial cell wall synthesis. SIDE EFFECTS: • It is relatively non-toxic. It shows little cross sensitivity with other l a c ta m a n ti b i o ti c s b e c a u s e o f i ts l o w i m m u n o g e n i c p o te n ti a l . Patients sensitive to penicillins tolerate aztreonam very well. • Some times it produces skin rashes and phlebitis. IMIPENEM: • It is active against wide variety of bacteria, including many gram negative, gram positive and anaerobic organisms. • It is resistant to lactamase but is degraded by dihydropeptidases present in renal tubules, resulting in low urinary levels of the drugs. • Drug is usually given with cilastatin, a drug that prevents degradation of Imipenem in renal tubules. MECHANISM OF ACTION: • It binds with PBPs and disrupts bacterial cell wall synthesis. SIDE EFFECTS: • Nausea, vomiting, diarrhea, skin rashes occur frequently. • In high doses drug may produces seizures. Patients allergic to penicillin show hypersensitivity reactions to imipenem. LACTAMASE INHIBITORS: • Antimicrobial activity of lactam antibiotics depends upon the intact lactam ring. Destruction of the ring by acids or lactamase (penicillinase), destroys the antimicrobial activity. • Clavulinic acid, sulbactam and tazobactam contain Lactam ring, have very weak antimicrobial activity. However, they are potent inhibitors of lactamase. They protect the lactam antibiotics from the destruction by lactamase and are often given with penicillins. THANKS











![ch 14 remember thing[1]](http://s1.studyres.com/store/data/008375860_1-2c45a3b285ef35d04828b346253789f0-150x150.png)